Comparative Analysis of Drug Response and Gene Profiling Of
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

TNF‑Α‑Mediated Epithelial‑To‑Mesenchymal Transition Regulates Expression of Immune Checkpoint Molecules in Hepatocellular Carcinoma
MOLECULAR MEDICINE REPORTS 21: 1849-1860, 2020 TNF‑α‑mediated epithelial‑to‑mesenchymal transition regulates expression of immune checkpoint molecules in hepatocellular carcinoma RITU SHRESTHA1,2, KIM R. BRIDLE1,2, DARRELL H.G. CRAWFORD1,2 and APARNA JAYACHANDRAN1,2 1University of Queensland, Faculty of Medicine and 2Liver Cancer Unit, Gallipoli Medical Research Institute, Greenslopes Private Hospital, Brisbane, QLD 4120, Australia Received June 12, 2019; Accepted January 31, 2020 DOI: 10.3892/mmr.2020.10991 Abstract. Hepatocellular carcinoma (HCC) is the ligand (PD‑L)1, PD‑L2, CD73 and B7‑H3. In contrast, reversal fastest growing cause of cancer-related deaths globally. of EMT suppressed the expression of PD‑L1, PD‑L2, CD73 Epithelial-to-mesenchymal transition (EMT) is a cellular and B7‑H3. In addition, high expression of TNF-α and PD‑L1 process that confers HCC tumor cells with the ability to evade in 422 patients with HCC was associated with poor overall the immune system. Immune escape in most tumors, including survival. The coordinate expression of TNF-α with PD‑L2 in HCC, is controlled by immune checkpoint molecules. The aim this patient cohort was associated with increased HCC recur- of the present study was to investigate the association between rence. In conclusion, the present study demonstrated a close EMT and immune checkpoint in HCC, and identify novel ther- association between immune modulator expression and EMT apeutic targets for HCC. An in vitro model of reversible EMT induction/reversal driven by TNF-α. was utilized based on cytokine tumor necrosis factor (TNF)-α treatment of HCC cell lines Hep3B and PLC/PRF/5. -

Potential High-Impact Interventions Report Priority Area 02: Cancer
AHRQ Healthcare Horizon Scanning System – Potential High-Impact Interventions Report Priority Area 02: Cancer Prepared for: Agency for Healthcare Research and Quality U.S. Department of Health and Human Services 540 Gaither Road Rockville, MD 20850 www.ahrq.gov Contract No. HHSA290201000006C Prepared by: ECRI Institute 5200 Butler Pike Plymouth Meeting, PA 19462 December 2012 Statement of Funding and Purpose This report incorporates data collected during implementation of the Agency for Healthcare Research and Quality (AHRQ) Healthcare Horizon Scanning System by ECRI Institute under contract to AHRQ, Rockville, MD (Contract No. HHSA290201000006C). The findings and conclusions in this document are those of the authors, who are responsible for its content, and do not necessarily represent the views of AHRQ. No statement in this report should be construed as an official position of AHRQ or of the U.S. Department of Health and Human Services. This report’s content should not be construed as either endorsements or rejections of specific interventions. As topics are entered into the System, individual topic profiles are developed for technologies and programs that appear to be close to diffusion into practice in the United States. Those reports are sent to various experts with clinical, health systems, health administration, and/or research backgrounds for comment and opinions about potential for impact. The comments and opinions received are then considered and synthesized by ECRI Institute to identify interventions that experts deemed, through the comment process, to have potential for high impact. Please see the methods section for more details about this process. This report is produced twice annually and topics included may change depending on expert comments received on interventions issued for comment during the preceding 6 months. -

Osimertinib Versus Erlotinib Or Gefitinib in Patients with EGFR-Mutated Advanced Non-Smal
European Journal of Cancer 125 (2020) 49e57 Available online at www.sciencedirect.com ScienceDirect journal homepage: www.ejcancer.com Original Research Patient-reported outcomes from FLAURA: Osimertinib versus erlotinib or gefitinib in patients with EGFR- mutated advanced non-small-cell lung cancer Natasha B. Leighl a, Nina Karaseva b, Kazuhiko Nakagawa c, Byoung-Chul Cho d, Jhanelle E. Gray e, Tina Hovey f, Andrew Walding g, Anna Ryde´n h, Silvia Novello i,* a Princess Margaret Cancer Centre, Toronto, ON, Canada b City Clinical Oncology Dispensary, St. Petersburg, Russia c Department of Medical Oncology, Kindai University Faculty of Medicine, Osakasayama, Japan d Division of Medical Oncology, Yonsei Cancer Center, Yonsei University College of Medicine, Seoul, Republic of Korea e Department of Thoracic Oncology, H. Lee Moffitt Cancer Center and Research Institute, Tampa, FL, USA f PHASTAR, London, UK g AstraZeneca R&D, Cambridge, UK h AstraZeneca Gothenburg, Mo¨lndal, Sweden i Department of Oncology, University of Turin, Azienda Ospedaliero-Universitaria San Luigi Gonzaga, Turin, Italy Received 25 October 2019; accepted 6 November 2019 Available online 12 December 2019 KEYWORDS Abstract Background: In the FLAURA trial, osimertinib demonstrated superior EORTC QLQ-C30; progression-free survival and a favorable toxicity profile to erlotinib or gefitinib as initial ther- EORTC QLQ-LC13; apy in patients with EGFR-mutated advanced non-small-cell lung cancer. Patient-reported Non-small-cell lung outcomes from FLAURA are discussed here. cancer; Methods: Patients (N Z 556) completed the EORTC QLQ-LC13 weekly for 6 weeks, then Osimertinib; every 3 weeks, and the QLQ-C30 every 6 weeks. -

Vandetanib (ZD6474), an Inhibitor of VEGFR and EGFR Signalling, As a Novel Molecular-Targeted Therapy Against Cholangiocarcinoma
British Journal of Cancer (2009) 100, 1257 – 1266 & 2009 Cancer Research UK All rights reserved 0007 – 0920/09 $32.00 www.bjcancer.com Vandetanib (ZD6474), an inhibitor of VEGFR and EGFR signalling, as a novel molecular-targeted therapy against cholangiocarcinoma 1,2 3 1 4 2 3 ,1,3 D Yoshikawa , H Ojima , A Kokubu , T Ochiya , S Kasai , S Hirohashi and T Shibata* 1 2 Cancer Genomics Project, National Cancer Center Research Institute, Tokyo, Japan; Division of Gastroenterological and General Surgery, Department of Surgery, Asahikawa Medical College, Asahikawa, Japan; 3Pathology Division, National Cancer Center Research Institute, Tokyo, Japan; 4Section for Studies on Metastasis, National Cancer Center Research Institute, Tokyo, Japan Cholangiocarcinoma is an intractable cancer, with no effective therapy other than surgical resection. Elevated vascular endothelial growth factor (VEGF) and epidermal growth factor receptor (EGFR) expressions are associated with the progression of cholangiocarcinoma. We therefore examined whether inhibition of VEGFR and EGFR could be a potential therapeutic target for cholangiocarcinoma. Vandetanib (ZD6474, ZACTIMA), a VEGFR-2/EGFR inhibitor, was evaluated. Four human cholangiocarcinoma cell lines were molecularly characterised and investigated for their response to vandetanib. In vitro, two cell lines (OZ and HuCCT1), both of which harboured KRAS mutation, were refractory to vandetanib, one cell line (TGBC24TKB) was somewhat resistant, and another cell line (TKKK) was sensitive. The most sensitive cell line (TKKK) had EGFR amplification. Vandetanib significantly À1 À1 À1 À1 inhibited the growth of TKKK xenografts at doses X12.5 mg kg day (Po0.05), but higher doses (50 mg kg day , Po0.05) of À1 À1 vandetanib were required to inhibit the growth of OZ xenografts. -

S41598-018-33190-8.Pdf
www.nature.com/scientificreports OPEN Ankyrin Repeat Domain 1 Overexpression is Associated with Common Resistance to Afatinib and Received: 20 February 2018 Accepted: 25 September 2018 Osimertinib in EGFR-mutant Lung Published: xx xx xxxx Cancer Akiko Takahashi1, Masahiro Seike1, Mika Chiba1, Satoshi Takahashi1, Shinji Nakamichi1, Masaru Matsumoto1, Susumu Takeuchi1, Yuji Minegishi1, Rintaro Noro1, Shinobu Kunugi2, Kaoru Kubota1 & Akihiko Gemma1 Overcoming acquired resistance to epidermal growth factor receptor tyrosine kinase inhibitors (EGFR-TKIs) is critical in combating EGFR-mutant non-small cell lung cancer (NSCLC). We tried to construct a novel therapeutic strategy to conquer the resistance to second-and third-generation EGFR-TKIs in EGFR-positive NSCLC patients. We established afatinib- and osimertinib-resistant lung adenocarcinoma cell lines. Exome sequencing, cDNA array and miRNA microarray were performed using the established cell lines to discover novel therapeutic targets associated with the resistance to second-and third-generation EGFR-TKIs. We found that ANKRD1 which is associated with the epithelial- mesenchymal transition (EMT) phenomenon and anti-apoptosis, was overexpressed in the second-and third-generation EGFR-TKIs-resistant cells at the mRNA and protein expression levels. When ANKRD1 was silenced in the EGFR-TKIs-resistant cell lines, afatinib and osimertinib could induce apoptosis of the cell lines. Imatinib could inhibit ANKRD1 expression, resulting in restoration of the sensitivity to afatinib and osimertinib of EGFR-TKI-resistant cells. In EGFR-mutant NSCLC patients, ANKRD1 was overexpressed in the tumor after the failure of EGFR-TKI therapy, especially after long-duration EGFR- TKI treatments. ANKRD1 overexpression which was associated with EMT features and anti-apoptosis, was commonly involved in resistance to second-and third-generation EGFR-TKIs. -

Press Release
Press Release Daiichi Sankyo and AstraZeneca Announce Global Development and Commercialization Collaboration for Daiichi Sankyo’s HER2 Targeting Antibody Drug Conjugate [Fam-] Trastuzumab Deruxtecan (DS-8201) Collaboration combines Daiichi Sankyo’s scientific and technological excellence with AstraZeneca’s global experience and resources in oncology to accelerate and expand the potential of [fam-] trastuzumab deruxtecan as monotherapy and combination therapy across a spectrum of HER2 expressing cancers AstraZeneca to pay Daiichi Sankyo up to $6.90 billion in total consideration, including $1.35 billion upfront payment and up to an additional $5.55 billion contingent upon achievement of future regulatory and sales milestones as well as other contingencies Companies to share equally development and commercialization costs as well as profits worldwide from [fam-] trastuzumab deruxtecan with Daiichi Sankyo maintaining exclusive rights in Japan Daiichi Sankyo is expected to book sales in U.S., certain countries in Europe, and certain other markets where Daiichi Sankyo has affiliates; AstraZeneca is expected to book sales in all other markets worldwide, including China, Australia, Canada and Russia Tokyo, Munich and Basking Ridge, NJ – (March 28, 2019) – Daiichi Sankyo Company, Limited (hereafter, Daiichi Sankyo) announced today that it has entered into a global development and commercialization agreement with AstraZeneca for Daiichi Sankyo’s lead antibody drug conjugate (ADC), [fam-] trastuzumab deruxtecan (DS-8201), currently in pivotal development for multiple HER2 expressing cancers including breast and gastric cancer, and additional development in non-small cell lung and colorectal cancer. Daiichi Sankyo and AstraZeneca will jointly develop and commercialize [fam-] trastuzumab deruxtecan as a monotherapy or a combination therapy worldwide, except in Japan where Daiichi Sankyo will maintain exclusive rights. -

TARCEVA for Severe Renal These Highlights Do Not Include All the Information Needed to Use Toxicity
HIGHLIGHTS OF PRESCRIBING INFORMATION patients at risk of dehydration. Withhold TARCEVA for severe renal These highlights do not include all the information needed to use toxicity. (5.2) TARCEVA® safely and effectively. See full prescribing information for • Hepatotoxicity: Occurs with or without hepatic impairment, including TARCEVA. hepatic failure and hepatorenal syndrome: Monitor periodic liver testing. Withhold or discontinue TARCEVA for severe or worsening liver tests. (5.3) TARCEVA (erlotinib) tablets, for oral use • Gastrointestinal perforations: Discontinue TARCEVA. (5.4) Initial U.S. Approval: 2004 • Bullous and exfoliative skin disorders: Discontinue TARCEVA. (5.5) • ---------------------------RECENT MAJOR CHANGES-------------------------- Cerebrovascular accident (CVA): The risk of CVA is increased in patients with pancreatic cancer. (5.6) Indications and Usage, Non-Small Cell Lung Cancer (NSCLC) (1.1) 10/2016 • Microangiopathic hemolytic anemia (MAHA): The risk of MAHA is Dosage and Administration (2.1) 06/2016 increased in patients with pancreatic cancer. (5.7) Dosage and Administration, Dose Modifications (2.4) 05/2016 • Ocular disorders: Discontinue TARCEVA for corneal perforation, Warnings and Precautions, Cerebrovascular Accident (5.6) 10/2016 ulceration or persistent severe keratitis. (5.8) Warnings and Precautions, Embryo-fetal Toxicity (5.10) 10/2016 • Hemorrhage in patients taking warfarin: Regularly monitor INR in patients taking warfarin or other coumarin-derivative anticoagulants. (5.9) ---------------------------INDICATIONS -

I4X-JE-JFCM an Open-Label, Multicenter, Phase 1B/2 Study To
Protocol (e) I4X-JE-JFCM An Open-label, Multicenter, Phase 1b/2 Study to Evaluate Necitumumab in Combination with Gemcitabine and Cisplatin in the First-Line Treatment of Patients with Advanced (Stage IV) Squamous Non-Small Cell Lung Cancer (NSCLC) NCT01763788 Approval Date: 12-Jun-2016 I4X-JE-JFCM(e) Clinical Protocol Page 1 1. Protocol I4X-JE-JFCM(e) An Open-label, Multicenter, Phase 1b/2 Study to Evaluate Necitumumab in Combination with Gemcitabine and Cisplatin in the First-Line Treatment of Patients with Advanced (Stage IV) Squamous Non-Small Cell Lung Cancer (NSCLC) Confidential Information The information contained in this protocol is confidential and is intended for the use of clinical investigators. It is the property of Eli Lilly and Company or its subsidiaries and should not be copied by or distributed to persons not involved in the clinical investigation of Necitumumab (IMC-11F8; LY3012211), unless such persons are bound by a confidentiality agreement with Eli Lilly and Company or its subsidiaries. Note to Regulatory Authorities: This document may contain protected personal data and/or commercially confidential information exempt from public disclosure. Eli Lilly and Company requests consultation regarding release/redaction prior to any public release. In the United States, this document is subject to Freedom of Information Act (FOIA) Exemption 4 and may not be reproduced or otherwise disseminated without the written approval of Eli Lilly and Company or its subsidiaries. Necitumumab (IMC-11F8; LY3012211) Gemcitabine (LY188011) This is a Phase 1b/2 study in the first-line treatment of patients with advanced (Stage IV) Squamous Non-Small Cell Lung Cancer (NSCLC). -
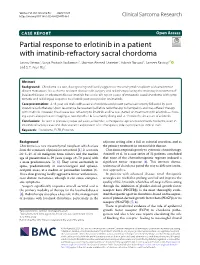
Partial Response to Erlotinib in a Patient with Imatinib-Refractory
Verma et al. Clin Sarcoma Res (2020) 10:28 https://doi.org/10.1186/s13569-020-00149-1 Clinical Sarcoma Research CASE REPORT Open Access Partial response to erlotinib in a patient with imatinib-refractory sacral chordoma Saurav Verma1, Surya Prakash Vadlamani1, Shamim Ahmed Shamim2, Adarsh Barwad3, Sameer Rastogi4* and S. T. Arun Raj2 Abstract Background: Chordoma is a rare, slow growing and locally aggressive mesenchymal neoplasm with uncommon distant metastases. It is a chemo-resistant disease with surgery and radiotherapy being the mainstay in treatment of localized disease. In advanced disease imatinib has a role. We report a case of metastatic sacral chordoma with symp- tomatic and radiological response to erlotinib post-progression on imatinib. Case presentation: A 48-year-old male with a sacral chordoma underwent partial sacrectomy followed by post- operative radiotherapy. Upon recurrence he received palliative radiotherapy to hemipelvis and was ofered therapy with imatinib. However, the disease was refractory to imatinib and he was started on treatment with erlotinib—show- ing a partial response on imaging at two months. He is currently doing well at 13 months since start of erlotinib. Conclusions: As seen in previously reported cases, erlotinib is a therapeutic option in advanced chordoma, even in imatinib refractory cases and thus warrants exploration of its therapeutic role in prospective clinical trials. Keywords: Chordoma, EGFR, Erlotinib Background adjuvant setting after a full or subtotal resection, and as Chordoma is a rare mesenchymal neoplasm which arises the primary treatment in unresectable disease. from the remnants of primitive notochord [1]. It accounts Chordoma responds poorly to cytotoxic chemotherapy. -
Multi-Discipline Review
CENTER FOR DRUG EVALUATION AND RESEARCH APPLICATION NUMBER: 761139Orig1s000 MULTI-DISCIPLINE REVIEW Summary Review Office Director Cross Discipline Team Leader Review Clinical Review Non-Clinical Review Statistical Review Clinical Pharmacology Review NDA/BLA Multi-disciplinary Review and Evaluation {BLA 761139} ENHERTU (fam-trastuzumab deruxtecan-nxki) NDA/BLA Multi-disciplinary Review and Evaluation Disclaimer: In this document, the sections labeled as “The Applicant’s Position” are completed by the Applicant, which do not necessarily reflect the positions of the FDA. Application Type Biologics License Application (BLA) 351(a) Application Number BLA 761139 Priority or Standard Priority Submit Date(s) August 29, 2019 Received Date(s) August 29, 2019 PDUFA Goal Date April 29, 2020 Division/Office DO1/OOD/OND/CDER Review Completion Date Electronic Stamp Date Established Name fam-trastuzumab deruxtecan-nxki (Proposed) Trade Name ENHERTU Pharmacologic Class HER2-directed antibody and topoisomerase inhibitor conjugate Code name Applicant Daiichi Sankyo, Inc Formulation(s) 100 mg lyophilized powder Dosing Regimen 5.4 mg IV every 3 weeks (b) (4) Applicant Proposed Indication(s)/Population(s) Recommendation on Accelerated Approval Regulatory Action Recommended Treatment of adult patients with unresectable or metastatic Indication(s)/Population(s) HER2-positive breast cancer who have received two or more (if applicable) prior anti-HER2-based regimens in the metastatic setting. 1 Version date: June 11, 2019 (ALL NDA/BLA reviews) Disclaimer: In this document, the sections labeled as “The Applicant’s Position” are completed by the Applicant and do not necessarily reflect the positions of the FDA. Reference ID: 4537638 NDA/BLA Multi-disciplinary Review and Evaluation {BLA 761139} ENHERTU (fam-trastuzumab deruxtecan-nxki) Table of Contents Reviewers of Multi-Disciplinary Review and Evaluation ............................................................. -

Fam-Trastuzumab Deruxtecan-Nxki Submitted by Daiichi
Dan Liang, PharmD Associate Director, Medical Information & Education Daiichi Sankyo, Inc. 211 Mount Airy Road Basking Ridge, NJ 07920 Phone: 908-992-7054 Email: [email protected] Date of request: July 9, 2020 NCCN Panel: Colon Cancer and Rectal Cancer On behalf of Daiichi Sankyo, Inc. and AstraZeneca Pharmaceuticals LP, I respectfully request the NCCN Guideline Panel for Colon and Rectal Cancers to review data from the clinical study1 in support of fam-trastuzumab deruxtecan-nxki, also known as T-DXd, as a monotherapy option for the treatment of patients with HER2-positive unresectable and/or metastatic colorectal cancer. Specific Changes: We respectfully ask the NCCN panel to consider the following: • COL-D1 through COL-D6 and REC-F1 through REC-F6, “Continuum of Care - Systemic Therapy for Advanced or Metastatic Disease” o Add “Fam-trastuzumab deruxtecan-nxki (HER2-positive and RAS and BRAF WT)” to the following: . COL-D1 and REC-F1: “Patient not appropriate for intensive therapy” . COL-D2 and REC-F2: “Previous oxaliplatin-based therapy without irinotecan” . COL-D3 and REC-F3: “Previous irinotecan-based therapy without oxaliplatin” . COL-D4 and REC-F4: “Previous treatment with oxaliplatin and irinotecan” . COL-D5 and REC-F5: “Previous therapy without irinotecan or oxaliplatin” . COL-D6 and REC-F6: “FOLFOX or CAPEOX or (FOLFOX or CAPEOX) + bevacizumab” • COL-D11 and REC-F11, “Systemic Therapy for Advanced or Metastatic Disease – Chemotherapy Regimens” o Add “Fam-trastuzumab deruxtecan-nxki 6.4 mg/kg IV on Day 1, cycled every 21 days” with a footnote: “fam-trastuzumab deruxtecan-nxki is approved for metastatic HER2-positive breast cancer at a different dose of 5.4 mg/kg IV on Day 1, cycled every 21 days” FDA Clearance: ENHERTU (fam-trastuzumab deruxtecan-nxki) is a HER2-directed antibody and topoisomerase inhibitor conjugate indicated for the treatment of adult patients with unresectable or metastatic HER2-positive breast cancer who have received two or more prior anti-HER2-based regimens in the metastatic setting. -

Cogent Biosciences Announces Creation of Cogent Research Team
Cogent Biosciences Announces Creation of Cogent Research Team April 6, 2021 Names industry veteran John Robinson, PhD as Chief Scientific Officer New Boulder-based team with exceptional track record of drug discovery and development focused on creating novel small molecule therapies for rare, genetically driven diseases Strong year-end cash position of $242.2 million supports company goals into 2024, including three CGT9486 clinical trials on-track to start this year, beginning with ASM in 1H21 BOULDER, Colo. and CAMBRIDGE, Mass., April 6, 2021 /PRNewswire/ -- Cogent Biosciences, Inc. (Nasdaq: COGT), a biotechnology company focused on developing precision therapies for genetically defined diseases, today announced the formation of the Cogent Research Team led by newly appointed Chief Scientific Officer, John Robinson, PhD. "Today marks an important step forward for Cogent Biosciences as we announce the formation of the Cogent Research Team with a focus on discovering and developing new small molecule therapies for patients fighting rare, genetically driven diseases," said Andrew Robbins, President and Chief Executive Officer of Cogent Biosciences. "I am thrilled to welcome John onboard as Cogent Biosciences' Chief Scientific Officer. John's expertise and seasoned leadership make him ideally suited to lead this new team of world class scientists. Given the team's impressive experience and accomplishments, we are excited for Cogent Biosciences' future and the opportunity to expand our pipeline and deliver novel precision therapies for patients." With an exceptional track record of innovation, the Cogent Research Team will focus on pioneering best-in-class, small molecule therapeutics to both improve upon existing drugs with clear limitations, as well as create new breakthroughs for diseases where others have been unable to find solutions.