Evaluation of Differential Peptide Loading on Tandem Mass Tag-Based Proteomic and Phosphoproteomic Data Quality
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Standard Flow Multiplexed Proteomics (Sflompro) – an Accessible and Cost-Effective Alternative to Nanolc Workflows
bioRxiv preprint doi: https://doi.org/10.1101/2020.02.25.964379; this version posted February 25, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license. Standard Flow Multiplexed Proteomics (SFloMPro) – An Accessible and Cost-Effective Alternative to NanoLC Workflows Conor Jenkins1 and Ben Orsburn2* 1Hood College Department of Biology, Frederick, MD 2University of Virginia Medical School, Charlottesville, VA *To whom correspondence should be addressed; [email protected] Abstract Multiplexed proteomics using isobaric tagging allows for simultaneously comparing the proteomes of multiple samples. In this technique, digested peptides from each sample are labeled with a chemical tag prior to pooling sample for LC-MS/MS with nanoflow chromatography (NanoLC). The isobaric nature of the tag prevents deconvolution of samples until fragmentation liberates the isotopically labeled reporter ions. To ensure efficient peptide labeling, large concentrations of labeling reagents are included in the reagent kits to allow scientists to use high ratios of chemical label per peptide. The increasing speed and sensitivity of mass spectrometers has reduced the peptide concentration required for analysis, leading to most of the label or labeled sample to be discarded. In conjunction, improvements in the speed of sample loading, reliable pump pressure, and stable gradient construction of analytical flow HPLCs has continued to improve the sample delivery process to the mass spectrometer. In this study we describe a method for performing multiplexed proteomics without the use of NanoLC by using offline fractionation of labeled peptides followed by rapid “standard flow” HPLC gradient LC-MS/MS. -

Relative Quantitation of Protein Digests Using Tandem Mass Tags and Pulsed-Q Dissociation (PQD)
Application Note: 452 Relative Quantitation of Protein Digests Using Tandem Mass Tags and Pulsed-Q Dissociation (PQD) Jae Schwartz, Terry Zhang, Rosa Viner, Vlad Zabrouskov, Thermo Fisher Scientific, San Jose, CA, USA Introduction LC Separation and MS Analysis Key Words Quantitation of differentially expressed proteins is one of LC Separation • LTQ XL™ the most challenging areas in proteomics. A variety of HPLC: Thermo Scientific Surveyor equipped with quantitation methods have been developed, including Micro AS autosampler • PQD isotope labeling approaches like ICAT®1, SILAC2, iTRAQ™3, Columns: PicoFrit™ column (10 cm x 75 µm i.d.), (New Objective, Inc., Cambridge, MA) • Proteomics AQUA4, and Tandem Mass Tag® (TMT®)5. In contrast to MS-based quantitation methods, iTRAQ- and TMT-labeled Sample: Inject 2 µL TMT-labeled digest mixture • Quantification peptides are identified and quantitated by MS/MS. Pulsed-Q Mobile Phases: A: 0.1% Formic acid in water B: 0.1% Formic acid in acetonitrile • TMT Dissociation (PQD)6,7 has been developed to facilitate quantitating of the low-mass reporter ions in MS/MS spectra Gradient: 10% B 10 minutes, 10% – 30% in 120 minutes of iTRAQ- or TMT-labeled peptides. The PQD technique Flow: 300 nL/min on column enables the detection of low-mass fragments in MS/MS mode MS Analysis including y1- and b1-type fragment ions, and also allows Mass Spectrometer: Thermo Scientific LTQ XL equipped with a the quantitation of peptides using the TMT reporter ions nanospray ion source 8 which appear in the 100 m/z range. Spray Voltage: 2.0 kV Capillary Temperature: 160 °C Goal Full MS: 300-1600 m/z To demonstrate the benefits of the PQD-based quantitation Isolation: 3 Da of isobarically labeled peptides in protein digests. -
Targeted Quantitative Proteomics Using Selected Reaction Monitoring
Targeted Quantitative Proteomics Using Selected Reaction Monitoring (SRM)- Mass Spectrometry Coupled with an 18O-labeled Reference as Internal Standards Jong-Seo Kim, Errol Robinson, Boyd L. Champion, Brianne O. Petritis, Thomas L. Fillmore, Ronald J. Moore, Liu Tao, David G. Camp II, Richard D. Smith, and Wei-Jun Qian Biological Sciences Division, Pacific Northwest National Laboratory, Richland, WA Methods Results Effect of Q1 resolution Reproducibility 18O labeling efficiency Overview Patient Samples Conclusions Group A: • To address the need of stable isotope Group B: • The utility of 18O-labeled “universal” O area ratio O area Trypsin 18 Red error bars: label-free peak area ratio labeled internal standards for accurate (= each 16O area / average 18O area) reference as internal standards for targeted O/ digestion 16 18 quantification, we introduce the use of an 16 Green error bars: each pair area ratio of O/ O quantitative proteomics has been Patient peptide 18 Pooled reference ratio O area O-labeled reference as comprehensive samples sample 18 successfully demonstrated 16 18 LC-SRM-MS O/ Concentration ratio ( O/ O) internal standards for accurate SRM-MS- 18O labeling 16 – A linear dynamic range of quantification Concen. based quantification instead of using labeled 18 0.01 0.02 0.04 0.1 0.2 1 5 10 25 50 100 4 O-labeled “universal” Ratio ~ 10 in relative concentration synthetic peptides. reference 16O/18O 6.1 12.5 13.7 13.8 5.5 7.7 16.8 2.8 4.6 4.2 1.6 pairs – Better reproducibility than label-free 18 Label • O-labeling efficiency for most peptides is 39.2 23.4 47.5 26.5 19.3 10.6 31.2 3.2 10.7 4.8 3.5 Fig. -

Quantitative Proteomics Reveals the Selectivity of Ubiquitin-Binding Autophagy Receptors in the Turnover of Damaged Lysosomes by Lysophagy
bioRxiv preprint doi: https://doi.org/10.1101/2021.07.19.452535; this version posted July 19, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license. Quantitative proteomics reveals the selectivity of ubiquitin-binding autophagy receptors in the turnover of damaged lysosomes by lysophagy Vinay Eapen1,*, Sharan Swarup1,*, Melissa Hoyer1,*, Joao Paolo1 and J. Wade Harper 1 1Department of Cell Biology, Harvard Medical School, Boston MA 02115 *, Equal Contribution Send correspondence to: [email protected] ABSTRACT Removal of damaged organelles via the process of selective autophagy constitutes a major form of cellular quality control. Damaged organelles are recognized by a dedicated surveillance machinery, leading to the assembly of an autophagosome around the damaged organelle, prior to fusion with the degradative lysosomal compartment. Lysosomes themselves are also prone to damage and are degraded through the process of lysophagy. While early steps involve recognition of ruptured lysosomal membranes by glycan-binding Galectins and ubiquitylation of transmembrane lysosomal proteins, many steps in the process, and their inter-relationships, remain poorly understood, including the role and identity of cargo receptors required for completion of lysophagy. Here, we employ quantitative organelle capture and proximity biotinylation proteomics of autophagy adaptors, cargo receptors, and Galectins in response to acute lysosomal damage, thereby revealing the landscape of lysosomal proteome remodeling during lysophagy. Among proteins dynamically recruited to damaged lysosomes were ubiquitin-binding autophagic cargo receptors. -
Mass Spectrometry and Proteomics Using R/Bioconductor
Mass spectrometry and proteomics Using R/Bioconductor Laurent Gatto CSAMA - Bressanone - 25 July 2019 1 / 40 Slides available at: http://bit.ly/20190725csama These slides are available under a creative common CC-BY license. You are free to share (copy and redistribute the material in any medium or format) and adapt (remix, transform, and build upon the material) for any purpose, even commercially . 2 / 40 On the menu Morning lecture: 1. Proteomics in R/Bioconductor 2. How does mass spectrometry-based proteomics work? 3. Quantitative proteomics 4. Quantitative proteomics data processing and analysis Afternoon lab: Manipulating MS data (raw and identification data) Manipulating quantitative proteomics data Data processing and DE 3 / 40 4 / 40 1. Proteomics and mass spectrometry packages, questions and workow in Bioconductor. 5 / 40 2. How does mass spectrometry work? (applies to proteomics and metabolomics) 6 / 40 Overview 7 / 40 How does MS work? 1. Digestion of proteins into peptides - as will become clear later, the features we measure in shotgun (or bottom-up) proteomics are peptides, not proteins. 2. On-line liquid chromatography (LC-MS) 3. Mass spectrometry (MS) is a technology that separates charged molecules (ions, peptides) based on their mass to charge ratio (M/Z). 8 / 40 Chromatography MS is generally coupled to chromatography (liquid LC, but can also be gas- based GC). The time an analytes takes to elute from the chromatography column is the retention time. 9 / 40 An mass spectrometer is composed of three components: 1. The source, that ionises the molecules: examples are Matrix-assisted laser desorption/ionisation (MALDI) or electrospray ionisation (ESI). -
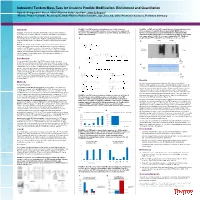
Iodoacetyl Tandem Mass Tags for Cysteine Peptide Modification, Enrichment and Quantitation Ryan D
Iodoacetyl Tandem Mass Tags for Cysteine Peptide Modification, Enrichment and Quantitation Ryan D. Bomgarden 1, Rosa I. Viner 2, Karsten Kuhn 3, Ian Pike 3, John C. Rogers 1 1Thermo Fisher Scientific, Rockford, IL, USA; 2Thermo Fisher Scientific, San Jose, CA, USA; 3Proteome Sciences, Frankfurt, Germany Overview FIGURE 2. iodoTMT reagents and labeling reaction. A) Mechanism of FIGURE 6. cysTMT and iodoTMT reagent labeling of S-nitrosylated proteins. iodoTMT reagent reaction with cysteine -containing proteins or peptides. B) A549 cell lysates (A) and BSA (B) were blocked with MMTS (lanes 1 –8, Purpose: To develop an iodoacetyl Tandem Mass Tag (iodoTMT) reagent for Structure of iodoTMTsixplex reagents for cysteine labeling, enrichment, and 10–15) or untreated (lanes 9, 16) before 500 mM nitro-glutathione (NO) irreversible cysteine peptide labeling, enrichment, and multiplexed quantitation. isobaric MS quantitation. treatment and TMT reagent labeling in the presence or absence of ascorbate and copper sulfate (CuSO ). Proteins were separated by SDS -PAGE and Methods: Reduced sulfhydryls of protein cysteines were labeled with 4 analyzed by anti-TMT antibody Western blotting or Coomassie stain. iodoTMTzero and/or iodoTMTsixplex reagents. Labeled peptides were enriched A using an immobilized anti -TMT antibody resin before mass spectrometry (MS) A cysTMT iodoTMT analysis. 1 2 3 4 5 6 7 8 9 10111213141516 Results: We developed an iodoTMT reagent set to perform duplex isotopic or sixplex isobaric mass spectrometry (MS) quantitation of cysteine-containing peptides. IodoTMT reagents showed efficient and specific labeling of peptide Anti-TMT cysteine residues with reactivity similar to iodoacetamide. Using an anti-TMT Western Blot Cell Lyate antibody, we characterized the immunoaffinity enrichment of peptides labeled with iodoTMT reagents from complex protein cell lysates and for detection of S-nitrosylated cysteines. -

Quantitative Assay of Targeted Proteome in Tomato Trichome
Takemori et al. Plant Methods (2019) 15:40 https://doi.org/10.1186/s13007-019-0427-7 Plant Methods METHODOLOGY Open Access Quantitative assay of targeted proteome in tomato trichome glandular cells using a large-scale selected reaction monitoring strategy Ayako Takemori1, Taiken Nakashima2, Hisashi Ômura3, Yuki Tanaka4, Keisuke Nakata1, Hiroshi Nonami1,5,6 and Nobuaki Takemori4,6* Abstract Background: Glandular trichomes found in vascular plants are called natural cell factories because they synthesize and store secondary metabolites in glandular cells. To systematically understand the metabolic processes in glandular cells, it is indispensable to analyze cellular proteome dynamics. The conventional proteomics methods based on mass spectrometry have enabled large-scale protein analysis, but require a large number of trichome samples for in-depth analysis and are not suitable for rapid and sensitive quantifcation of targeted proteins. Results: Here, we present a high-throughput strategy for quantifying targeted proteins in specifc trichome glandular cells, using selected reaction monitoring (SRM) assays. The SRM assay platform, targeting proteins in type VI trichome gland cells of tomato as a model system, demonstrated its efectiveness in quantifying multiple proteins from a lim- ited amount of sample. The large-scale SRM assay uses a triple quadrupole mass spectrometer connected online to a nanofow liquid chromatograph, which accurately measured the expression levels of 221 targeted proteins con- tained in the glandular cell sample recovered from 100 glandular trichomes within 120 min. Comparative quantitative proteomics using SRM assays of type VI trichome gland cells between diferent organs (leaves, green fruits, and calyx) revealed specifc organ-enriched proteins. Conclusions: We present a targeted proteomics approach using the established SRM assays which enables quantif- cation of proteins of interest with minimum sampling efort. -

Bait Correlation Improves Interactor Identification by Tandem Mass Tag
Bait correlation improves interactor identification by Tandem Mass Tag-Affinity Purification-Mass Spectrometry Liangyong Mei‡,†,a , Maureen R. Montoya‡,a, Guy M. Quanrud a, Minh Tran a, Athena Villa-Sharma a, Ming Huangb, and Joseph C. Genereux a,b* aDepartment of Chemistry, University of California, Riverside, CA 92521 bEnvironmental Toxicology Graduate Program, University of California, Riverside, CA 92521 *To whom correspondence should be addressed: Joseph C. Genereux, 501 Big Springs Rd, Riverside, CA 92507. [email protected], 951-827-3759. 1 ABSTRACT The quantitative multiplexing capacity of isobaric Tandem Mass Tags (TMT) has increased the throughput of affinity purification mass spectrometry (AP-MS) to characterize protein interaction networks of immunoprecipitated bait proteins. However, variable bait levels between replicates can convolute interactor identification. We compared the Student's t-test and Pearson's R correlation as methods to generate t-statistics and assessed the significance of interactors following TMT-AP-MS. Using a simple linear model of protein recovery in immunoprecipitates to simulate reporter ion ratio distributions, we found that correlation-derived t-statistics protect against bait variance while robustly controlling Type I errors (false positives). We experimentally determined the performance of these two approaches for determining t-statistics under two experimental conditions: irreversible prey association to the Hsp40 mutant DNAJB8H31Q followed by stringent washing, and reversible association to 14-3-3z with gentle washing. Correlation-derived t-statistics performed at least as well as Student’s t-statistics for each sample, and with substantial improvement in performance for experiments with high bait level variance. Deliberately varying bait levels over a large range fails to improve selectivity but does increase robustness between runs. -

Novel Insights Into Quantitative Proteomics from an Innovative
Novel Insights into Quantitative Proteomics from an Innovative Bottom-Up Simple Light Isotope Metabolic (bSLIM) Labeling Data Processing Strategy Nicolas Sénécaut, Gelio Alves, Hendrik Weisser, Laurent Lignières, Samuel Terrier, Lilian Yang-Crosson, Pierre Poulain, Gaëlle Lelandais, Yi-Kuo Yu, Jean-Michel Camadro To cite this version: Nicolas Sénécaut, Gelio Alves, Hendrik Weisser, Laurent Lignières, Samuel Terrier, et al.. Novel Insights into Quantitative Proteomics from an Innovative Bottom-Up Simple Light Isotope Metabolic (bSLIM) Labeling Data Processing Strategy. Journal of Proteome Research, American Chemical Society, 2021, 20 (3), pp.1476-1487. 10.1021/acs.jproteome.0c00478. hal-03266586 HAL Id: hal-03266586 https://hal.archives-ouvertes.fr/hal-03266586 Submitted on 21 Jun 2021 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. Distributed under a Creative Commons Attribution - NonCommercial - NoDerivatives| 4.0 International License pubs.acs.org/jpr Article Novel Insights into Quantitative Proteomics from an Innovative Bottom-Up Simple Light Isotope Metabolic (bSLIM) Labeling Data Processing Strategy Nicolas Sénécaut, Gelio Alves, Hendrik Weisser, Laurent Lignieres,̀ Samuel Terrier, Lilian Yang-Crosson, Pierre Poulain, Gaellë Lelandais, Yi-Kuo Yu, and Jean-Michel Camadro* Cite This: J. -

Introduction to Label-Free Quantification
SeqAn and OpenMS Integration Workshop Temesgen Dadi, Julianus Pfeuffer, Alexander Fillbrunn The Center for Integrative Bioinformatics (CIBI) Mass-spectrometry data analysis in KNIME Julianus Pfeuffer, Alexander Fillbrunn OpenMS • OpenMS – an open-source C++ framework for computational mass spectrometry • Jointly developed at ETH Zürich, FU Berlin, University of Tübingen • Open source: BSD 3-clause license • Portable: available on Windows, OSX, Linux • Vendor-independent: supports all standard formats and vendor-formats through proteowizard • OpenMS TOPP tools – The OpenMS Proteomics Pipeline tools – Building blocks: One application for each analysis step – All applications share identical user interfaces – Uses PSI standard formats • Can be integrated in various workflow systems – Galaxy – WS-PGRADE/gUSE – KNIME Kohlbacher et al., Bioinformatics (2007), 23:e191 OpenMS Tools in KNIME • Wrapping of OpenMS tools in KNIME via GenericKNIMENodes (GKN) • Every tool writes its CommonToolDescription (CTD) via its command line parser • GKN generates Java source code for nodes to show up in KNIME • Wraps C++ executables and provides file handling nodes Installation of the OpenMS plugin • Community-contributions update site (stable & trunk) – Bioinformatics & NGS • provides > 180 OpenMS TOPP tools as Community nodes – SILAC, iTRAQ, TMT, label-free, SWATH, SIP, … – Search engines: OMSSA, MASCOT, X!TANDEM, MSGFplus, … – Protein inference: FIDO Data Flow in Shotgun Proteomics Sample HPLC/MS Raw Data 100 GB Sig. Proc. Peak 50 MB Maps Data Reduction 1 -

Comparative Evaluation of Two Isobaric Labeling Tags, Diart and Itraq † ‡ § † ‡ ‡ ‡ ⊥ ¶ ⊥ ¶ Zhen Chen, , , Quanhui Wang, , Liang Lin, Qi Tang, James L
Article pubs.acs.org/ac Comparative Evaluation of Two Isobaric Labeling Tags, DiART and iTRAQ † ‡ § † ‡ ‡ ‡ ⊥ ¶ ⊥ ¶ Zhen Chen, , , Quanhui Wang, , Liang Lin, Qi Tang, James L. Edwards, , Shuwei Li,*, , † ‡ and Siqi Liu*, , † Beijing Institute of Genomics, Chinese Academy of Sciences, Beijing, 101318, China ‡ BGI-Shenzhen, Shenzhen, 518083, China § Graduate University of the Chinese Academy of Sciences, Beijing, 100049, China ⊥ Institute for Bioscience and Biotechnology Research, University of Maryland, Rockville, Maryland 20850, United States ¶ Department of Chemistry and Biochemistry, University of Maryland, College Park, Maryland 20742, United States ABSTRACT: Isobaric tags have broad applications in both basic and translational research, as demonstrated by the widely used isobaric tag for relative and absolute quantitation (iTRAQ). Recent results from large-scale quantitative proteomics projects, however, indicate that protein quantifi- cation by iTRAQ is often biased in complex biological samples. Here, we report the application of another isobaric tag, deuterium isobaric amine reactive tag (DiART), for quantify- ing the proteome of Thermoanaerobacter tengcongensis (T. tengcongensis), a thermophilic bacterium first discovered in China. We compared the performance of DiART with iTRAQ from several different aspects, including their fragmentation mechanisms, the number of identified proteins, and the accuracy of quantification. Our results revealed that, as compared with iTRAQ, DiART yielded significantly stronger reporter ions, which did not reduce the number of identifiable peptides, but improved the signal-to- noise ratio (S/N) for quantification. Remarkably, we found that, under identical chromatography and mass spectrometry (MS) conditions, DiART exhibited less reporter ions ratio compression than iTRAQ, probably due to more reporter ions with higher intensities produced by DiART labeling. -

Development of Tandem Mass Tag Labeling Method for Lipid Molecules Containing Carboxy and Phosphate Groups, and Their Stability in Human Serum
H OH metabolites OH Article Development of Tandem Mass Tag Labeling Method for Lipid Molecules Containing Carboxy and Phosphate Groups, and Their Stability in Human Serum Suzumi M. Tokuoka 1, Yoshihiro Kita 1, Masaya Sato 2 , Takao Shimizu 1,3, Yutaka Yatomi 2 and Yoshiya Oda 1,* 1 Department of Lipidomics, Graduate School of Medicine, The University of Tokyo, Hongo 7-3-1, Bunkyo-ku, Tokyo 113-8654, Japan; [email protected] (S.M.T.); [email protected] (Y.K.); [email protected] (T.S.) 2 Department of Clinical Laboratory Medicine, Graduate School of Medicine, The University of Tokyo, Hongo 7-3-1, Bunkyo-ku, Tokyo 113-8654, Japan; [email protected] (M.S.); [email protected] (Y.Y.) 3 Department of Lipid Signaling, National Center for Global Health and Medicine, Toyama 1-21-1, Shinjuku-ku, Tokyo 162-8655, Japan * Correspondence: [email protected]; Tel.: +81-3-5841-3540 Abstract: In clinical lipidomics, it is a challenge to measure a large number of samples and to reproduce the quantitative results. We expanded the range of application of the tandem mass tag (TMT) method, which is widely used in proteomics, to lipidomic fields. There are various types of lipid molecule, for example, eicosanoids have a carboxyl group and phosphatidic acid has a phosphate group. We modified these functional groups simultaneously with TMT. This approach allows for a single analysis by mixing six samples and using one of the six samples as a bridging sample; the quantitative data can be easily normalized even if the number of measurements increases.