Behavior Change Communication Activities and Achievements Sustainability Equity
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Office of the Civil Surgeon, West Singhbhum, Chaibasa List of Eligible Candidate for the Post of LAB TECHNICIAN CHC NCD CLINIC Post Code - 15, Advt
Office of the Civil Surgeon, West Singhbhum, Chaibasa List of Eligible Candidate for the Post of LAB TECHNICIAN CHC NCD CLINIC Post Code - 15, Advt. No 01 2017 Technical Qualification Inter Jharkhand (DMLT) State Experie Knowle Form Paramedic nce Sl. Father's Date of Home Residen Categor dge of Amo Sl. Name Mobile no Permanent Address Present Address al counl, (Min. Remarks Bank Name DD No DD Date No. Name Birth District tial y Compu unt No. Marks Marks Ranchi - 02 Total Total ter Obtaine % Obtaine % Registrato Years) Marks Marks d d n AT - SURYA NARSING VILL - DUDRI, PO - TOKLO, HOME, THANA ROAD, SUSHIL WEST PNB, NIRANJAN CHAKRADHARPUR, DIST - WARD NO 02, PO - YES OBC 04 Y 01 1 4 KUMAR 12-Jan-1990 9934978075 SINGHB 500 280 56.00% 700 503 71.86% NA NA ASANTALI 818130 11-Sep-2017 MAHTO WEST SINGHBHUM, CHAKRADHARPUR, DIST - (SDO) (SDO) M MAHTO HUM A 400.00 JHARKHAND WEST SINGHBHUM, JHARKHAND VILL - ABHAYPUR, PO - VILL - ABHAYPUR, PO - SANJAY URKIYA, PS - URKIYA, PS - WEST CANARA PRAYAG YES OBC 2 59 KUMAR 15-Feb-1985 9438509940 MANOHARPUR, DIST - MANOHARPUR, DIST - SINGHB 900 460 51.11% 700 422 60.29% NA 02 M NA BANK, 967913 09.16.2017 MAHTO (SDO) (CO) MAHTO WEST SINGHBHUM, WEST SINGHBHUM, HUM CHAIBASA 400.00 JHARKHAND JHARKHAND VILL - BHOGRA, VILL - GUA, GUASAI, PO - MHANTISAI, PO - WEST GEETA KHAGESHW GUA, DIST - WEST 03 Y 02 3 75 27-Dec-1986 7091265622 JAGANNATHPUR, DIST - SINGHB 500 235 47.00% 1900 1409 74.16% NA NA SBI, GUA 407515 16-Sep-2017 KUMARI AR PAN SINGHBHUM, M WEST SINGHBHUM, HUM 400.00 JHARKHAND JHARKHAND VILL - SIDMA BARU -
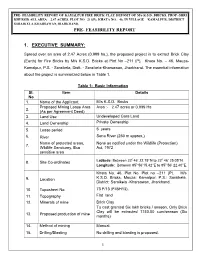
Pre- Feasibility Report 1. Executive Summary
PRE- FEASIBILITY REPORT OF KAMALPUR FIRE BRICK CLAY DEPOSIT OF M/s K.S.D. BRICKS, PROP.-SHRI KHURSID ALI, AREA – 2.47 ACRES, PLOT NO –211(P), KHATA NO.– 46, IN VILLAGE – KAMALPUR, DISTRICT – SARAIKELA-KHARSAWAN,JHARKHAND. PRE- FEASIBILITY REPORT 1. EXECUTIVE SUMMARY: Spread over an area of 2.47 Acres (0.999 ha.), the proposed project is to extract Brick Clay (Earth) for Fire Bricks by M/s K.S.D. Bricks at Plot No –211 (P), Khata No. – 46, Mauza- Kamalpur, P.S. - Saraikela, Distt. - Saraikela-Kharsawan, Jharkhand. The essential information about the project is summarized below in Table 1. Table 1: Basic Information Sl. Item Details No 1. Name of the Applicant M/s K.S.D. Bricks Proposed Mining Lease Area Area :- 2.47 acres or 0.999 Ha 2. (As per Agreement Deed) 3. Land Use Undeveloped Gora Land 4. Land Ownership Private Ownership 5. Lease period 5 years 6. River Sona River (250 m approx.) Name of protected areas, None as notified under the Wildlife (Protection) 7. Wildlife Sanctuary, Eco Act, 1972 sensitive area 0 0 8. Site Co-ordinates Latitude: Between 22 46’ 22.15’’N to 22 46’ 25.05’’N. Longitude: Between 850 56’15.42’’E to 850 56’ 22.40’’E. Khata No. 46, Plot No. Plot no –211 (P), M/s 9. Location K.S.D. Bricks, Mouza: Kamalpur, P.S.: Saraikela, District: Saraikela -Kharsawan, Jharkhand. 10. Toposheet No. 73 F/13 (F45H13). 11. Topography Flat land 12. Minerals of mine Brick Clay To cast granted Six lakh bricks / season, Only Brick Clay will be extracted 1740.00 cum/season (Six 13. -

Jharkhand Road Projects Implementation Company Limited (Jrpicl)
JHARKHAND ROAD PROJECTS IMPLEMENTATION COMPANY LIMITED (JRPICL) EIGHTH ANNUAL REPORT 2016-17 Overview and Achievements The Government of Jharkhand (GoJ) and Infrastructure Leasing & Financial Services Limited (IL&FS) entered into a Programme Development Agreement (PDA) dated February 06, 2008 to form a Joint Venture for upgradation of about 1,500 lane kms of roads in the State of Jharkhand under Jharkhand Accelerated Road Development Programme (JARDP). Pursuant to the aforesaid PDA, GoJ and IL&FS incorporated a Special Purpose Entity (SPE) in the name of Jharkhand Accelerated Road Development Company Limited (JARDCL) for successful implementation of the JARDP including planning, designing and procurement of contractors, financing, construction, operation and maintenance of the road stretches identified under the JARDP. As per the terms of the PDA, the financing, construction, operation and maintenance of road projects may be taken up either by JARDCL or through another Project SPV to be incorporated either by GoJ and/or IL&FS, as mutually agreed. With the approval of GoJ, IL&FS on August 04, 2009 incorporated the Project SPV namely Jharkhand Road Projects Implementation Company Limited (JRPICL) to carry out the implementation work under the JARDP. 1500 Lane km of road was mandated to be developed under Jharkhand Accelerated Road Development Programme (JARDP), out of which till date over 768.61 Lane Km of road has been assigned to our Company. Your Company has successfully completed 5 road projects namely Four Sections of Ranchi Ring Road (Section III, IV, V & VI), Ranchi Patratu Dam Road, Patratu Dam – Ramgarh Road Project, Adityapur – Kandra Road and Chaibasa – Kandra Chowka Road Projects within the timeline set by the Government of Jharkhand from time to time and also commenced the Operation & Maintenance work of all these projects. -

Kolhan University, Chaibasa (Examination Department)
KOLHAN UNIVERSITY, CHAIBASA (EXAMINATION DEPARTMENT) Examination Centre for B.A./B.Sc./B.Com. Part-III (H/G/Voc) Exam. 2017. (2014-17) Reporting Time : 9.30 A.M. Time : 10.00 A.M. to 01.00 P.M. Sl. Name of the Centre Name of the College attached Name of the Centre No Superintendent. 1. Tata College, Chaibasa 1. Mahila College, Chaibasa Principal, 2. G.C. Jain Comm. College, Chaibasa Tata College, Chaibasa 2. Mahila College, Chaibasa 1. Tata College, Chaibasa Principal, 2. Noamundi College, Noamundi Mahila College, Chaibasa 3. J.L.N. College, 1. J.L.N. College, Chakradharpur Principal, Chakradharpur 2. VAS College, Sonua J.L.N. College, Chakradharpur 3. St. Augustine College, Manoharpur 4. K.S. College, 1. K.S. College, Saraikella Principal, Saraikella K.S. College, Saraikella 5. Singhbhum College, 1. Singhbhum College, Chandil Principal, Chandil S.B. College, Chandil 1. Jsr.Co-operative College, Jamshedpur Principal, J.K.S. College 6. 2. Patamda Degree College, Jalla J.K.S. College, Jamshedpur Jamshedpur 3. NSIBM, Pokhari, Jamshedpur 7. The G.S.C. for Women, 1.Karim City College, Jamshedpur Principal, Jamshedpur The G.S. C. for Women, Jsr. 8. L.B.S.M. College, 1. A.B.M. College, Jamshedpur Principal, Jamshedpur L.B.S.M. College, Jamshedpur 9. A.B.M. College, 1. J.K.S. College, Jamshedpur Principal, Jamshedpur 2. AJK College, Asanboni A.B.M. College, Jamshedpur 3. Jain college, Jamshedpur 4. Mrs. KMPM Voc. College, Jamshedpur 5. GIIT College, Jamshedpur 10. Jsr. Co-operative College, 1. Jsr. Workers’ College, Jamshedpur Principal, Jamshedpur Jsr. -

Table 4. 5 List of MOU's in Jharkhand
Table 4. 5 List of MOU's in Jharkhand Name of the Company Product to be manufactured Proposed Investment District I Proposed Site (Rs. In crore) 1 Mis Monnet !spat Limited, Integrated Steel Plant (DRI based) 1400 Hazaribagh 2 Mis Vallabh Steel Limited, Sponge Iron, Power Plant, Steel Plant 288 Saraikela-Kharsawan 3 Mis Aadhunik Allov &Power Ltd. Sponge Iron, Power Plant, Steel Plant 970 Saraikela-Kharsawan Sponge Iron, Power Plant, Steel Plant, 4 Mis Nilanchal Iron & Power Ltd. Mining 450 Saraikela-Kharsawan 5 Mis Jharkhand Ispat Pvt. Ltd., Sponge Iron, Steel Plant, 400 Ramgrah Sponge Iron, Captive Coal Mine, 6 Mis Abhijeet Infrastructure Pvt. Ltd. Ferro Allov 300 Hazaribag 7 Mis AML Steel & Power Ltd. Integrated Steel Plant 2000 Saraikela-Kharsawan Sponge Iron, Captive Coal Mine, 8 Mis Corporate IsPat Alloy Limited, Ferro Allov 300 Hazaribagh Sponge Iron, Captive Coal Mine, 9 Mis Annpuma Global Ltd, Power Plant 500 Mis Prasad Groups, Resources, Pvt Sponge Iron, Power Plant, Steel IO Ltd. Plant, Mining 400 Ramgarh Sponge Iron , Captive Coal Mine 11 MlsPrakash !spat , Crushing Unit 71.4 Chaibasa Sponge Iron , Captive Coal Mine 12 MlsHorizon Eximp Ltd. ,Crushing Unit 74.15 Chaibasa Sponge Iron , Captive Coal Mine 13 MlsSpectrum Mercantile Pvt. Ltd., Crushing Unit 74.15 Chaibasa 14 Mis Chaibassa Steel Pvt. Ltd. Sponge Iron 74.15 Chaibasa 15 Mis Tech Al Corporation Allumina Plant 6500 16 Mis Electro steel Casting Ltd. Soonge, Steel & Power 200 Lohardaga 17 MIS Balajee Industrial Product Ltd. Sponge Iron, Pig Iron, Steel Making 122 Chaibasa 18 Mis Pawaniai Steel & Power Ltd. Sponge Iron, Steel Making 1000 Lohardaga Sponge Iron &Induction Furnace, 19 Mis R G Steels Pvt. -

Interstate Routes in Between Odisha and Jharkhand
.,-. AIFEE LIST OF VACANT -INTERSTATE •ROUTES IN BETWEEN ODISH A AND JHARKHAND No., . Permits to No. of SI Distance of the Route in KMs Name of the routes be issued Trips Nature of No. J . by Service Jharkh W. Total Length Odisha Bihar Odisha Odisha and Bengal of the Route 1 2 3 4 5 6 7 8 9 10 ,Bhadrak to Tata via.Balasore, 1 255 Baripada, Rairangpur, Tiring 40 0 0 295 1 1 Express Baripada to Chakulia 2 41 via.Jamsola 39 0 0 80 2 ' 4 Ordinary _ Bolani to Chaibasa via.Barbil, 3 40 Nalda, Badajamda 107 0 0 147 1 2 Ordinary Baripada to Bokaro 4 via.Rairangpur, Tiring, Tata, 118 166 0 64 348 2 2 -Express Purulia . Baripada to Musabani 5 40 via.Jamsola 45 0 0 85 3 6 Ordinary - . Chaibasa to Rairangpur 6 45 via.Tiring, Hata 120 0 . 0 165 1 • 2 Ordinary Chaibasa to Barbil via.Cha mpua, 7 65 Jayantgarh 67 0 0 132 1 2 Ordinary . Deoghar to Baripada via.Giridih, 8 Hazaribag, Ranchi, Tata, 118 500 0 0 618 2 2 •ExpFess . Rairangpur, Tiring • • 9 Gumla to Baripada via.Sisai, 118 270 0 Ranchi, Tata, Tiring, RaWangpur 388 2 2 express 10 Jharadihi to Saraikela via.Tata, Tiring 95 0 135 1 2 Ordinary Ranchi to Keonjhar via.Khunti, 11 195 0 0 Chaibasa, Champua 249 2 2 Ordinary Rourkela to Gua via.Barbil, 12 Nalda 20 0 0 194 1 2 Ordinary Simdega to Sundergarh 13 via.Subdega, Rouldega, 88 60 0 0 148 Sagbahal 1 2 Ordinary Simdega to Debgarh 14 via.Birmitrapur, Rourkela, 190 48 0 0 238 Panposh, Bonai, Barkot 1 1 Ordinary 15 Joda to Gumla via.Lasthikata, 175 130 0 0 Rourkela, Biramitrapur 305 1 1 .Express Baripada to Chatra via.Jamsola, 16 40 355 0 0 Tata, Ranchi 39'5 1 1 Express Baripada ato Daltanganj 17 via.Rairangpur, Tiring, Tata, 118 395 0 0 513 Ranchi 1 1 Express Berhampur to Tata via.Baripai 18 da, Jamsola renamed 483 235 0 0 as Berhampur to Ranchi 718 1 1 Expr-ess via.Jamsola, Tata • LIST OF VACANT INTERSTATE ROUTES PLYING BETWEEN ODISHA AND BIHAR PASSING THROUGH JHARKHAND THE . -

Manager Building Project Bhawan Campus, Jamshedpur.Hospital
., F.No.21-35/2020-IA-III Government of India Ministry of Environment, Forest and Climate Change (IA.Ill Section) Indira Paryavaran Bhawan, Jor Bagh Road, New Delhi - 3 Date: 02 July, 2020 To, Shri Lalit Kumar Tibrewal, Zonal Manager M/s Jharkhand State Building Construction Corporation Limited 3rd Floor JSBCCL Building Project Bhawan Campus, P.O. Dhurwa Ranchi-834004, Jharkhand E-Mail: [email protected] Subject: 'Construction of 500 bedded Government Hospital', located at Khasra No. 1726 (bg, bh, bk, bl), 1727, Village Dimna, Circle Mango, Town Jamshedpur, District East Singhbum, Jharkhand by M/s Jharkhand State Building Construction Corporation Limited- Environmental Clearance- reg. Sir, This has reference to your online proposal No.lA/JH/MIS/151071/2020 dated 08.04.2020, submitted to this Ministry for grant of Environmental Clearance (EC) in terms of the provisions of the Environment Impact Assessment (EIA) Notification, 2006 under the Environment (Protection) Act, 1986. 2. The proposal for grant of environmental clearance to the project 'Construction of 500 bedded Government Hospital', located at Khasra No. 1726 (bg, bh, bk, bl), 1727, Village Dimna, Circle Mango, Town Jamshedpur, District East Singhbum, Jharkhand by M/s Jharkhand State Building Construction Corporation Limited, was considered by the Expert Appraisal Committee {lnfra-2) in its 5151meeting held during 21-22 May, 2020. The details of the project, as per the documents submitted by the project proponent, and also as informed during the above meeting are as under: - (i) The project is located at 1726 (bg, bh, bk, bl), 1727 Village Dimna, Circle Mango, Town Jamshedpur, District East Singhbum, Jharkhand Latitude 22°50'34.1 ?"N and Longitude 86°13'56.45"E. -
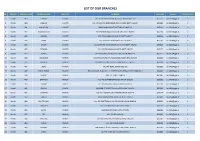
List of Our Branches
LIST OF OUR BRANCHES SR REGION BRANCH CODE BRANCH NAME DISTRICT ADDRESS PIN CODE E-MAIL CONTACT NO 1 Ranchi 419 DORMA KHUNTI VILL+PO-DORMA,VIA-KHUNTI,DISTT-KHUNTI-835 227 835227 [email protected] 0 2 Ranchi 420 JAMHAR KHUNTI VILL-JAMHAR,PO-GOBINDPUR RD,VIA-KARRA DISTT-KHUNTI. 835209 [email protected] 0 3 Ranchi 421 KHUNTI (R) KHUNTI MAIN ROAD,KHUNTI,DISTT-KHUNTI-835 210 835210 [email protected] 0 4 Ranchi 422 MARANGHADA KHUNTI VILL+PO-MARANGHADA,VIA-KHUNTI,DISTT-KHUNTI 835210 [email protected] 0 5 Ranchi 423 MURHU KHUNTI VILL+PO-MURHU,VIA-KHUNTI, DISTT-KHUNTI 835216 [email protected] 0 6 Ranchi 424 SAIKO KHUNTI VILL+PO-SAIKO,VIA-KHUNTI,DISTT-KHUNTI 835210 [email protected] 0 7 Ranchi 425 SINDRI KHUNTI VILL-SINDRI,PO-KOCHASINDRI,VIA-TAMAR,DISTT-KHUNTI 835225 [email protected] 0 8 Ranchi 426 TAPKARA KHUNTI VILL+PO-TAPKARA,VIA-KHUNTI, DISTT-KHUNTI 835227 [email protected] 0 9 Ranchi 427 TORPA KHUNTI VILL+PO-TORPA,VIA-KHUNTI, DISTT-KHUNTI-835 227 835227 [email protected] 0 10 Ranchi 444 BALALONG RANCHI VILL+PO-DAHUTOLI PO-BALALONG,VIA-DHURWA RANCHI 834004 [email protected] 0 11 Ranchi 445 BARIATU RANCHI HOUSING COLONY, BARIATU, RANCHI P.O. - R.M.C.H., 834009 [email protected] 0 12 Ranchi 446 BERO RANCHI VILL+PO-BERO, RANCHI-825 202 825202 [email protected] 0 13 Ranchi 447 BIRSA CHOWK RANCHI HAWAI NAGAR, ROAD NO. - 1, KHUNTI ROAD, BIRSA CHOWK, RANCHI - 3 834003 [email protected] 0 14 Ranchi 448 BOREYA RANCHI BOREYA, KANKE, RANCHI 834006 [email protected] 0 15 Ranchi 449 BRAMBEY RANCHI VILL+PO-BRAMBEY(MANDER),RANCHI-835205 835205 [email protected] 0 16 Ranchi 450 BUNDU -

Kandra Road Project of Jharkhand Road Projects Implementation Company Limited for the Long Term Bank Loan Facility of ` 171.93 Cr on Its Annual Surveillance
Rating Review Rationale Brickwork Ratings revises the rating of Adityapur – Kandra Road Project of Jharkhand Road Projects Implementation Company Limited for the Long Term Bank Loan Facility of ` 171.93 Cr on its Annual Surveillance. Brickwork Ratings (BWR) revises the Rating1 of Adityapur–Kandra Road Project of Jharkhand Road Projects Implementation Company Limited (JRPICL-AK) availed from Allahabad Bank and Dena Bank to BWR BBB+ [Pronounced BWR Triple B Plus] (Outlook: Stable) for the Long Term Bank Loan Facility of ` 171.93 Cr on Annual Surveillance from BWR BBB [Pronounced BWR Triple B] (Outlook: Stable) reviewed on August 01, 2013. As on 15-Jul-2014 (` Cr) Consortium Banks/Rs Cr Limit Draw Down Outstanding Rating Amount Allahabad Bank (Lead Bank) 100.00 100.00 94.73 94.73 Dena Bank 81.50 81.50 77.20 77.20 Total Term Loans 181.50 181.50 171.93 171.93 Limits Facility Tenure Revised Rating Previous Rating (₹ Cr) BWR BBB BWR BBB+ Term Long (Pronounced BWR 171.93 (Pronounced BWR Triple B Plus) Loan Term Triple B) (Outlook: Stable) (Outlook: Stable) Jharkhand Road Projects Implementation Company Limited (JRPICL) is a joint venture promoted by IL&FS (Infrastructure Leasing & Financial Services Limited) & its subsidiary ITNL (IL&FS Transportation Networks Limited), incorporated on Aug 04, 2009, for four laning of 15.1 kms each on Adityapur-Kandra section in the state of Jharkhand under JARDP (Jharkhand Accelerated Road Development Programme). JRPICL is supported by Government of Jharkhand (GOJ). It is formed to undertake the design, engineering, financing, procurement, construction, operation and maintenance of the road projects on BOT Annuity Basis. -
Singhbhum West.Pdf
Contents S. No. Topic Page No. 1. General Characteristics of the District 1 1.1 Location & Geographical Area 1 1.2 Topography 2 1.3 Availability of Minerals. 2 1.4 Forest 2 1.5 Administrative set up 2 2. District at a glance 3 2.1 Existing Status of Industrial Area in the District Singhbhum(West) 6 3. Industrial Scenario Of Singhbhum(West) 6 3.1 Industry at a Glance 6 3.2 Year Wise Trend Of Units Registered 7 3.3 Details Of Existing Micro & Small Enterprises & Artisan Units In 7 The District 3.4 Large Scale Industries / Public Sector undertakings 8 3.5 Major Exportable Item 9 3.6 Growth Trend 9 3.7 Vendorisation / Ancillarisation of the Industry 9 3.8 Medium Scale Enterprises 10 3.8.1 List of the units in Singhbhum(West )& near by Area 10 3.8.2 Major Exportable Item 13 3.9 Service Enterprises 14 3.9.1 Coaching Industry 14 3.9.2 Potentials areas for service industry 15 3.10 Potential for new MSMEs 15 4. Existing Clusters of Micro & Small Enterprise 15 4.1 Detail Of Major Clusters 15 4.1.1 Manufacturing Sector 15 4.1.2 Service Sector 15 4.2 Details of Identified cluster 15 5. General issues raised by industry association during the course of 16 meeting 6 Steps to set up MSMEs 17 7. Additional information if any 18 II Brief Industrial Profile of Singhbhum(West )District 1. General Characteristics of the District West Singhbhum or Pashchimi Singhbhum is one of the 24 districts of Jharkhand state. -

Fiftieth Report Standing Committee on Urban and Rural Development
FIFTIETH REPORT STANDING COMMITTEE ON URBAN AND RURAL DEVELOPMENT (2003) (THIRTEENTH LOK SABHA) THE PROVISIONS OF THE MUNICIPALITIES (EXTENSION TO THE SCHEDULED AREAS) BILL, 2001 MINISTRY OF URBAN DEVELOPMENT AND POVERTY ALLEVIATION (DEPARTMENT OF URBAN DEVELOPMENT) Presented to Lok Sabha on …………… Laid in Rajya Sabha on …………… LOK SABHA SECRETARIAT NEW DELHI November, 2003/Kartika, 1925 (Saka) CONTENTS PAGE COMPOSITION OF THE COMMITTEE (2003).................................................. (iii) COMPOSITION OF THE COMMITTEE (2002).................................................. (v) COMPOSITION OF THE COMMITTEE (2001).................................................. (vii) INTRODUCTION .............................................................................................. (ix) REPORT PART-I Background of ‘The Provisions of the Municipalities (Extension to the Scheduled Areas) Bill, 2001’. .............................. 1 PART—II Analysis of ‘The Provisions of the Municipalities (Extension to the Scheduled Areas) Bill, 2001’. .............................. 4 APPENDICES I. ‘The Provisions of the Municipalities (Extension to the Scheduled Areas) Bill, 2001’ ............... 31 II. The Constitution (Seventy-fourth Amendment) Act, 1992. ............................................................................................ 40 III. Memoranda received from experts/organisations on the various provisions of the Bill ...................................... 59 IV. Statement showing clause by clause suggestions/ observations made by -

E-Tender for Comprehensive AMC of Computers, Network Switches, LAN
कमचारी रा बीमा िनगम ेीय कायालय / Regional Office )म एवं रोजगार मंालय , भारत सरकार ( पंचदीप भवन , नामकुम , राँची 834010- EMPLOYEES’ STATE INSURANCE CORPORATION PANCHDEEP BHAWAN, NAMKUM, RANCHI -834010 (Ministry of Labour & Employment , Govt. of India) Phone : 0651-2960319 Email : [email protected] Website : www.esic.nic.in / www.esic.in Fi leNo.15/D/21/24/07/2019 -General Dated: 29/07/2021 E-Tender Notice E-TENDER FOR COMPREHENSIVE AMC of COMPUTERS, NETWORK SWITCHES, LAN, LAN NODES, PRINTERS, VoIP PHONES I NCLUDING CABLING, UPSs, BIOMETRI C DEVICES AND ASSOCIATED PERIPHERALS ALONG WITH LAN CABLING , POWER CABLING AND EARTHING WORK OF VARIOU S ESIC & ESIS SITES ACROSS JHARKHAND REGION. 1) Regional Office, E.S.I. Corporation, Ranchi invites online tender from eligible, reputed, and bonafide maintenance providers/agencies capable of providing above captioned work for its various sites in Jharkhand Region for a period of Two Years. 2) The tender document can be downloaded from https://www.esic.nic.in/tenders, Central Public Procurement Portal: https://eprocure.gov.in/eprocure/app. 3) The interested bidders m ay submit the tender online at e-procurement portal https://eprocure.gov.in/eprocure/app in two-bid system in the prescribed proforma. Tenders are to be submitted online only through e -procurement portal . All the supporting documents required are requested to be submitted physically also along with EMD. Online bids for which not all supporting documents are submitted physically will be treated as invalid. In other words, online submission of bids along with submission of all the supporting documents physica lly is required for every participating bidder.