A Glow of HLA Typing in Organ Transplantation Batool Mutar Mahdi
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Population Genetics and Anthropology
Abstracts S24 Poster Group 7 - Immune Regulation 94 HUMORAL AND CELLULAR IMMUNE RESPONSE 93 MECHANISMS DIRECTED AGAINST THE FETUS SUPERIOR T CELL SUPPRESSION BY RAPAMYCIN+FK506, CONTRIBUTE TO PLACENTAL ABRUPTION. OVER RAPAMYCIN+CSA, DUE TO ABROGATED CTL INDUCTION, IMPAIRED MEMORY RESPONSES AND Andrea Steinborn, Cyrus Sayehli, Christoph Sohn, Erhard Seifried, PERSISTENT APOPTOSIS Edgar Schmitt, Manfred Kaufmann, Christian Seidl. Department of Obstetrics and Gynecology, University of Frankfurt; Hans JPM Koenen, Etienne CHJ Michielsen, Jochem Verstappen, Institute of Immunology, University of Mainz; Department of Esther Fasse and Irma Joosten. Department for Blood Transfusion Transplantation Immunology, RCBDS, Germany and Transplantation Immunology, University Medical Center Placental abruption is an unpredictable severe complication in Nijmegen, The Netherlands. pregnancy. In order to investigate the possibility that the activation Immunosuppressive therapy is best achieved with a combination of agents of the fetal non-adaptive immune system may be involved in the targeting multiple activation steps of T-cells. In transplantation, Cyclosporin-A pathogenesis of this disease, IL-6 release from cord blood (CsA) or Tacrolimus (FK506) are successfully combined with Rapamycin monocytes was examined by intracellular cytokine staining and (Rap). Rap and CsA were first considered for combination therapy because flow cytometric analysis. Our results demonstrate that preterm FK506 and Rap target the same intracellular protein and thus may act in an antagonistic way. However, in clinical studies FK506+Rap proved to be placental abruption (n=15) in contrast to uncontrollable preterm effective. To date, there is no in vitro data supporting these in vivo findings and labour (n=33) is associated with significantly (p<0.001) increased it is unclear whether the observed effects are T cell mediated. -
Tissue Typing: HLA Typing and Screening
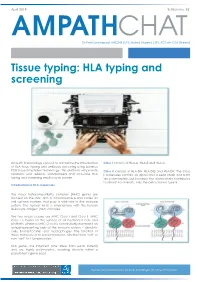
April 2019 Edition no. 55 CHAT Dr Petri Swanepoel, MBChB (UP), MMed (Haem) (UP), FCPath (SA) (Haem) Tissue typing: HLA typing and screening Ampath Immunology is proud to announce the introduction Class I consists of HLA-A, HLA-B and HLA-C. of HLA tissue typing and antibody screening using Luminex PCR-based multiplex technology. This platform will provide Class II consists of HLA-DR, HLA-DQ and HLA-DP. The Class clinicians with reliable, standardised and accurate HLA II molecules contain an alpha and a beta chain and both typing and screening results much sooner. are polymorphic, but because the alpha chain contributes to almost no diversity, only the beta chain is typed. Introduction to HLA molecules The major histocompatibility complex (MHC) genes are located on the short arm of chromosome 6 and codes for cell surface markers that play a vital role in the immune system. The human MHC is synonymous with the human leukocyte antigen (HLA) complex. The two major classes are MHC Class I and Class II. MHC Class I is found on the surface of all nucleated cells and platelets, whereas MHC Class II is constitutively expressed on antigen-presenting cells of the immune system – dendritic cells, B-lymphocytes and macrophages. The function of these molecules is to present proteins, whether from “self’ or non-“self” to T-lymphocytes. HLA genes are inherited (one allele from each parent) and are highly polymorphic, creating diversity within a population’s gene pool. Please contact your local Ampath pathologist for more information. April 2019 Edition no. 55 HLA typing Donor-specific antibodies have become an established biomarker, predicting the risk for antibody-mediated rejection. -

Immunology-Transplantation.Pdf
Transplantation Renal block second lecture Brought to you by: Hossam al-shehri Ibrahim al-qasir Bayan Al-Amr Lama Al-Faraidi o Objectives: To understand the diversity among human leukocyte antigens (HLA) or major histo-compatibility complex (MHC) To know the role of HLA antigens in transplant rejection To be familiar with types of immune responses mediating transplant rejections and importance of tissue matching To understand the principles of management after transplantation Black : Slides Purple : Extra notes for further understanding Orange: Notes said by the doctor Red : important 432 Immunology Team Major Histocompatibility Complex and Transplantation • Major histocompatibility complex (MHC) proteins were discovered for the first time with the advent of tissue transplantation • The success of tissue and organ transplantation depends upon the donor’s and recipient’s “human leukocyte antigens” (HLA) encoded by HLA genes . • Human Leukocyte antigen system = Major histocompatibility Complex in humans. Cause Major Histocompatibility complex genes found in different species like mammals for example. • These proteins are allo-antigens(Allo-antigens are antigens from members of the same species.) • Genes for HLA proteins are clustered in the MHC complex located on the short arm (p arm)of chromosome 6 • MHCs or HLAs are different between one person and another, so in transplantation they will act as a foreign antigen in the recipient body, and an immune response will be directed against those bodies this is known as rejection. Unless the HLAs collection is a bit similar like in siblings or exactly 432 Immunology Team the same like in identical twins. For Further understanding: MHC Class 1: are glycoproteins that will appear on both antigen presenting cells and nucleated cells for example, RBCs are not nucleated so there is no MHC. -

HLA Diagnostic Sequencing ± Conception, Application and Automation
Transfusions- und Tranplantationsmedizin Redaktion: Mariam Klouche HLA Diagnostic Sequencing ± Conception, Application and Automation Diagnostische HLA-Sequenzierung ± Konzept, Anwendung und Automatisierung R. Blasczyk Summary: Sequencing gives the most reliable and ac- 2-digit HLA typing, a gene-specific amplification curate information of the DNA sequence of a gene and approach for sequencing of both alleles simultaneously is therefore of particular interest for fully characterising should be applied. Thus, the progress made in diagnos- the genetic complexity and allelic diversity of the HLA tic HLA sequencing now offers a real alternative to the genes. The full complexity of allelic diversity in HLA conventional molecular typing techniques, and will in- class Iand class IIgenes,as well as recent improve- creasingly replace them for the patients' benefit. ments in the convenience and quality of automated se- quencing, makes sequencing the method of choice for Keywords: HLA analysis; sequencing; automation. HLA low- and high-resolution typing. HLA typing by means of sequencing should be done whenever the Zusammenfassung: Die Sequenzierung liefert die HLA type of an individual is needed. The current devel- zuverlaÈssigste und genaueste Information uÈber die opments with regard to HLA-sequencing systems, se- DNA-Sequenz eines Gens und ist daher fuÈr die Charak- quencing instruments and software solutions for data in- terisierung der genetischen KomplexitaÈt und allelischen terpretation have made sequencing equally simple and Vielfalt der HLA-Gene von besonderem Interesse. Die robust, providing formats for each level of throughput hohe KomplexitaÈt der allelischen DiversitaÈt der HLA and automation in order to match each laboratory's in- Klasse Iund IIGeneund die aktuellen Verbesserungen dividual requirements. -
Understanding the Immune System How It Works
Understanding the Immune System How It Works U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES NATIONAL INSTITUTES OF HEALTH National Institute of Allergy and Infectious Diseases Artwork by Jeanne Kelly Understanding the Immune System How It Works U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES NATIONAL INSTITUTES OF HEALTH National Institute of Allergy and Infectious Diseases NIH Publication No. 07-5423 September 2007 www.niaid.nih.gov Contents 1 Introduction 2 Self and Nonself 3 The Structure of the Immune System 7 Immune Cells and Their Products 19 Mounting an Immune Response 25 Immunity: Natural and Acquired 28 Disorders of the Immune System 34 Immunology and Transplants 35 The Immune System and the Nervous System 36 Frontiers in Immunology 42 Summary 43 Glossary Note: Words in bold are defined in the glossary at the end of this booklet. Introduction he immune system is a network of cells, Ttissues, and organs that work together to defend the body against attacks by “foreign” invaders. These are primarily microbes—tiny organisms such as bacteria, parasites, and fungi that can cause infections. Viruses also Bacteria: streptococci cause infections, but are too primitive to be classified as living organisms. The human body provides an ideal environment for many microbes. It is the immune system’s job to keep them out or, failing that, to seek out and destroy them. Virus: When the immune system hits the wrong herpes virus target, however, it can unleash a torrent of disorders, including allergic diseases, arthritis, and a form of diabetes. If the immune system is crippled, other kinds of diseases result. -

The Pharmacogenomic HLA Biomarker Associated to Adverse Abacavir Reactions: Comparative Analysis of Different Genotyping Methods
314 Current Genomics, 2012, 13, 314-320 The Pharmacogenomic HLA Biomarker Associated to Adverse Abacavir Reactions: Comparative Analysis of Different Genotyping Methods Laura Stocchi1, Raffaella Cascella1, Stefania Zampatti1, Antonella Pirazzoli2, Giuseppe Novelli3,4 and Emiliano Giardina*,1 1Università degli Studi di Roma Tor Vergata, Centro di Eccellenza per lo Studio del Rischio Genomico in Patologie Complesse Multifattoriali, Roma, Italy; 2ViiV Healthcare, Verona, Italy, 3Agenzia di Valutazione del Sistema Universitario e della Ricerca (ANVUR), 4Ospedale San Pietro, Fatebenefratelli, Roma, Italy Abstract: Many pharmacogenomic biomarkers (PGBM) were identified and translated into clinical practice, affecting the usage of drugs via label updates. In this context, abacavir is one of the most brilliant examples of pharmacogenetic studies translated into clinical practice. Pharmacogenetic studies have revealed that abacavir HSRs are highly associated with the major histocompatibility complex class I. Large studies established the effectiveness of prospective HLA-B*57:01 screening to prevent HSRs to abacavir. Accordingly to these results the abacavir label has been modified: the European Medicines Agency (EMA) and the FDA recommend/suggested that the administration of abacavir must be preceded by a specific genotyping test. The HLA locus is extremely polymorphic, exhibiting many closely related alleles, making it difficult to discriminate HLA-B*57:01 from other related alleles, and a number of different molecular techniques have been developed recently to detect the presence of HLA-B*57:01. In this review, we provide a summary of the available techniques used by laboratories to genotype HLA-B*57:01, outlining the scientific and pharmacoeconomics pros and cons. Received on: December 23, 2011 - Revised on: March 09, 2012 - Accepted on: March 31, 2012 Keywords: HLA-B*57:01, abacavir, hypersensitivity reaction (HSR), pharmacogenomics. -

Poster Group 12
Abstracts S56 217 218 PHARMACODYNAMIC MONITORING OF IMMUNO- SIMULTANEOUS HEPATO-RENAL TRANSPLANTATION SUPPRESSIVE THERAPY WITH CALCINEURIN INHIBITORS WITH A POSITIVE CROSSMATCH IN SENSITIZED PATIENTS. Jaume Martorell 1,Olga Millán1; Merce Brunet2; Josep-Maria Campistol3; Ana Jaume Martorell, Marta Crespo, Vicente Torregrosa, Alejandro Faura3; Isabel Rojo1; Elena Vidal2; Olga Jiménez2; Federic. Oppenheimer3; Gutierrez, Federic Openheimer, Jordi Vives. Institut Clinic Jordi Vives1; Institut Clinic d’Infeccions i Immunologia (ICII)1, Servei de Toxicologia2, Unitat de Transplantament Renal3, IDIBAPS, Hospital Clinic, d’Infeccions i Immunologia (ICII), Unitat de Transplantament Renal, 08036 Barcelona, Spain IDIBAPS, Hospital Clinic, 08036 Barcelona, Spain Background: Graft survival depends on immunosuppressors efficacy. Introduction: A positive crossmatch (CM+) is a formal contraindication for Pharmacodynamic parameters are needed to evaluate individual biological effect and isolated renal transplantation but is not a contraindication for liver to complement pharmacokinetics, specially in multidrug low toxicity transplantation. It has been said that in simultaneous Hepato-Renal immunosuppressive therapies which include Calcineurin Inhibitors (CNi). transplantation (SHRT) the liver protects the kidney from rejection. In our Methods: Patients: 65 stable renal transplant recipients treated with: Cyclosporine-A center 21 SHRT had been performed since 1993, 2 of them with CM+. (CsA)(n=16), Tacrolimus (TRL)(n=10); Cyclosporine-A plus Mycophenolate-Mofetil Aim of the study: Retrospective analysis of two cases of SHRT with CM+. (CsA+MMF)(n=14); Tacrolimus plus Mycophenolate-Mofetil (TRL+MMF)(n=13) Patients and methods: 2 women (30 & 52 years) with hepatic cirrhosis VHC in and Mycophenolate-Mofetil (MMF)(n=12). Non-treated normal healthy controls hemodialysis after a first renal transplant failure, with Panel Reacting (NHC)(n=12). -
Rapid, Scalable and Highly Automated HLA Genotyping Using Next
Danzer et al. BMC Genomics 2013, 14:221 http://www.biomedcentral.com/1471-2164/14/221 METHODOLOGY ARTICLE Open Access Rapid, scalable and highly automated HLA genotyping using next-generation sequencing: a transition from research to diagnostics Martin Danzer1*†, Norbert Niklas1†, Stephanie Stabentheiner2, Katja Hofer1, Johannes Pröll1, Christina Stückler1, Edeltraud Raml1, Helene Polin1 and Christian Gabriel1 Abstract Background: Human leukocyte antigen matching at allelic resolution is proven clinically significant in hematopoietic stem cell transplantation, lowering the risk of graft-versus-host disease and mortality. However, due to the ever growing HLA allele database, tissue typing laboratories face substantial challenges. In light of the complexity and the high degree of allelic diversity, it has become increasingly difficult to define the classical transplantation antigens at high-resolution by using well-tried methods. Thus, next-generation sequencing is entering into diagnostic laboratories at the perfect time and serving as a promising tool to overcome intrinsic HLA typing problems. Therefore, we have developed and validated a scalable automated HLA class I and class II typing approach suitable for diagnostic use. Results: A validation panel of 173 clinical and proficiency testing samples was analysed, demonstrating 100% concordance to the reference method. From a total of 1,273 loci we were able to generate 1,241 (97.3%) initial successful typings. The mean ambiguity reduction for the analysed loci was 93.5%. Allele assignment including intronic sequences showed an improved resolution (99.2%) of non-expressed HLA alleles. Conclusion: We provide a powerful HLA typing protocol offering a short turnaround time of only two days, a fully integrated workflow and most importantly a high degree of typing reliability. -
Tissue Typing
Tissue Typing Tissue Typing The transplant of organs and tissues is one of the greatest curative achievements of this century. In organ transplantation, the adaptive immunity is considered the main response exerted to the transplanted tissue, since the main goal of the immune response is the MHC (major histocompatibility complex) molecules expressed on the surface of donor cells. Cell surface molecules that induce an antigenic stimulus cause the rejection immune response to grafted tissue or organ. A wide variety of transplantation antigens have been described, including the major histocompatibility molecules, minor histocompatibility antigens, ABO blood group antigens and endothelial cell antigens. The sensitization to MHC antigens may be caused by transfusions, pregnancy, or failed previous grafts leading to development of anti-human leukocyte antigen (HLA) antibodies that are important factor responsible for graft rejection in solid organ transplantation and play a role in post- transfusion complication, Anti-HLA Abs may be present in healthy individuals. Methods for HLA typing are described, including serological methods, molecular techniques of sequence-specific priming (SSP), sequence-specific oligonucleotide probing (SSOP); Sequence based typing (SBT) and reference strand-based conformation analysis (RSCA) method. Problems with organ transplantation are reservoir of organs and immune suppressive treatments that used to decrease rate of rejection with less side effect and complications. 1 Tissue Typing In the past, it was difficult to tell exactly whether an organ or tissue, such as a kidney, lung or bone marrow, was an exact match for the transplant between a donor and recipient. If it was not, a serious rejection reaction could sometimes occur between the recipient patient and the transplanted organ. -

Advances in Transplantation Immunology Vancouver, September 1 and 2 , 2015 Next Generation Sequencing, Epitope Analysis And
Advances in Transplantation Immunology st nd Vancouver, September 1 and 2 , 2015 Next Generation Sequencing, Epitope Analysis and MHC A ntibodies in Organ and Stem Cell Transplantation Cutting-edge innovations for clinical, laboratory and research teams: Advances in gene sequencing and proteomics; Role of HLA in human disease: NGS typing of HLA and other MHC genes; Epitope analysis and matching; Measurement and interpretation of complex HLA antibodies; Clinical implication of new methods for transplantation matching and management; Introducing new technologies to the clinical laboratory; and Bioinformatics analysis of NGS and epitope data. Plenary speakers include: Dr. Henry Erlich, Roche Discovery Research and Human Genetics, Dr. Rene Duquesnoy, Professor Emeritus, University of Pittsburgh. Space for this symposium is strictly limited. To confirm your registration please contact: www.vchri.ca/ngssymposium Vancouver Coastal Health Research Institute Vancouver General Hospital 604-875-4111 x 67793 st Advances in Transplantation Immunology: Day 1, September 1 Next Generation Sequencing (NGS) offers enormous potential to enhance the field of HLA typing, through precise determination of nucleotide sequences across the full length of the human genes, phase resolution to minimize ambiguity, multiplexing for scalable analysis, and high-throughput via laboratory automation. Introduction of NGS to the clinical laboratory brings specific challenges including computing support and data storage, computational analysis and bioinformatics, and the limitations of reference data in current repositories. This symposium will address these issues in preparation for the advent of this new technology. 8.00 am Breakfast Meet and Mix, Exhibits Session 1: 9.00 – 10.30 NGS and HLA (part 1). Chairs: K. Tinckam and N. -

The Long and Winding Road Towards Epitope Matching in Clinical Transplantation
Transplant International REVIEW The long and winding road towards epitope matching in clinical transplantation Cynthia S.M. Kramer1, Moshe Israeli2, Arend Mulder1, Ilias I.N. Doxiadis3, Geert W. Haasnoot1, Sebastiaan Heidt1 & Frans H.J. Claas1 1 Department of SUMMARY Immunohaematology and Blood Recent data suggest that HLA epitope matching is beneficial for the pre- Transfusion, Leiden University vention of de novo donor specific antibody (DSA) formation after trans- Medical Center, Leiden, the plantation. In this review, different approaches to predict the Netherlands immunogenicity of an HLA mismatch will be discussed. The parameters 2 Tissue Typing Laboratory, Rabin Medical Center, Petach-Tikva, Israel used in these models are often called epitopes but the actual antibody epi- 3 Institut fur€ Transfusionsmedizin, tope is far more complex. Exact knowledge of the antibody epitope is cru- Universitatsklinikum€ Leipzig, Leipzig, cial if epitope matching is also used as a tool to select compatible donors Germany for (highly) sensitized patients. Evidence is provided that it is not always possible to give an exact definition of an antibody epitope. We conclude Correspondence that HLA “epitope” matching is superior over HLA antigen matching with Frans H.J. Claas, Department of respect to the prevention of de novo DSA formation and will enhance the Immunohematology and Blood prediction of acceptable HLA mismatches for sensitized patients. However, transfusion, Leiden University Medical epitope matching at our current level of knowledge will not solve all histo- Center, Albinusdreef 2, 2333 ZA compatibility problems as unexpected antibody reactivity still may occur. Leiden, The Netherlands. Tel.: +31 71 5263802; Fax: +31 71 5265267; Transplant International 2019; 32: 16–24 e-mail: [email protected] Key words antibodies, epitopes, HLA matching, immunogenicity, virtual crossmatch Received: 13 March 2018; Revision requested: 16 April 2018; Accepted: 10 October 2018; Published online: 26 November 2018 the enormous polymorphism of the HLA system. -
Instructions for Use
Product no: 511.21 Batch no: TK0057 Primer Lot no: 523-x DynaMix PlusTM no: R0847 Expiry date: 2007-05 Size: 20 tests Instructions For Use Dynal AllSet+™ Minor Histocompatibility Antigen (mHA) Typing Kit For Research Use Only INSTRUCTIONS FOR USE Dynal AllSet+™ Minor Histocompatibility Antigen (mHA) Typing Kit CONTENTS Page INTENDED USE…………………………………………………………………………..….………………………………… 3 SUMMARY AND EXPLANATION…….........………………...………………………………………………………. 3 PRINCIPLES OF THE PROCEDURE ……………………………...............……………..………………………… 3 REAGENTS.........................................................…................…………...….…………………………… 4 Provided in Typing kit ……...………………………………..……….……………………………………….. 4 Storage ………………………………………………………………..……..…………..………………………….. 4 WARNINGS AND PRECAUTIONS ………………………………………………….…………………………………. 5 EQUIPMENT REQUIRED BUT NOT PROVIDED BY DYNAL ……….…………………………………………. 5 PROCEDURE ...........……………………………….……………………………………….….…………………………… 6 Sample Collection and Preparation.........................………………………………………… 6 PCR Amplification Set-up ........................…...................………...……………………… 6 PCR Amplification .................................……………………...........………………………… 7 PCR Detection using agarose gel electrophoresis ……………………………………………. 8 INTERNAL CONTROLS .................................……........…...……………………………….………… 9 Internal Positive Control ………………………………………………………………………………. 9 Integrated Negative Control well ……………………………………………………………........ 9 INTERPRETATION ….……………………………………………………………………………………………………… 10 TROUBLESHOOTING GUIDE