Bed Bugs in Medical Facilities
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

1 February 2021
February 2021 Harriet Tubman was born around 1820 on a plantation in Dorchester County, Maryland. She had eight brothers and sisters; due to the realities of slavery they were eventually forced apart. At the age of 12 her desire for justice became apparent. She stepped between an enslaved person and the overseer who threw a weight that struck Harriet in the head. This good deed left her with headaches and narcolepsy for the rest of her life. In 1840 her father was set free by his previous owner. The new owner refused to recognize this and kept Harriet, her mother, and the rest of her siblings in bondage. In 1844, Harriet married John Tubman who was a free black man and changed her last name. This marriage was not good and with the knowledge of two of her brothers about to be sold provoked Harriet to plan an escape. September 17, 1849, Harriet and her two brothers escaped from the Maryland plantation. Although her brothers changed their minds and went back. With the help of the Underground Railroad Harriet persevered and traveled 90 miles north to Pennsylvania and freedom. Harriet was not satisfied living free on her own and she wanted freedom for her loved ones and friends, too. She returned to the south to lead her niece and her niece’s children to Philadelphia via the Underground Railroad. The 1850 Fugitive Slave Act allowed fugitive and freed workers in the north to be captured and enslaved, which in turn made Harriet’s job with the Underground Railroad much harder. -

Myiasis During Adventure Sports Race
DISPATCHES reexamined 1 day later and was found to be largely healed; Myiasis during the forming scar remained somewhat tender and itchy for 2 months. The maggot was sent to the Finnish Museum of Adventure Natural History, Helsinki, Finland, and identified as a third-stage larva of Cochliomyia hominivorax (Coquerel), Sports Race the New World screwworm fly. In addition to the New World screwworm fly, an important Old World species, Mikko Seppänen,* Anni Virolainen-Julkunen,*† Chrysoimya bezziana, is also found in tropical Africa and Iiro Kakko,‡ Pekka Vilkamaa,§ and Seppo Meri*† Asia. Travelers who have visited tropical areas may exhibit aggressive forms of obligatory myiases, in which the larvae Conclusions (maggots) invasively feed on living tissue. The risk of a Myiasis is the infestation of live humans and vertebrate traveler’s acquiring a screwworm infestation has been con- animals by fly larvae. These feed on a host’s dead or living sidered negligible, but with the increasing popularity of tissue and body fluids or on ingested food. In accidental or adventure sports and wildlife travel, this risk may need to facultative wound myiasis, the larvae feed on decaying tis- be reassessed. sue and do not generally invade the surrounding healthy tissue (1). Sterile facultative Lucilia larvae have even been used for wound debridement as “maggot therapy.” Myiasis Case Report is often perceived as harmless if no secondary infections In November 2001, a 41-year-old Finnish man, who are contracted. However, the obligatory myiases caused by was participating in an international adventure sports race more invasive species, like screwworms, may be fatal (2). -

Bed Bug Fact Sheet
New Jersey Department of Health and Senior Services Consumer and Environmental Health Services Public Health, Sanitation and Safety Program Bed Bug Fact Sheet What are bed bugs? Bed bugs are small insects that feed on the blood of mammals and birds. Adult bed bugs are oval, wingless and rusty red colored, and have flat bodies, antennae and small eyes. They are visible to the naked eye, but often hide in cracks and crevices. When bed bugs feed, their bodies swell and become a brighter red. In homes, bed bugs feed primarily on the blood of humans, usually at night when people are sleeping. What does a bed bug bite feel and look like? Typically, the bite is painless and rarely awakens a sleeping person. However, it can produce large, itchy welts on the skin. Welts from bed bug bites do not have a red spot in the center – those welts are more characteristic of flea bites. Are bed bugs dangerous? Although bed bugs may be a nuisance to people, they are not known to spread disease. They are known to cause allergic reactions from their saliva in sensitive people. How long do bed bugs live? The typical life span of a bed bug is about 10 months. They can survive for weeks to months without feeding. How does a home become infested with bed bugs? In most cases, bed bugs are transported from infested areas to non-infested areas when they cling onto someone’s clothing, or crawl into luggage, furniture or bedding that is then brought into homes. How do I know if my home is infested with bed bugs? If you have bed bugs, you may also notice itchy welts on you or your family member’s skin. -

COVID-19 Mrna Pfizer- Biontech Vaccine Analysis Print
COVID-19 mRNA Pfizer- BioNTech Vaccine Analysis Print All UK spontaneous reports received between 9/12/20 and 22/09/21 for mRNA Pfizer/BioNTech vaccine. A report of a suspected ADR to the Yellow Card scheme does not necessarily mean that it was caused by the vaccine, only that the reporter has a suspicion it may have. Underlying or previously undiagnosed illness unrelated to vaccination can also be factors in such reports. The relative number and nature of reports should therefore not be used to compare the safety of the different vaccines. All reports are kept under continual review in order to identify possible new risks. Report Run Date: 24-Sep-2021, Page 1 Case Series Drug Analysis Print Name: COVID-19 mRNA Pfizer- BioNTech vaccine analysis print Report Run Date: 24-Sep-2021 Data Lock Date: 22-Sep-2021 18:30:09 MedDRA Version: MedDRA 24.0 Reaction Name Total Fatal Blood disorders Anaemia deficiencies Anaemia folate deficiency 1 0 Anaemia vitamin B12 deficiency 2 0 Deficiency anaemia 1 0 Iron deficiency anaemia 6 0 Anaemias NEC Anaemia 97 0 Anaemia macrocytic 1 0 Anaemia megaloblastic 1 0 Autoimmune anaemia 2 0 Blood loss anaemia 1 0 Microcytic anaemia 1 0 Anaemias haemolytic NEC Coombs negative haemolytic anaemia 1 0 Haemolytic anaemia 6 0 Anaemias haemolytic immune Autoimmune haemolytic anaemia 9 0 Anaemias haemolytic mechanical factor Microangiopathic haemolytic anaemia 1 0 Bleeding tendencies Haemorrhagic diathesis 1 0 Increased tendency to bruise 35 0 Spontaneous haematoma 2 0 Coagulation factor deficiencies Acquired haemophilia -
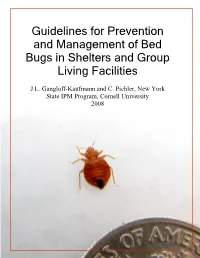
Guidelines for Prevention and Management of Bed Bugs in Shelters and Group Living Facilities
Guidelines for Prevention and Management of Bed Bugs in Shelters and Group Living Facilities J.L. Gangloff-Kaufmann and C. Pichler, New York State IPM Program, Cornell University 2008 Guidelines for Prevention and Management of Bed Bugs in Shelters and Group Living Facilities Produced for the New York City Department of Homeless Services, in cooperation with the New York City Department of Health and Mental Hygiene and the New York State Integrated Pest Management (IPM) Program, Cornell University. Written by Jody Gangloff-Kaufmann and Cathy Pichler, New York State IPM Program, Cornell University. See www.nysipm.cornell.edu . Contact Jody Gangloff-Kaufmann ([email protected]) for hard copies of this publication. Thanks to the Bed Bug Advisory Group for ideas, comments, editing, support, and interest in facing this challenge: Waheed Bajwa, NYC DOHMH; Sarah Bannister, NYC DHS; Gil Bloom, Standard Pest Management; Caroline Bragdon, NYC DOHMH; Tony Branch, NYC DHS; Stephen Clohessy, NYC HPD; David Coard, NYC DHS; Wayne Coger, NYS DHS; Richard Cooper, Cooper Pest Solutions; Sharon Heath, NYC DOHMH; Daniel Kass, NYC DOHMH; and Louis Sorkin, B.C.E., American Museum of Natural History. Thanks also, to those who generously provided photographs for this publication, including Louis Sorkin, Rick Cooper, Phil Stravino of PAC Exterminating, Lynbrook, NY, Allison Taisey, New York State IPM Program, and Black Widow Pest Control, Valley Stream, NY. This publication is supported, in part, with funding (IPM Partnership Grant 2007-008) from the Northeastern IPM Center (www.NortheastIPM.org) and the USDA Cooperative State Research, Education and Extension Service. This publication was produced by Community Integrated Pest Management Program, a part of the New York State IPM Program, which develops sustainable ways to manage pests and helps people to use methods that minimize environmental, health, and economic risks. -

Insects Affecting Man Mp21
INSECTS AFFECTING MAN MP21 COOPERATIVE EXTENSION SERVICE College of Agriculture The University of Wyoming DEPARTMENT OF PLANT SCIENCES Trade or brand names used in this publication are used only for the purpose of educational information. The information given herein is supplied with the understanding that no discrimination is intended, and no endorsement information of products by the Agricultural Research Service, Federal Extension Service, or State Cooperative Extension Service is implied. Nor does it imply approval of products to the exclusion of others which may also be suitable. Issued in furtherance of Cooperative Extension work, acts of May 8 and June 30,1914, in cooperation with the U.S. Department of Agriculture, Glen Whipple, Director, Cooperative Extension Service, University of Wyoming Laramie, WY. 82071. Persons seeking admission, employment or access to programs of the University of Wyoming shall be considered without regard to race, color, national origin, sex, age, religion, political belief, handicap, or veteran status. INSECTS AFFECTING MAN Fred A. Lawson Professor of Entomology and Everett Spackman Extension Entomologist with minor revisions by Mark A. Ferrell Extension Pesticide Coordinator (September 1996) TABLE OF CONTENTS INTRODUCTION .............................................................1 BASIC RELATIONSHIPS ......................................................1 PARASITIC RELATIONSHIPS..................................................1 Lice......................................................................1 -

Bed Bugs and Book Bags Pre-Test /Post-Test (Please Circle)
Information on knowledge gain from educational programs provided to teachers is being gathered by the University of Florida /IFAS- Extension. You will be asked to complete a short quiz both before and after an educational program about bed bugs. There are no anticipated risks to you as a participant. Upon completion of the program, you will be provided with a set of classroom curriculum, Bed Bugs and Book Bags. You are free to withdraw your consent to participate and may discontinue your participation at any time without consequence. If you have any questions about this research protocol, please contact the Jacksonville Bed Bug Task Force at 904- 255-7450. Questions or concerns about your rights as a research participant rights may be directed to the IRB02 office, University of Florida, Box 112250, Gainesville, FL 32611; (352) 392-0433. Name: _______________________________________________ Date: ________________________ School District: ________________ Grades Taught: ________________ Subjects Taught: _______________ Years of Teaching Service: _______ Ethnicity: Caucasian African American Hispanic Asian Other ___________ Bed Bugs and Book Bags Pre-Test /Post-Test (please circle) Please select the most appropriate answer choice based on your knowledge of the bed bug. If you provide this quiz to entire classes, please indicate how many individuals selected each answer choice. 1. Bed bugs have: A. Flattened bodies with leathery wings B. Yellowish hairs over oval, flattened bodies C. Jumping legs and shortened wings D. Oval bodies and eight legs 2. Bed bugs find a host through which cues? A. Blood from open sores B. Snores and body movement C. Carbon dioxide, heat and body odor D. -
Do-It-Yourself Bed Bug Control Guide
DO-IT-YOURSELF BED BUG CONTROL GUIDE DO-IT-YOURSELF BED BUG CONTROL GUIDE OVERVIEW 1 IDENTIFYING BED BUGS 2 BED BUG TOOLS Flashlight 3 Garbage bags and plastic totes 5 Mattress encasements 6 Caulk 7 Vacuum 8 Clothes dryer 9 Steamer 10 Pitfall trap 11 Desiccant insecticide dust 12 PESTICIDES 14 POST-TREATMENT EVALUATION 15 FOR MORE INFORMATION 15 Bed bug myths FALSE TRUE Bed bugs won’t come out if the While bed bugs prefer darkness, keeping the room is brightly lit. light on won’t keep these pests away. Bed bugs cannot be seen You can see all stages of bed bugs and their by the naked eye. eggs with your naked eye. Bed bugs live in dirty places. Bed bugs are not attracted to dirt and grime. However, clutter offers more hiding places. Bed bugs transmit disease. There have been no cases or studies that indicate bed bugs transmit diseases. I can get rid of bed bugs by Adult bed bugs may live as long as a year leaving my house empty for a without food, so a long vacation won’t get few weeks and letting it freeze. rid of an infestation. Allowing your house to freeze can cause severe damage to your home. OVERVIEW In recent years, there has been a nationwide resurgence of bed bug infestations, and Alaska has not been immune to this trend. Rural Alaska is especially disadvantaged because of the high cost of getting a pest management professional to a rural community. Without professional help, people tend to rely on pesticides to battle bed bugs on their own. -

Nine Clouds Beds Let Us Help You Sleep
Nine Clouds Beds Let us help you sleep “The Book” © Copyright Nine Clouds Beds, 2011. All rights reserved. Nine Clouds 2273 Dundas St. W. Mississauga, Ontario Canada L5K 2L8 www.nineclouds.ca [email protected] 1-888-BED-SALE (During business hours) Toll Free 1-888-233-7253 Table of Contents 7 Introduction 33 Chapter 6: Choosing a Bed After Injury or Need a New Mattress? Hospitalization Beds Of All Styles & Sizes Introduction Beds, Bunks, Daybeds & more... Gathering Information Equipment Requirements Care Requirements Section One: Mattress and Bed Selection Length of Rehabilitation Available Funding 11 Chapter 1: Mattress and Bed Sizes Possible Complications Twin Size Mattress Choosing a Bed Twin XL Size Mattress Adjustable Height Double Size Mattress Other Alternatives Double XL Size Mattress Choosing a Mattress Queen Size Mattress Therapeutic Aids and Other Furniture King Size Mattress Finances California King Size Mattress Custom Size Mattress International Mattress Size Chart Section Two: Sleep Quality and Your Health 15 Chapter 2: Types of Mattress Construction 43 Chapter 7: Don’t Let Bed Bugs Get the Best of Innerspring Mattresses You Coil Types Bed Bug Revival Memory Foam Mattresses Biting Behavior Latex Mattresses Is it a Bed Bug? Bye-Bye Bed Bugs 19 Chapter 3: Mattress Buying Tips Moving away Things to remember when you are buying a Don’t panic mattress. 47 Chapter 8: Bed Wetting and the Journey to 21 Chapter 4: Choosing the Right Sleeping Dry Mornings Recognized Reasons for Primary Enuresis Pillow Step One: What is your sleeping -

Addendum A: Antiparasitic Drugs Used for Animals
Addendum A: Antiparasitic Drugs Used for Animals Each product can only be used according to dosages and descriptions given on the leaflet within each package. Table A.1 Selection of drugs against protozoan diseases of dogs and cats (these compounds are not approved in all countries but are often available by import) Dosage (mg/kg Parasites Active compound body weight) Application Isospora species Toltrazuril D: 10.00 1Â per day for 4–5 d; p.o. Toxoplasma gondii Clindamycin D: 12.5 Every 12 h for 2–4 (acute infection) C: 12.5–25 weeks; o. Every 12 h for 2–4 weeks; o. Neospora Clindamycin D: 12.5 2Â per d for 4–8 sp. (systemic + Sulfadiazine/ weeks; o. infection) Trimethoprim Giardia species Fenbendazol D/C: 50.0 1Â per day for 3–5 days; o. Babesia species Imidocarb D: 3–6 Possibly repeat after 12–24 h; s.c. Leishmania species Allopurinol D: 20.0 1Â per day for months up to years; o. Hepatozoon species Imidocarb (I) D: 5.0 (I) + 5.0 (I) 2Â in intervals of + Doxycycline (D) (D) 2 weeks; s.c. plus (D) 2Â per day on 7 days; o. C cat, D dog, d day, kg kilogram, mg milligram, o. orally, s.c. subcutaneously Table A.2 Selection of drugs against nematodes of dogs and cats (unfortunately not effective against a broad spectrum of parasites) Active compounds Trade names Dosage (mg/kg body weight) Application ® Fenbendazole Panacur D: 50.0 for 3 d o. C: 50.0 for 3 d Flubendazole Flubenol® D: 22.0 for 3 d o. -

When Bed Bugs Bite
Mark K. Huntington, MD, PhD When bed bugs bite Sioux Falls Family Medicine Residency Program; Department of Family Treating bed bug bites is straightforward; helping Medicine, University of South Dakota Sanford patients control and even prevent future infestations is School of Medicine, Vermillion, SD another matter. Here’s how you can help. mark.huntington@usd. edu The author reported no ed bugs, Cimex spp, are a re-emerging public health potential conflicts of interest relevant to this article. Practice problem in the United States. First recorded by the recommenDations B ancient Greeks,1 bed bugs have plagued societies for › Provide symptomatic relief centuries. In the United States, infestations peaked in inten- for bed bug bites with antihis- sity in the 1920s and 1930s, then were largely eliminated as tamines or corticosteroids. C a significant concern after World War II, thanks to synthetic, › Advise patients experienc- residual pesticides.2 By the mid-1990s, bed bugs were so un- ing an infestation to consider common that specimens could not be obtained for medical the CDC’s recommended education purposes.3 integrated pest manage- That has all changed. ment program (eg, heat Although commonly perceived as disproportionately treatment, vacuuming, affecting the underprivileged,4 bed bugs are equal- nonchemical pesticides) to opportunity pests, infesting the most posh hotels, retailers, increase the likelihood of and theaters.5,6 According to one news report summariz- successful extermination. C ing data from a national pest control -

Children Hospitalized for Myiasis in a Reference Center in Uruguay
Boletín Médico del Hospital Infantil de México RESEARCH ARTICLE Children hospitalized for myiasis in a reference center in Uruguay Martín Notejane1,2*, Cristina Zabala1,2, Lucía Ibarra2, Leticia Sosa2, and Gustavo Giachetto1,2 1Clínicas Pediátricas, Facultad de Medicina, Universidad de la República; 2Hospital Pediátrico, Centro Hospitalario Pereira Rossell. Montevideo, Uruguay Abstract Background: Myiasis is an emerging disease caused by tissue invasion of dipteran larvae. In Uruguay, Cochliomyia homini- vorax and Dermatobia hominis are the most frequent species. This study aimed to describe the epidemiological and clinical characteristics and the follow-up of children < 15 years hospitalized for myiasis in a reference center in Uruguay between 2010 and 2019. Methods: We conducted a descriptive and retrospective study by reviewing medical records. We analyzed the following variables: age, sex, comorbidities, origin, the month at admission, clinical manifestations, other parasitoses, treatments, complications, and larva species identified. Results: We found 63 hospitalized children: median age of 7 years (1 month–14 years), 68% of females. We detected risk comorbidities for myiasis (33%), of which chronic malnutrition was the most frequent (n = 6); 84% were from the south of the country; 76% were hospitalized during the summer. Superficial and multiple cutaneous involvements were found in 86%: of the scalp 50, furunculoid type 51, secondary to C. hominivorax 98.4%, and to D. hominis in 1.6%. As treatments, larval extraction was detected in all of them, surgical in 22%. Asphyctic products for parasites were applied in 94%, ether in 49. Antimicrobials were prescribed in 95%; cephradine and ivermectin were the most frequent. About 51% presented infectious complications: impetigo was found in 29, cellulitis in 2, and abscess in 1.