Ocean Studies Institute AAUS Scientific Diving Course Application Package
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Drag Levels and Energy Requirements on a SCUBA Diver
Loughborough University Institutional Repository Drag levels and energy requirements on a SCUBA diver This item was submitted to Loughborough University's Institutional Repository by the/an author. Citation: PASSMORE, M.A and RICKERS, G., 2002. Drag levels and energy requirements on a SCUBA diver. Journal of Sports Engineering, 5(4), pp. 173- 182. Additional Information: • The final publication is available at www.springerlink.com. Metadata Record: https://dspace.lboro.ac.uk/2134/6649 Version: Accepted for publication Publisher: Springer ( c International Sports Engineering Association (ISEA)) Please cite the published version. This item was submitted to Loughborough’s Institutional Repository (https://dspace.lboro.ac.uk/) by the author and is made available under the following Creative Commons Licence conditions. For the full text of this licence, please go to: http://creativecommons.org/licenses/by-nc-nd/2.5/ Drag levels and Energy Requirements on a SCUBA Diver. M.A. Passmore, G Rickers Loughborough University Department of Aeronautical and Automotive Engineering ABSTRACT The popularity of sport diving has increased rapidly since its inception in the 1950’s. Over this period, the trend has been to increase the amount of equipment carried by the diver. There are many undoubted safety advantages associated with the additional kit, but under some conditions, it can impose an additional burden in the form of increased drag. The purpose of this paper is to identify the drag penalties for a number of simple SCUBA configurations. This is achieved through scale model experiments conducted in a wind tunnel. Some comments on the associated energy requirements are made, and from these, the effect on a diver’s bottom time is briefly addressed. -

2.4.3 Underwater Cave Survey
2.4.3 Underwater Cave Survey 2.4.3.1 Course Outcomes GUE’s Underwater Cave Survey course is designed to introduce experienced cave divers to the important skill of surveying underwater caves. Among the course’s intended outcomes are: introducing divers to the basic principles of underwater cave survey, the implementation of a defined team approach to underwater survey data collection, preparing an experienced cave diver to productively assist in a coordinated cave project, and introducing divers to cartography methods. 2.4.3.2 Prerequisites Applicants for an Underwater Cave Survey course must: a. Submit a completed Course Registration Form, Medical History Form, and Liability Release to GUE HQ. b. Hold insurance that will cover diving emergencies, such as hyperbaric treatment, e.g., DAN Master-level insurance or equivalent. c. Be physically and mentally fit. d. Be a nonsmoker. e. Obtain a physician’s prior written authorization for the use of prescription drugs, except for birth control, or for any medical condition that may pose a risk while diving. f. Be a minimum of 18 years of age. Documented parental or legal guardian consent must be submitted to GUE HQ when the participant is a minor. g. Be a certified GUE Cave Diver Level 2 diver. h. Have completed at least 25 non-training Cave 2 dives beyond GUE Cave Diver Level 2 certification. 2.4.3.3 Course Content The Underwater Cave Survey course is normally conducted over five days. It requires a minimum of ten diving hours and at least forty hours of instruction, encompassing classroom lectures, land drills, and in-water work. -

General Training Standards, Policies, and Procedures
General Training Standards, Policies, and Procedures Version 9.2 GUE General Training Standards, Policies, and Procedures © 2021 Global Underwater Explorers This document is the property of Global Underwater Explorers. All rights reserved. Unauthorized use or reproduction in any form is prohibited. The information in this document is distributed on an “As Is” basis without warranty. While every precaution has been taken in its preparation, neither the author(s) nor Global Underwater Explorers have any liability to any person or entity with respect to any loss or damage caused or alleged to be caused, directly or indirectly, by this document’s contents. To report violations, comments, or feedback, contact [email protected]. 2 GUE General Training Standards, Policies, and Procedures Version 9.2 Contents 1. Purpose of GUE .............................................................................................................................................6 1.1 GUE Objectives ............................................................................................................................................. 6 1.1.1 Promote Quality Education .................................................................................................................. 6 1.1.2 Promote Global Conservation Initiatives .......................................................................................... 6 1.1.3 Promote Global Exploration Initiatives ............................................................................................. 6 -

Safe Boating Guidelines
DIVE FLAGS HEALTH & DIVING REFERENCE SERIES When diving, fly the flag. Ensure the flags are stiff, 6 West Colony Place unfurled and in recognizable condition. Durham, NC 27705 USA SAFE BOATING PHONE: +1-919-684-2948 DIVER DOWN FLAG DAN EMERGENCY HOTLINE: +1-919-684-9111 GUIDELINES This flag explicitly signals that divers are in the water and should always be flown from a vessel or buoy when divers are in the water. When flown from a vessel, the diver down flag should be at least 20 inches by 24 inches and flown above the vessel’s highest point. When displayed from a buoy, the flag should be at least 12 inches by 12 inches. ALPHA FLAG Internationally recognized, this flag is flown when the mobility of a vessel is restricted, indicating that other vessels should yield the right of way. The alpha flag may be flown along with the diver down flag when divers are in the water. D SURFACE MARKER BUOYS I V When deployed during ascent, a E surface marker buoy (SMB) will make R a diver’s presence more visible. In B addition to a SMB, divers may also E L use a whistle or audible signal, a dive O light or a signaling mirror to notify W boaters of their location in the water. Part #: 013-1034 Rev. 3.27.15 REPORT DIVING INCIDENTS ONLINE AT DAN.ORG/INCIDENTREPORT. JOIN US AT DAN.ORG SAFE BOATING GUIDELINES To prevent injuries and death by propeller and vessel strikes, divers and boaters must be proactively aware of one another. -

9. Extended Range Diver
TDI Standards and Procedures Part 2: TDI Diver Standards 9. Extended Range Diver 9.1 Introduction This course provides training and experience required to competently utilize air for dives up to 55 metres / 180 feet that requires staged decompression, utilizing nitrox mixtures or oxygen during decompression. The objective of this course is to train divers in the proper techniques, equipment requirements, and hazards of deep air diving to a maximum of 55 metres / 180 feet utilizing nitrox mixtures or oxygen for staged decompression. 9.2 Qualifications of Graduates Upon successful completion of this course, graduates may engage in decompression diving activities without direct supervision provided: 1. The diving activities approximate those of training 2. The areas of activities approximate those of training 3. Environmental conditions approximate those of training Upon successful completion of this course, graduates are qualified to enroll in: 4. TDI Advanced Wreck Course 5. TDI Trimix Course 6. TDI Advanced Trimix Course 9.3 Who May Teach This course may be taught by any active TDI Extended Range Instructor 9.4 Student to Instructor Ratio Academic 1. Unlimited, so long as adequate facility, supplies and time are provided to ensure comprehensive and complete training of subject matter Confined Water (swimming pool-like conditions) 1. N/A Open Water (ocean, lake, quarry, spring, river or estuary) 1. A maximum of 4 students per instructor; it is the instructor’s discretion to reduce this number as conditions dictate Version 0221 75 TDI Standards and Procedures Part 2: TDI Diver Standards 9.5 Student Prerequisites 1. Minimum age 18 2. -

Belize Dive-Kit List
Blue Ventures Belize Dive-Kit List Last updated May 2014 Contents Introduction ...................................................................................................................................... 1 Essential Items .................................................................................................................................. 2 PADI Manuals & Materials ............................................................................................................. 2 Open Water Course ................................................................................................................... 2 Advanced Open Water Course ................................................................................................... 2 EFR ............................................................................................................................................ 2 Rescue Diver .............................................................................................................................. 3 Divemaster ................................................................................................................................ 3 Log Books .................................................................................................................................. 3 Mask ............................................................................................................................................. 3 Snorkel ......................................................................................................................................... -

Best Diving Practice Guidelines*
Appendix 1. Best Diving Practice Guidelines* A1.1 Divers should terminate the dive while there is still sufficient cylinder pressure to permit them to safely reach the surface and return to shore or boat, including allowing for any decompression time or planned safety stops. A1.2 The dive team should not include a diver who for any reason is not physically or psychologically fit at the time of the dive; or whose dive equipment is not in a safe operating condition in the opinion of the nominated dive leader. A1.3 All dives, including repetitive dives, should preferably be calculated using DCIEM tables (Canadian Defence and Civil Institute for Environmental Medicine), but the use of well-maintained dive computers is acceptable. A1.4 Divers should do a safety stop at 5 m depth for at least 3 minutes immediately before surfacing at the end of each dive where the average depth exceeded 7 metres or the maximum depth exceeded 10 metres. A1.5 If a dive does extend beyond the no-decompression limits, divers should remain awake for at least 1 hour after diving and remain in the company of another person prepared to assist with medical intervention if required. A1.6 Divers should adhere to the buddy system as taught in their dive training. This buddy system is based upon mutual assistance, especially in an emergency. A1.7 If a volunteer diver becomes separated from their buddy: a) the diver shall do a 360-degree search for a maximum of 1 minute looking for bubbles or visual sign of the other diver b) if the lost diver is not located, the searching diver shall return to the surface at the correct ascent rate, still performing the 360-degree search on ascent c) the searching diver will deploy a safety surface marker buoy, use a whistle (or ask where the lost diver is) and wait on surface for 4 minutes d) if the lost diver is still missing, divers are to return to their boat or shore and initiate emergency procedures by contacting emergency services. -

Diving, Retail & Service Price List 2018
DIVING PRICE LIST DIVING Description Price Shore Dive 1 guided shore dive in Flying Fish Cove or Ethel Beach $65 Boat Dive 1 boat dive, including weights, air tank and boat $139 Double Tank Dive 2 boat dives, including weights, air tanks and boat $205 Boat Passenger 1 boat passenger fee for double tank dive $30 Special Trip Surcharge Long distance fuel surcharge for southwest or south side of $75 island (min 4 divers) Night or Early Morning Surcharge for a night dive or early morning dive from the $38 Surcharge boat, including guide (min 4 divers) Scuba Skills Update Refresher dive, including theory session, shallow water skill $169 practice, dive equipment and 1 shore dive with an instructor Private Guide Private guide per dive, max 2 persons per guide $98 EANX 32% Fill Nitro 32% per tank $8 DIVING PACKAGES Description Price 3-Day Dive Package Total 6 dives, 2 per day, including weights, air tanks and $595 boat. Package is per person and cannot be shared. 7th, 8th & 9th Dive Extra dive to 3-day dive package per dive $99 5-Day Dive Package Total 10 dives, 2 per day, including weights, air tanks and $970 boat. Package is per person and cannot be shared. 11th Dive Onwards Extra dive to the 5-day dive package per dive $97 DIVE GEAR RENTAL Description Price BCD, Regulator, Short Price per single item per day hired $9 Wetsuit, Dive Computer Equipment Package 1 BCD, regulator, short wetsuit and dive computer per day $29 Equipment Package 2 BCD, regulator, long wetsuit and dive computer per day $35 Long Wetsuit Long 5mm Wetsuit per day $15 Surface Marker Buoy Mandatory for all diving. -

Dive Kit List
Dive Kit List Last updated July 2015 blueventures.org Contents Introduction ............................................................................................................................................ 2 Essential Items ........................................................................................................................................ 2 PADI Manuals & Materials .................................................................................................................. 2 Advanced Open Water Course ........................................................................................................ 2 Log Books ........................................................................................................................................ 2 Mask .................................................................................................................................................... 2 Snorkel ................................................................................................................................................ 2 Fins ...................................................................................................................................................... 3 Dive Boots/booties ............................................................................................................................. 3 ........................................................................................................................................................... -

2018 September;48(3):132−140
Diving and Hyperbaric Medicine The Journal of the South Pacific Underwater Medicine Society and the European Underwater and Baromedical Society Volume 48 No. 3 September 2018 Subclavian Doppler bubble monitoring Australian snorkelling and diving fatalities 2012 Inner ear barotrauma – a tool for diagnosis Which tooth restoration for divers? HBOT for large bowel anastomosis problems ISSN 2209-1491 (online); ISSN 1833-3516 (print) ABN 29 299 823 713 CONTENTS Diving and Hyperbaric Medicine Volume 48 No.3 September 2018 Editorials 198 Baltic Symposium on Diving and Hyperbaric Medicine 2018 129 The Editor’s offering Fiona Sharp 130 Decompression sickness, fatness and active hydrophobic spots Pieter Jan AM van Ooij Book review 199 Gas bubble dynamics in the human body Original articles John Fitz-Clarke 132 Reliability of venous gas embolism detection in the subclavian area for decompression stress assessment following scuba diving Julien Hugon, Asya Metelkina, Axel Barbaud, Ron Nishi, Fethi Bouak, SPUMS notices and news Jean-Eric Blatteau, Emmanuel Gempp 141 Provisional report on diving-related fatalities in Australian 201 ANZ Hyperbaric Medicine Group waters in 2011 Introductory Course in Diving John Lippmann, Chris Lawrence, Andrew Fock, Scott Jamieson and Hyperbaric Medicine 2019 168 Impact of various pressures on fracture resistance and 201 Australian and New Zealand microleakage of amalgam and composite restorations College of Anaesthetists Diving Elnaz Shafigh, Reza Fekrazad, Amir Reza Beglou and Hyperbaric Medicine Special 173 Meta-analysis -

2.2.2 GUE Fundamentals Part 2
2.2.2 GUE Fundamentals Part 2 2.2.2.1 Course Outcomes The GUE Fundamentals Part 2 course is designed to continue to cultivate the essential skills required for sound diving practice. Included among its course outcomes are: to provide the recreational diver, who does not desire diver training beyond the recreational level, with an opportunity to advance their basic diving skills; to train divers in the theory and practice of nitrox; to provide those divers who aspire to more advanced diver training with the tools that will contribute to a greater likelihood of success; and to provide divers with a gateway into advanced GUE training. 2.2.2.2 Prerequisites Applicants for a GUE Fundamentals Part 2 course must: a. Submit a completed Course Registration Form, Medical History Form, and Liability Release Form to GUE HQ. b. Hold insurance that will cover diving emergencies such as hyperbaric treatment, e.g., DAN Master-level insurance or equivalent. c. Be physically and mentally fit. d. Be a nonsmoker. e. Obtain a physician’s prior written authorization for the use of prescription drugs, except for birth control, or for any medical condition that may pose a risk while diving. f. Be a minimum of 16 years of age. Documented parental or legal guardian consent must be submitted to GUE HQ when the participant is a minor. g. Be a certified GUE Recreational Diver Level 1 diver, or have successfully completed GUE Fundamentals Part 1. 2.2.2.3 Course Content The GUE Fundamentals Part 2 course is normally conducted over three days. -
Use of Reels in Diving
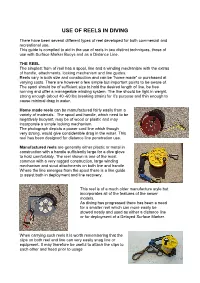
USE OF REELS IN DIVING There have been several different types of reel developed for both commercial and recreational use. This guide is compiled to aid in the use of reels in two distinct techniques, those of use with Surface Marker Buoys and as a Distance Line. THE REEL The simplest from of reel has a spool, line and a winding mechanism with the extras of handle, attachments, locking mechanism and line guides. Reels vary in both size and construction and can be “home made” or purchased at varying costs. There are however a few simple but important points to be aware of. The spool should be of sufficient size to hold the desired length of line, be free running and offer a manageable winding system. The line should be light in weight, strong enough (about 40 -60 lbs breaking strain) for it’s purpose and thin enough to cause minimal drag in water. Home made reels can be manufactured fairly easily from a variety of materials. The spool and handle, which need to be negatively buoyant, may be of wood or plastic and may incorporate a simple locking mechanism. The photograph depicts a power cord line which though very strong, would give considerable drag in the water. This reel has been designed for distance line penetration use. Manufactured reels are generally either plastic or metal in construction with a handle sufficiently large for a dive glove to hold comfortably. The reel shown is one of the most common with a very rugged construction, large winding mechanism and stout attachments on both line and handle.