Identifying Opportunities and Challenges to Strengthen Union
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Mamoni Newsletter Issue 8, Jan-Mar 2017
MaMoni Health Systems Strengthening Project Issue 08 January- March Newsletter 2017 Community Skilled Birth Attendant (CSBA) e-register rolled out in Madhabpur Photo: Save the Children/Bashir Ahmed Save Photo: aMoni HSS project is collaborating with Measure Evaluation, icddrb and SIAP project to introduce electronic ManagementM Information System (eMIS) in Habiganj district. Recent months saw CSBA module (e-register) rolled out and incorporation of GIS map into the monitoring tool. Data from UH&FWC facility assessment has been integrated with the service statistics allowing presentation of multiple information in a logically segregated way. CSBA module has been rolled out in Madhabpur Upazila of Habiganj and Basail Upazila of Tangail. Training on General Patient, Family Planning and PAC e-registers were organized in all upazilas of Habiganj except Madhabpur, where all the service modules have already been rolled out. The reference document and manual for the e-registers have been developed and practiced during the training sessions. Simultaneously FWA e-register was introduced throughout Habiganj. aMoni HSS Project shared program experiences at the Community Health Workers’ Symposium held from 21st to 23rd FebruaryM 2017 in Kampala, Uganda. The symposium titled "Contribution of Community Health Workers (CHWs) toward Earlier all the DGFP CSBAs of Madhabpur, 13 in total, had received training on MNC e-register and started working on it. Again attainment of the Sustainable Development Goals (SDGs)" was organised by the School of Social Sciences Public Health team around 400 HAs and FWAs were trained on PRS application who have been collecting population data since. In Madhabpur, at Nottingham Trent University (NTU), Makerere University School of Public Health (MakSPH) and the Ugandan Ministry of some 92% of the population have been registered and given away Health ID cards. -

English Language Newspaper Readability in Bangladesh
Advances in Journalism and Communication, 2016, 4, 127-148 http://www.scirp.org/journal/ajc ISSN Online: 2328-4935 ISSN Print: 2328-4927 Small Circulation, Big Impact: English Language Newspaper Readability in Bangladesh Jude William Genilo1*, Md. Asiuzzaman1, Md. Mahbubul Haque Osmani2 1Department of Media Studies and Journalism, University of Liberal Arts Bangladesh, Dhaka, Bangladesh 2News and Current Affairs, NRB TV, Toronto, Canada How to cite this paper: Genilo, J. W., Abstract Asiuzzaman, Md., & Osmani, Md. M. H. (2016). Small Circulation, Big Impact: Eng- Academic studies on newspapers in Bangladesh revolve round mainly four research lish Language Newspaper Readability in Ban- streams: importance of freedom of press in dynamics of democracy; political econo- gladesh. Advances in Journalism and Com- my of the newspaper industry; newspaper credibility and ethics; and how newspapers munication, 4, 127-148. http://dx.doi.org/10.4236/ajc.2016.44012 can contribute to development and social change. This paper looks into what can be called as the fifth stream—the readability of newspapers. The main objective is to Received: August 31, 2016 know the content and proportion of news and information appearing in English Accepted: December 27, 2016 Published: December 30, 2016 language newspapers in Bangladesh in terms of story theme, geographic focus, treat- ment, origin, visual presentation, diversity of sources/photos, newspaper structure, Copyright © 2016 by authors and content promotion and listings. Five English-language newspapers were selected as Scientific Research Publishing Inc. per their officially published circulation figure for this research. These were the Daily This work is licensed under the Creative Commons Attribution International Star, Daily Sun, Dhaka Tribune, Independent and New Age. -

Interaction Between Journos Imperative, Says Indian Press Council Chair Staff Correspondent
Interaction between journos imperative, says Indian Press Council chair Staff Correspondent Members of a visiting team of the Press Council of India exchange views with senior journalists of media outlets of the East West Media Group Ltd at its conference room in the city on Wednesday.- sun photo Interaction and cooperation between journalists of India and Bangladesh are needed to overcome common professional barriers, threats and challenges, said Press Council of India Chairman Justice Chandramauli Kumar Prasad. Media coverage in a conflict zone has become a great challenge for journalists, he stated. “Journalism is going to be a risky profession in the subcontinent as they have to face different kinds of threats and challenges.” The media crew of both the friendly countries should unitedly challenge the menaces confronting them in professional duties, Justice Prasad said. The observations were made during a view-exchange meeting of a delegation of the Press Council of India with editors and senior journalists of East-West Media Group Ltd on Wednesday. The event was held in the EWMGL conference room at Bashundhara Residential Area. The visiting team of journalists, mostly editors from prominent Indian newspapers, also made a tour of the EWMGL media outlets. The visitors got fully apprised of the state of the mass media in Bangladesh. Speaking on the occasion, the Press Council chair underscored the need for more interaction and communications between the journalists of two countries. Journalists from both sides also echoed Justice Prasad’s views on the matter and voiced concern over the mounting threat of terrorism, militancy and conspiracies against their respective countries. -
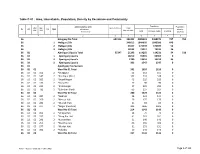
Table C-01 : Area, Households, Population, Density by Residence and Community
Table C-01 : Area, Households, Population, Density by Residence and Community Administrative Unit Population Population UN / MZ / Area in Acres Total ZL UZ Vill RMO Residence density WA MH Households Community Total In Households Floating [sq. km] 1 2 3 4 5 6 7 8 36 Habiganj Zila Total 651516 393302 2089001 2088274 727 792 36 1 Habiganj Zila 346612 1844035 1843386 649 36 2 Habiganj Zila 33157 171749 171697 52 36 3 Habiganj Zila 13533 73217 73191 26 36 02 Ajmiriganj Upazila Total 55347 21293 114265 114231 34 510 36 02 1 Ajmiriganj Upazila 18210 99365 99365 0 36 02 2 Ajmiriganj Upazila 2780 13353 13319 34 36 02 3 Ajmiriganj Upazila 303 1547 1547 0 36 02 Ajmiriganj Paurashava 36 02 01 Ward No-01 Total 341 1610 1610 0 36 02 01 103 2 *Durgapur 52 151 151 0 36 02 01 147 2 *Fatehpur (Part) 102 518 518 0 36 02 01 169 2 *Gupal Nagar 43 229 229 0 36 02 01 173 2 *Gusai Pur 27 90 90 0 36 02 01 235 2 *Krisnanagar 57 295 295 0 36 02 01 733 2 *Sukribari (Part) 60 327 327 0 36 02 02 Ward No-02 Total 280 1424 1424 0 36 02 02 087 2 *Debhati 25 121 121 0 36 02 02 260 2 *Mesuri Hati 29 175 175 0 36 02 02 281 2 *Munshi Hati 21 83 83 0 36 02 02 377 2 *Nogar (Paschim) 205 1045 1045 0 36 02 03 Ward No-03 Total 214 1143 1143 0 36 02 03 093 2 *Dhupa Hati 16 79 79 0 36 02 03 157 2 *Gang Par Hati 41 261 261 0 36 02 03 241 2 *Kumar Hati 31 140 140 0 36 02 03 253 2 *Maidha Para 66 369 369 0 36 02 03 277 2 *Mudak Hati 31 151 151 0 36 02 03 383 2 *Fokabaj 29 143 143 0 36 02 04 Ward No-04 Total 237 1133 1133 0 RMO: 1 = Rural, 2 = Urban and 3 = Other Urban Page 1 of 103 Table C-01 : Area, Households, Population, Density by Residence and Community Administrative Unit Population Population UN / MZ / Area in Acres Total ZL UZ Vill RMO Residence density WA MH Households Community Total In Households Floating [sq. -

One Year After the Rana Plaza Catastrophe : Slow Progress and Insufficient Compensation
FIDH - International Federation for Human Rights Odhikar One Year After the Rana Plaza Catastrophe : Slow Progress and Insufficient Compensation One year has passed since the collapse of the Rana Plaza in Dhaka, Bangladesh, and survivors and victims' families are still waiting for adequate compensation. Safety conditions and respect for workers' rights in garment factories in Bangladesh remain concerning. Background: On April 24, 2013 in Savar, in the suburb of Dhaka, Bangladesh, the “Rana Plaza” factory collapsed, killing at least 1,130 people and injuring more than 2,000.1 This eight-storey structure, built and operating in violation of minimal safety standards, held five ready-made garment factories which supplied some thirty European and American clothing brands. In the aftermath of this disaster, a variety of international multi-stakeholder initiatives were created, bringing together global brands, trade unions, NGOs and the International Labour Organization (ILO), in order to improve the building and fire safety codes of textile factories in Bangladesh, as well as to compensate Rana Plaza survivors and victims' families. Some multinational companies were quick to provide one-off payments to victims, others have not yet contributed to the compensation fund, and some continue to insist that they hadn't placed any orders with the five Rana Plaza clothing factories. Q&A by FIDH and its member organisation in Bangladesh Odhikar 1- Have those responsible for this catastrophe been identified? Have they been held accountable? Several actors share responsibility for this tragedy. The primary responsibility falls on the Bangladeshi authorities, who failed in their obligation to protect workers. The private actors implicated in the disaster also share responsibility, namely the owners of the Rana Plaza building and of the garment factories it held, as well as the multinational corporations which sourced from those garment factories. -

Mamoni Health Systems Strengthening Activity
MaMoni Health Systems Strengthening Activity Quarterly Report January 1 – March 31, 2015 Submitted May 15, 2015 This document is made possible by the generous support of the American people through the support of the Office of Population, Health, Nutrition and Education, United States Agency for International Development, Bangladesh (USAID/Bangladesh) under the terms of Associate Cooperative Agreement No. AID-388-LA-13-00004 through MCHIP, managed by Jhpiego Corporation. The contents of this document are the responsibility of Jhpiego Corporation and do not necessarily reflect the views of USAID or the United States Government. Cover Photo Credit: Using a computer tablet, MaMoni HSS data collectors enter population information into a national registry system in Madhabpur Upazila, where the Routine Health Information System (RHIS) project is being piloted. Directorate General Health Services and Directorate General Family Planning service providers will use this electronic information to track clients and ensure services to the families. Photo Credit: Shimantik/Save the Children. MaMoni HSS – Year Two Second Quarterly Report April 2015 2 TABLE OF CONTENTS 1. Introduction ...................................................................................................................................7 2. Program Objectives and Key Activities ............................................................................................8 3. Results for Year 1 ........................................................................................................................ -

Media Release: Pakistan
International JACQUELINE PARK IFJ Asia-Pacific Director Federation ELISABETH COSTA of Journalists General Secretary Situation Report: Bangladesh, December 2012 Journalism in the Political Crossfire The deeply polarising effect of politics in Bangladesh has been felt in various domains, the media included. As Bangladesh prepares for another round of general elections to the national parliament at the end of 2013, political discord and disharmony are rising. The years since the last general elections in 2008 have been politically stable since the Awami League (AL), the party that led the country’s movement for liberation from Pakistan, has secured alongside its allies, an impregnable majority in parliament. But there has not been any manner of political concord. Opposition boycotts of the proceedings of parliament and allegations of unfair pressures on political and civil society elements inclined towards the opposition, have been frequent. In June 2011, the Government of Sheikh Hasina Wajed piloted the Fifteenth Amendment to the Constitution through Bangladesh’s parliament, providing another potential flashpoint for acrimony as elections near. Among other things, the Fifteenth Amendment does away with the process of conducting national elections under a neutral caretaker government. It reaffirms Islam as state religion, but then enshrines the values of secularism and freedom of faith. It officially raises Sheikh Mujibur Rahman to the status of “father of the nation”, mandates that his portraits will be displayed at key sites of the Bangladeshi state and the offices of its main functionaries, and incorporates into the official text of the constitution, two historic speeches that he made in March 1971 as Bangladesh broke away from Pakistan. -

Media Coverage Links
Pneumonia in Bangladesh: Where we are and what need to do Media Coverage Links 1. icddr,b press release - https://www.icddrb.org/quick-links/press-releases?id=98&task=view 2. UNB (news agency) - http://www.unb.com.bd/category/Bangladesh/pneumonia-kills-24000- plus-children-in-bangladesh-every-year/60359 3. The Daily Star - https://www.thedailystar.net/city/news/juvenile-pneumonia-ignored-due- covid-pandemic-experts-1993417 4. Dhaka Tribune (English) https://www.dhakatribune.com/bangladesh/2020/11/11/every-hour- pneumonia-kills-3-children-in-bangladesh 5. Dhaka Tribune (Bangla) https://bit.ly/3ngKe2H 6. The New Age - https://www.newagebd.net/article/121327/67-children-die-of-pneumonia- daily:-study 7. The Observer BD - https://www.observerbd.com/news.php?id=284093 8. The Business Standard - https://tbsnews.net/bangladesh/health/67-children-die-pneumonia- every-day-bangladesh-156727 9. The Financial Express - https://www.thefinancialexpress.com.bd/health/pneumonia-kills-67- children-every-day-in-bangladesh-1605157926 10. The Independent - http://www.theindependentbd.com/post/255893 11. Bangladesh Post (print and online – English) - https://www.bangladeshpost.net/posts/pneumonia-still-number-one-killer-of-bangladeshi- children-46768 12. The Daily Sun (print and online – English) - https://www.daily- sun.com/post/517196/Preventing-child-death-from-pneumonia-requires-multi-system-approach 13. The New Nation (print and online – English) - http://thedailynewnation.com/news/268690/67-children-die-of-pneumonia-every-day-in- bangladesh.html 14. The Bangladesh and Beyond (online – English) - https://thebangladeshbeyond.com/preventing- child-death-from-pneumonia-requires-multi-system-approach-health-experts/ 15. -

Bangladesh: Human Rights Report 2015
BANGLADESH: HUMAN RIGHTS REPORT 2015 Odhikar Report 1 Contents Odhikar Report .................................................................................................................................. 1 EXECUTIVE SUMMARY ............................................................................................................... 4 Detailed Report ............................................................................................................................... 12 A. Political Situation ....................................................................................................................... 13 On average, 16 persons were killed in political violence every month .......................................... 13 Examples of political violence ..................................................................................................... 14 B. Elections ..................................................................................................................................... 17 City Corporation Elections 2015 .................................................................................................. 17 By-election in Dohar Upazila ....................................................................................................... 18 Municipality Elections 2015 ........................................................................................................ 18 Pre-election violence .................................................................................................................. -
Caught Between Fear and Repression
CAUGHT BETWEEN FEAR AND REPRESSION ATTACKS ON FREEDOM OF EXPRESSION IN BANGLADESH Amnesty International is a global movement of more than 7 million people who campaign for a world where human rights are enjoyed by all. Our vision is for every person to enjoy all the rights enshrined in the Universal Declaration of Human Rights and other international human rights standards. We are independent of any government, political ideology, economic interest or religion and are funded mainly by our membership and public donations. © Amnesty International 2017 Cover design and illustration: © Colin Foo Except where otherwise noted, content in this document is licensed under a Creative Commons (attribution, non-commercial, no derivatives, international 4.0) licence. https://creativecommons.org/licenses/by-nc-nd/4.0/legalcode For more information please visit the permissions page on our website: www.amnesty.org Where material is attributed to a copyright owner other than Amnesty International this material is not subject to the Creative Commons licence. First published in 2017 by Amnesty International Ltd Peter Benenson House, 1 Easton Street, London WC1X 0DW, UK Index: ASA 13/6114/2017 Original language: English amnesty.org CONTENTS FREEDOM OF EXPRESSION TIMELINE 4 EXECUTIVE SUMMARY & METHODOLOGY 6 1. ACTIVISTS LIVING IN FEAR WITHOUT PROTECTION 13 2. A MEDIA UNDER SIEGE 27 3. BANGLADESH’S OBLIGATIONS UNDER INTERNATIONAL LAW 42 4. BANGLADESH’S LEGAL FRAMEWORK 44 5. CONCLUSION AND RECOMMENDATIONS 57 Glossary AQIS - al-Qa’ida in the Indian Subcontinent -

Zila Report : Habiganj
POPULATION & HOUSING CENSUS 2011 ZILA REPORT : HABIGANJ Bangladesh Bureau of Statistics Statistics and Informatics Division Ministry of Planning BANGLADESH POPULATION AND HOUSING CENSUS 2011 Zila Report: HABIGANJ October 2015 BANGLADESH BUREAU OF STATISTICS (BBS) STATISTICS AND INFORMATICS DIVISION (SID) MINISTRY OF PLANNING GOVERNMENT OF THE PEOPLE’S REPUBLIC OF BANGLADESH ISBN-978-984-33-8637-3 COMPLIMENTARY Published by Bangladesh Bureau of Statistics (BBS) Statistics and Informatics Division (SID) Ministry of Planning Website: www.bbs.gov.bd This book or any portion thereof cannot be copied, microfilmed or reproduced for any commercial purpose. Data therein can, however, be used and published with acknowledgement of their sources. Contents Page Message of Honorable Minister, Ministry of Planning …………………………………………….. vii Message of Honorable State Minister, Ministry of Finance and Ministry of Planning …………. ix Foreword ……………………………………………………………………………………………….. xi Preface …………………………………………………………………………………………………. xiii Zila at a Glance ………………………………………………………………………………………... xv Physical Features ……………………………………………………………………………………... xix Zila Map ………………………………………………………………………………………………… xx Geo-code ………………………………………………………………………………………………. xxi Chapter-1: Introductory Notes on Census ………………………………………………………….. 1 1.1 Introduction ………………………………………………………………………………… 1 1.2 Census and its periodicity ………………………………………………………………... 1 1.3 Objectives ………………………………………………………………………………….. 1 1.4 Census Phases …………………………………………………………………………… 2 1.5 Census Planning …………………………………………………………………………. -

Bangladesh Adolescent Health and Wellbeing Survey News Coverage
Bangladesh Adolescent Health and Wellbeing Survey News Coverage English Media 1. Editorial in Prothom Alo: https://en.prothomalo.com/opinion/editorial/take-actions-to-stop-sexual- harassment-of-teenage-girls 2. UNB (news agency, English online) - http://www.unb.com.bd/category/Bangladesh/over-90pc- adolescents-using-mobile-phones-in-bangladesh-survey/64755 3. The Daily Star (English, online) - https://www.thedailystar.net/health/news/hygienic-menstrual- practices-very-low-among-adolescent-girls-survey-2043185 4. The Daily Star (English, print and online) - https://www.thedailystar.net/city/news/usage-menstrual- products-high-hygiene-low-survey-2043569?amp 5. The Daily Star (Bangla, online) - http://bit.ly/2Ns3bDe 6. New Age (English, print and online) - https://www.newagebd.net/article/129953/survey-finds-poor- state-of-menstrual-hygiene-practices-among-adolescents 7. Dhaka Tribune (English, print and online) - https://www.dhakatribune.com/bangladesh/2021/02/12/survey-over-90-adolescents-use-mobile-phones- in-bangladesh 8. The Financial Express (English, print and online) - https://today.thefinancialexpress.com.bd/metro- news/over-90pc-adolescents-using-mobile-phones-in-bangladesh-survey-1613146189 9. The Business Standard (English, print and online) - https://tbsnews.net/bangladesh/health/76-85- adolescents-eat-adequately-diverse-food-200482 10. The Observer (English, print and online) - https://www.observerbd.com/news.php?id=298673 Bangla Media 1. Editorial in Prothom Alo 2. Prothom Alo (Bangla, print) 3. Prothom Alo (Bangla, online) - http://bit.ly/3pjiQBT 4. Jugantor (Bangla, print and online) - http://bit.ly/3pgQAje 5. Desh Rupantor (Bangla, print and online) - https://www.deshrupantor.com/capital/2021/02/12/276395 6.