Procedure Codes
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Anorectal Disorders Satish S
Gastroenterology 2016;150:1430–1442 Anorectal Disorders Satish S. C. Rao,1 Adil E. Bharucha,2 Giuseppe Chiarioni,3,4 Richelle Felt-Bersma,5 Charles Knowles,6 Allison Malcolm,7 and Arnold Wald8 1Division of Gastroenterology and Hepatology, Augusta University, Augusta, Georgia; 2Department of Gastroenterology and Hepatology, Mayo College of Medicine, Rochester, Minnesota; 3Division of Gastroenterology of the University of Verona, Azienda Ospedaliera Universitaria Integrata di Verona, Verona, Italy; 4Division of Gastroenterology and Hepatology and UNC Center for Functional GI and Motility Disorders, University of North Carolina at Chapel Hill, Chapel Hill, North Carolina; 5Department of Gastroenterology/Hepatology, VU Medical Center, Amsterdam, The Netherlands; 6National Centre for Bowel Research and Surgical Innovation, Blizard Institute, Queen Mary University of London, London, United Kingdom; 7Division of Gastroenterology, Royal North Shore Hospital, and University of Sydney, Sydney, Australia; 8Division of Gastroenterology, University of Wisconsin School of Medicine and Public Health, Madison, Wisconsin This report defines criteria and reviews the epidemiology, questionnaires and bowel diaries are correlated,5 some pathophysiology, and management of the following com- patients may not accurately recall bowel symptoms6; hence, mon anorectal disorders: fecal incontinence (FI), func- symptom diaries may be more reliable. tional anorectal pain, and functional defecation disorders. In this report, we examine the prevalence and patho- FI is defined as the recurrent uncontrolled passage of fecal physiology of anorectal disorders, listed in Table 1,and material for at least 3 months. The clinical features of FI provide recommendations for diagnostic evaluation and are useful for guiding diagnostic testing and therapy. management. These supplement practice guidelines rec- ANORECTAL Anorectal manometry and imaging are useful for evalu- ommended by the American Gastroenterological Associa- fl ating anal and pelvic oor structure and function. -

Research Article Magnetic Resonance Sialography Findings of Submandibular Ducts Imaging
Hindawi Publishing Corporation BioMed Research International Volume 2013, Article ID 417052, 6 pages http://dx.doi.org/10.1155/2013/417052 Research Article Magnetic Resonance Sialography Findings of Submandibular Ducts Imaging Nezahat Karaca ErdoLan,1 Canan Altay,2 Nesibe Özenler,3 TuLba Bozkurt,1 Engin Uluç,1 Berna Dirim Mete,1 and Esmail Özdemir4 1 Department of Radiology, Izmir Ataturk¨ Research and Training Hospital, Basın Sitesi, Karabaglar,˘ 35360 Izmir, Turkey 2 Department of Radiology, Medical School, Dokuz Eylul University, Inciralti, 35340 Izmir, Turkey 3 Department of Radiology, Balıkesir Ataturk¨ State Hospital, Yıldız Mahallesi Soma Caddesi No. 1, 10100 Balıkesir, Turkey 4 Universal Ege Health Hospital, 35220 Izmir, Turkey Correspondence should be addressed to Canan Altay; [email protected] Received 2 April 2013; Revised 29 May 2013; Accepted 12 June 2013 Academic Editor: Yoshito Tsushima Copyright © 2013 Nezahat Karaca Erdogan˘ et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Purpose. We aimed to assess the problem solving capability of magnetic resonance sialography (MR sialography), a noninvasive method for imaging submandibular gland ducts and determining duct-related pathologies, by comparing diseased and healthy cases. Materials and Methods. We conducted radiological assessment on a total of 60 submandibular glands (mean age 44.7) in 20 cases and 10 volunteers. MR sialography examinations were conducted with single-shot fast spin-echo sequence by using a surface coil placed on the submandibular gland. Each gland was evaluated in terms of the length, width and stricture of the main duct, as well as the difference between the intraparenchymal duct width, and the main duct width. -

Smartphone-Based Dilated Fundus Photography and Near Visual Acuity Testing As Inexpensive Screening Tools to Detect Referral Warranted Diabetic Eye Disease
Smartphone-Based Dilated Fundus Photography and Near Visual Acuity Testing as Inexpensive Screening Tools to Detect Referral Warranted Diabetic Eye Disease BRIAN C. TOY, MD,*† DAVID J. MYUNG, MD, PHD,*† LINGMIN HE, MD,*† CAROLYN K. PAN, MD,*† ROBERT T. CHANG, MD,* ALISON POLKINHORNE, MA,‡ DOUGLAS MERRELL, BS,‡ DOUG FOSTER, MBA,‡ MARK S. BLUMENKRANZ, MD* Purpose: To compare clinical assessment of diabetic eye disease by standard dilated examination with data gathered using a smartphone-based store-and-forward teleoph- thalmology platform. Methods: 100 eyes of 50 adult patients with diabetes from a health care safety-net ophthalmology clinic. All patients underwent comprehensive ophthalmic examination. Concurrently, a smartphone was used to estimate near visual acuity and capture anterior and dilated posterior segment photographs, which underwent masked, standardized review. Quantitative comparison of clinic and smartphone-based data using descriptive, kappa, Bland-Altman, and receiver operating characteristic analyses was performed. Results: Smartphone visual acuity was successfully measured in all eyes. Anterior and posterior segment photography was of sufficient quality to grade in 96 and 98 eyes, respectively. There was good correlation between clinical Snellen and smartphone visual acuity measurements (rho = 0.91). Smartphone-acquired fundus photographs demon- strated 91% sensitivity and 99% specificity to detect moderate nonproliferative and worse diabetic retinopathy, with good agreement between clinic and photograph grades (kappa = 0.91 ± 0.1, P , 0.001; AUROC = 0.97, 95% confidence interval, 0.93–1). Conclusion: The authors report a smartphone-based telemedicine system that demon- strated sensitivity and specificity to detect referral-warranted diabetic eye disease as a proof-of-concept. Additional studies are warranted to evaluate this approach to expanding screening for diabetic retinopathy. -

Reoperative Techniques and Management in Hirschsprung Disease: a Narrative Review
14 Review Article Reoperative techniques and management in Hirschsprung disease: a narrative review Farokh R. Demehri^, Belinda H. Dickie Department of Surgery, Boston Children’s Hospital, Boston, MA, USA Contributions: (I) Conception and design: All authors; (II) Administrative support: None; (III) Provision of study materials or patients: None; (IV) Collection and assembly of data: All authors; (V) Data analysis and interpretation: All authors; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors Correspondence to: Farokh R. Demehri, MD. Department of Surgery, Boston Children’s Hospital, 300 Longwood Ave, Fegan 3, Boston, MA 02115, USA. Email: [email protected]. Abstract: The majority of children who undergo operative management for Hirschsprung disease have favorable results. A subset of patients, however, have long-term dysfunctional stooling, characterized by either frequent soiling or obstructive symptoms. The evaluation and management of a child with poor function after pull-through for Hirschsprung disease should be conducted by an experienced multidisciplinary team. A systematic workup is focused on detecting pathologic and anatomic causes of pull- through dysfunction. This includes an exam under anesthesia, pathologic confirmation including a repeat biopsy, and a contrast enema, with additional studies depending on the suspected etiology. Obstructive symptoms may be due to technique-specific types of mechanical obstruction, histopathologic obstruction, or dysmotility—each of which may benefit from reoperative surgery. The causes of soiling symptoms include loss of the dentate line and damage to the anal sphincter, which generally do not benefit from revision of the pull-through, and pseudo-incontinence, which may reveal underlying obstruction. A thorough understanding of the types of complications associated with various pull-through techniques aids in the evaluation of a child with postoperative dysfunction. -

ICD~10~PCS Complete Code Set Procedural Coding System Sample
ICD~10~PCS Complete Code Set Procedural Coding System Sample Table.of.Contents Preface....................................................................................00 Mouth and Throat ............................................................................. 00 Introducton...........................................................................00 Gastrointestinal System .................................................................. 00 Hepatobiliary System and Pancreas ........................................... 00 What is ICD-10-PCS? ........................................................................ 00 Endocrine System ............................................................................. 00 ICD-10-PCS Code Structure ........................................................... 00 Skin and Breast .................................................................................. 00 ICD-10-PCS Design ........................................................................... 00 Subcutaneous Tissue and Fascia ................................................. 00 ICD-10-PCS Additional Characteristics ...................................... 00 Muscles ................................................................................................. 00 ICD-10-PCS Applications ................................................................ 00 Tendons ................................................................................................ 00 Understandng.Root.Operatons..........................................00 -

Ophthalmic Imaging Guidance
Ophthalmic Services Guidance Ophthalmic Imaging March 2021 Review: February 2022 18 Stephenson Way, London, NW1 2HD T. 020 7935 0702 [email protected] rcophth.ac.uk @RCOphth © The Royal College of Ophthalmologists 2021 All rights reserved For permission to reproduce and of the content contained herein please contact [email protected] Contents 1 Introduction 3 2 Corneal and anterior segment imaging 3 Anterior segment photography 3 3 Retinal imaging 5 Colour fundus photography 5 4 Scanning laser ophthalmoscopy (SLO) 6 Overview 6 Monochromatic imaging 7 Fundus autofluorescence (FAF) 7 Ultra-Widefield (UWF) imaging 8 Fundus Fluorescein Angiography (FFA) 9 Indocyanine Green Angiography (ICG) 9 Vitreous, Retinal and Choroidal Optical Coherence Tomography (OCT) 9 Optical Coherence Tomography Angiography (OCTA) 10 Adaptive optics 11 Laser Doppler Flowmetry 11 Retinal oximetry 12 5 Optic nerve head and peripapillary imaging 12 Optic disc photography 12 Scanning laser tomography 13 Scanning laser polarimetry 13 Optic nerve head and peripapillary Optical Coherence Tomography 14 6 External, oculoplastic and adnexal imaging 14 External Photography 14 3D Digital Stereophotogrammetry 14 Doppler flow imaging of the superior ophthalmic vein 15 7 Ultrasonography 15 Ocular and Orbital Ultrasound 15 A-Scan 15 B-Scan 16 Ultrasound biomicroscopy (UBM) 16 Colour flow mapping (CFM) and spectral Doppler techniques 17 8 Networking and imaging software 17 Networking 17 DICOM and DICOM Modality Worklist standards 18 Data storage, picture archiving and communication system (PACS) 18 Electronic medical records (EMR) 18 Summary 19 9 Information governance 19 10 Telemedicine and virtual clinics 19 11 Consent 20 12 Staffing 20 13 Authors 21 2021/PROF/438 2 1 Introduction Ophthalmic imaging is an integral part of the work of all ophthalmic departments. -

Bilateral Exudative Retinal Detachment in a Patient with Cerebral Venous Sinus Thrombosis: a Case Report
Bilateral exudative retinal detachment in a patient with cerebral venous sinus thrombosis: a case report Liang Li The second Xiangya Hospital, Central South University Ling Gao ( [email protected] ) Second Xiangya Hospital https://orcid.org/0000-0002-9850-2038 Case report Keywords: exudative retinal detachment, cerebral venous sinus thrombosis, elschnig spot, retinal capillary ischemia Posted Date: June 6th, 2019 DOI: https://doi.org/10.21203/rs.2.9789/v1 License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License Page 1/8 Abstract Background: Cerebral venous sinus thrombosis (CVST) is a rare cerebrovascular disease, it’s ocular symptoms often characterized by a subacute bilateral visual loss, or diplopia and paralysis of eye movements. Fundus examination usually presents as bilateral papilledema and other ocular signs are rare. We report a case of bilateral multiple retinal detachments and nally diagnosed as CVST. Case presentation: A 49-year old woman with progressive headache and bilateral vision deterioration visited our clinic. Ophthaomological examinations including medical history, best-corrected visual acuity, intraocular pressure, slit-lamp biomicroscopy, fundus ophthalmoscopy, uorescein angiography and Optical coherence tomography and head Magnetic Resonance Venogram (MRV) was also performed. Blood tests for ruling out systemic diseases were also performed. Fundus exam revealed bilateral multiple retinal detachment with sub-retinal uid and blurred disc margin. Fluorescein angiography (FA) revealed early hypouorescence in the background stage, multiple pinpoint leakages at the level of retinal pigment epithelium (RPE), and late pooling to outline the boundary of retinal detachment, with some of the leakage shaped as multiple circles in the late stage of FA. -
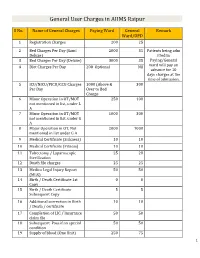
General User Charges in AIIMS Raipur
General User Charges in AIIMS Raipur S No. Name of General Charges Paying Ward General Remark Ward/OPD 1 Registration Charges 200 25 2 Bed Charges Per Day (Sami 2000 35 Patients being adm Deluxe) itted in 3 Bed Charges Per Day (Deluxe) 3000 35 Paying/General 4 Diet Charges Per Day 200 Optional Nil ward will pay an advance for 10 days charges at the time of admission. 5 ICU/NICU/PICU/CCU Charges 1000 (Above & 300 Per Day Over to Bed Charge 6 Minor Operation in OT/MOT 250 100 not mentioned in list, under L A 7 Minor Operation in OT/MOT 1000 300 not mentioned in list, under G A 8 Major Operation in OT, Not 2000 1000 mentioned in list under G A 9 Medical Certificate (Sickness) 10 10 10 Medical Certificate (Fitness) 10 10 11 Tubectomy / Laparoscopic 25 20 Sterilization 12 Death file charges 25 25 13 Medico Legal Injury Report 50 50 (MLR) 14 Birth / Death Certificate 1st 0 0 Copy 15 Birth / Death Certificate 5 5 Subsequent Copy 16 Additional correction in Birth 10 10 / Death / certificate 17 Completion of LIC / Insurance 50 50 claim file 18 Subsequent Pass if on special 50 50 condition 19 Supply of blood (One Unit) 250 75 1 20 Medical Board Certificate 500 500 On Special Case User Charges for Investigations in AIIMS Raipur S No. Name of Investigations Paying General Remark Ward Ward/OPD Anaesthsia 1 ABG 75 50 2 ABG ALONGWITH 150 100 ELECTROLYTES(NA+,K+)(Na,K) 3 ONLY ELECTROLYTES(Na+,K+,Cl,Ca+) 75 50 4 ONLY CALCIUM 50 25 5 GLUCOSE 25 20 6 LACTATE 25 20 7 UREA. -

Curriculum Vitae
Curriculum Vitae INFORMAZIONI PERSONALI Nome SERGIO Cognome SALERNO Recapiti Sezione di Radiologia DIBIMEF E-mail [email protected] FORMAZIONE TITOLI • Studente in Medicina dal novembre 1986 al novembre 1992. • Specializzando in Radiodiagnostica dal Novembre 1992 al Dicembre 1996. • Esperienza come Assistente in Formazione presso l'Istituto di Radiologia della Università degli studi di Trieste diretto dal Prof. L. Dalla Palma (maggio 1994 e febbraio 1995). • Fellow al Diagnostic Radiology Department del Hammersmith Hospital di Londra (marzo-luglio 1996). • Dottorando di Ricerca in Radiologia Oncologica (ciclo XII) dal novembre 1997 al febbraio 2000. • Fellow al Diagnostic Radiology Department del St' Georges Hospital di Londra (aprile-luglio 1997). • Research Fellow del CIRSE al Diagnostic Radiology Department del St' Georges Hospital di Londra (luglio-ottobre 1999). ATTIVITA' DIDATTICA • Componente del Collegio dei Docenti del Dottorato di Ricerca in Scienze Stomatologiche dal Ciclo XVIII. • Docente nel Corso integrato di Diagnostica per Immagini del Corso di Laurea in Medicina e Chirurgia dell’Università di Palermo dall’anno accademico 2001-2002 al 2007-2008. • Docente del Corso di Laurea in Fisioterapia per la materia Diagnostica per Immagini dell’Università di Palermo dall’anno accademico 2002-2003 al 2007-2008. • Docente del Corso di Laurea in Tecniche della Riabilitazione Neuropsicomotoria per la materia Diagnostica per Immagini dell’Università di Palermo dall’anno accademico 2003-2004 al 2007-2008. • Docente del Corso di Laurea in Tecniche della Riabilitazione Neuropsicomotoria per la materia Neuroradiologia nell’ anno accademico nel 2008-2009. • Docente del Corso di Laurea in Tecniche della Riabilitazione Psichiatrica per la materia Diagnostica per Immagini dell’Università di Palermo dall’anno accademico 2004-2005 al 2006-2007. -

Procedure Codes for Physician: Radiology
NEW YORK STATE MEDICAID PROGRAM PHYSICIAN - PROCEDURE CODES SECTION 4 - RADIOLOGY Physician – Procedure Codes, Section 4 - Radiology Table of Contents GENERAL INSTRUCTIONS ............................................................................................................ 4 GENERAL RULES AND INFORMATION ......................................................................................... 6 MMIS RADIOLOGY MODIFIERS .................................................................................................... 8 DIAGNOSTIC RADIOLOGY (DIAGNOSTIC IMAGING)................................................................. 9 HEAD AND NECK.................................................................................................................... 9 CHEST .................................................................................................................................. 10 SPINE AND PELVIS .............................................................................................................. 11 UPPER EXTREMITIES .......................................................................................................... 12 LOWER EXTREMITIES ......................................................................................................... 13 ABDOMEN ............................................................................................................................ 14 GASTROINTESTINAL TRACT ............................................................................................... 15 URINARY -

(DICOM) Supplement 91: Ophthalmic Photography Image SOP Classes
Digital Imaging and Communications in Medicine (DICOM) Supplement 91: Ophthalmic Photography Image SOP Classes Prepared by: DICOM Standards Committee 1300 N. 17th Street Suite 1847 Rosslyn, Virginia 22209 USA VERSION: Final Text, September 29, 2004. Supplement 91 – Ophthalmic Photography Image SOP Classes Page 2 Table of Contents Table of Contents ................................................................................................................................................. 2 Foreword ............................................................................................................................................................... 4 Scope and Field of Application ............................................................................................................................ 4 Part 3 Additions..................................................................................................................................................... 6 Part 3 Annex A Additions ..................................................................................................................................... 8 A.41 Ophthalmic Photography 8 Bit Image Information Object Definition ................................................ 9 A.41.1 Ophthalmic Photography 8 Bit Image IOD Description............................................................... 9 A.41.2 Ophthalmic Photography 8 Bit Image IOD Entity-Relationship Model ...................................... 9 A.41.3 Ophthalmic Photography 8 Bit Image IOD Modules -

12.1 Radiology
12.1 Radiology Southwest Medical Associates (SMA) provides radiology services at multiple locations. The facility located at 888 S. Rancho Drive offers extended hours for urgent situations. SMA offers additional facilities, which operate during normal business hours (please call the individual facility for office hours). Special radiology studies such as CT, Ultrasound, Fluoroscopy, and IVP’s require appointments. Appointments can be made by contacting the scheduling department at (702) 877-5390. Plain film studies do not require a referral or an appointment; however, they do require an order signed by a physician. Contact the Radiology Department at (702) 877-5125 option 5 with any questions. NAME/LOCATION PHONE HOURS PROCEDURES Rancho/Charleston (702) 877-5125 S-S 24 hours Scheduled procedures 888 S. Rancho Dr. 24 hours for emergencies STAT, Expedited Ultrasounds, CT Scans Diagnostic Mammography DEXA Scans N. Tenaya Satellite (702) 243-8500 S-S 7 a.m. - 7 p.m. Plain film studies 2704 N. Tenaya Way Screening Mammography Routine Ultrasounds Routine CT Scans S. Eastern Satellite (702) 737-1880 S-S 7 a.m. - 7 p.m. Plain film studies 4475 S. Eastern Ave. Screening Mammography DEXA Scans Routine Ultrasounds STAT, Expedited, Routine CT Scans Siena Heights Satellite (702) 617-1227 S-S 7 a.m. – 7 p.m. Plain film studies 2845 Siena Heights Screening Mammography Routine Ultrasounds Montecito Satellite (702) 750-7424 S-S 7 a.m. – 7 p.m. Plain Film Studies 7061 Grand Montecito Pkwy Routine Ultrasounds Sunrise Satellite (702) 459-7424 M-F 8 a.m. - 5 p.m. Plain film studies 540 N.