NSIAD-89-119 Navy Training Chapter 1 Introduction
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Appendix File Anes 1988‐1992 Merged Senate File
Version 03 Codebook ‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐‐ CODEBOOK APPENDIX FILE ANES 1988‐1992 MERGED SENATE FILE USER NOTE: Much of his file has been converted to electronic format via OCR scanning. As a result, the user is advised that some errors in character recognition may have resulted within the text. MASTER CODES: The following master codes follow in this order: PARTY‐CANDIDATE MASTER CODE CAMPAIGN ISSUES MASTER CODES CONGRESSIONAL LEADERSHIP CODE ELECTIVE OFFICE CODE RELIGIOUS PREFERENCE MASTER CODE SENATOR NAMES CODES CAMPAIGN MANAGERS AND POLLSTERS CAMPAIGN CONTENT CODES HOUSE CANDIDATES CANDIDATE CODES >> VII. MASTER CODES ‐ Survey Variables >> VII.A. Party/Candidate ('Likes/Dislikes') ? PARTY‐CANDIDATE MASTER CODE PARTY ONLY ‐‐ PEOPLE WITHIN PARTY 0001 Johnson 0002 Kennedy, John; JFK 0003 Kennedy, Robert; RFK 0004 Kennedy, Edward; "Ted" 0005 Kennedy, NA which 0006 Truman 0007 Roosevelt; "FDR" 0008 McGovern 0009 Carter 0010 Mondale 0011 McCarthy, Eugene 0012 Humphrey 0013 Muskie 0014 Dukakis, Michael 0015 Wallace 0016 Jackson, Jesse 0017 Clinton, Bill 0031 Eisenhower; Ike 0032 Nixon 0034 Rockefeller 0035 Reagan 0036 Ford 0037 Bush 0038 Connally 0039 Kissinger 0040 McCarthy, Joseph 0041 Buchanan, Pat 0051 Other national party figures (Senators, Congressman, etc.) 0052 Local party figures (city, state, etc.) 0053 Good/Young/Experienced leaders; like whole ticket 0054 Bad/Old/Inexperienced leaders; dislike whole ticket 0055 Reference to vice‐presidential candidate ? Make 0097 Other people within party reasons Card PARTY ONLY ‐‐ PARTY CHARACTERISTICS 0101 Traditional Democratic voter: always been a Democrat; just a Democrat; never been a Republican; just couldn't vote Republican 0102 Traditional Republican voter: always been a Republican; just a Republican; never been a Democrat; just couldn't vote Democratic 0111 Positive, personal, affective terms applied to party‐‐good/nice people; patriotic; etc. -
View Full Issue As
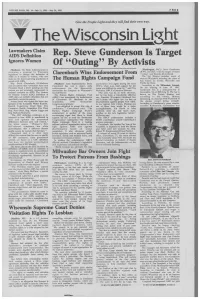
VOLUME FOUR, NO. 14—July 11, 1991—July 24, 1991 FREE Give the People Light and they will find their own way. The Wisconsin Light Lawmakers Claim AIDS Definition Rep. Steve Gunderson Is Target Ignores Women Of "Outing" By Activists [Madison]- The Bush Administration is [Washington, D.C.]- Steve Gunderson reviewing a proposal by Wisconsin (R-WI, 3rd Dist.) was the target of heavy legislators to change the definition of Clarenbach Wins Endorsement From "outing" over the July 4th weekend. AIDS as it relates to women, who now The 3rd District includes much of make up the fastest-growing population of The Human Rights Campaign Fund western Wisconsin including the cities of people with AIDS. Eau Claire, La Crosse, Platteville and Rep. David Clarenbach (D-Madison) [Madison]. State Representative David and Lesbian civil rights during the early Prairie du Chien. and seventeen other lawmakers have sent Clarenbach has won a major, early 1970's, when even mild support for the According to the Milwaukee Journal, President Bush a letter pointing out that endorsement for the Democratic cause was difficult to come by," said Tim On the evening of June 30, 1991, woman are not accurately represented in nomination for Congress in Wisconsin's McFeeley, HRCF's Executive Director. Gunderson was in a restaurant/bar in national statistics on AIDS. The Centers Second District. "Not only was he an early advocate, Alexandria, VA at 808 King St. The bar is for Disease Control (CDC) definition of The Human Rights Campaign Fund but he has been a remarkable effective known as The French Quarter and AIDS does not include infections that are (HRCF) has announced its endorsement one. -

Congressional Record—Senate S2430
S2430 CONGRESSIONAL RECORD — SENATE April 11, 2019 Two weeks ago, Senator Murray and I took California at Berkeley in 1973. Eugene over County, NC, where he practiced the first step by introducing legislation that McCarthy’s 1968 Presidential campaign for 20 years. While in private practice, will extend funding for community health inspired Jim’s exploration of politics. Judge Fox served as the county attor- centers for five years at $4 billion a year in He was elected to the Wisconsin State ney for New Hanover County for 13 mandatory funding. The legislation also extends funding for Assembly in 1976 and to the State Sen- years. four additional federal health programs set ate in 1978. With his mother at his side President Ronald Reagan nominated to expire in September: the Teaching Health as his campaign manager, he ran for Judge Fox to serve as a U.S. District Center Graduate Medical Education Pro- and was elected to the U.S. House of Court Judge for the Eastern District of gram; National Health Service Corps; Spe- Representatives in 1982 from Wiscon- North Carolina on September 13, 1982. cial Diabetes Program; and Special Diabetes sin’s 5th Congressional District in Judge Fox served the residents of Program for Indians. southeastern Wisconsin, where he North Carolina for more than 35 years. Today we will hear about how the commu- nity health centers program is working and served five terms. He served as chief judge from 1990 to how to ensure 27 million Americans can con- Moody was a progressive voice in 1997 and assumed senior status on Jan- tinue to have access to quality health care Congress in the spirit of Wisconsin’s uary 31, 2001. -
Go for It! Use Your Library
go for it! use your library national library week april 17-23, 1983 american library association LEGISLATIVE DAY IN WASHINGTON Tuesday, April 19 of National Library Week April 17-23, 1983 Sponsors: American Library Association, District of Columbia Library Association, participating state library/media associations, and other contributing organizations. SCHEDULE Morning Briefing: 8:00 to 9:00 a.m., Dirksen Senate Office Building, Room SD-106, first floor. Information folders, last minute instructions, briefing on status of library-related legislation. 8:20 a.m., briefing by Eileen D. Cooke, Director, ALA Washington Office. Because a Senate hearing is scheduled in Room SD-106 immediately followins our briefing, we must vacate the room quickly. Therefore, regrettably, coffee and doughnuts will not be served before the briefing, but can be purchased in the Dirksen Coffee Shop which opens at 7:30 a.m. Congressional Office Visits: 9:30 a.m. to 3:30 p.m., or according to your pre viously set appointments. Consult the Capitol Hill map and directory for Congressional office and telephone numbers in your folder. All Day Rest Area: Room 2105, Rayburn House Office Building, has been reserved from 8:00 a.m. to 4:00 p.m. for participant's use. Wrap-up Session: 4:00 to 5:00 p.m., Rayburn House Office Building, Room 2168 (Gold Room), first floor. Closing comments by Jack Jennings, Associate General Counsel, House Committee on Education and Labor. Any remaining time will permit informal reports and discussion of events earlier in the day. Congressional Reception: 5:00 to 7:00 p.m., Rayburn House Office BuHding, Rm. -

HOUSE of REPRESENTATIVES-Friday, July 23, 1993
16818 CONGRESSIONAL RECORD-HOUSE July 23, 1993 HOUSE OF REPRESENTATIVES-Friday, July 23, 1993 The House met at 10 a.m. Coyne Kasi ch Pomeroy Grams Livingston Ros-Lehtinen The Chaplain, Rev. James David Cramer Kennedy Porter Grandy Machtley Roth Danner Kennelly Poshard Greenwood Manzullo Roukema Ford, D.D., offered the following Darden Kildee Price (NC) Hancock McColl um Royce prayer: de la Gan.a Kleczka Ra.ball Hansen McCrery Saxton 0 gracious God, as You have blessed Deal Klein Reed Hastert Mc Dade Schaefer DeLauro Klink Reynolds Hefley McHugh Schiff Your people with the potential for dis Dellums Kopetski Richardson Herger Mcinnis Sensenbrenner cernment in all things, we pray that we Derrick Kreidler Roemer Hobson McKeon Shaw will dedicate ourselves to use our Deutsch LaFalce Rose Hoekstra McMillan Shays words in ways that promote justice and Dicks Lambert Rostenkowski Hoke Meyers Shuster Dingell Lancaster Rowland Horn Mica Skeen encourage mercy and compassion, so Durbin Lantos Roybal-Allard Huffington Michel Smith(TX) our words unite us in understanding. Edwards (TX) LaRocco Sabo Hunter Miller (FL) Smith(MI) You have called us, O God, to be faith Engel Laughlin Sangmeister Hutchinson Molinari Smith(OR) English (AZ) Lehman Sa.rpa.lius Hyde Moorhead Snowe ful in all things and we pray that we English (OK) Levin Sawyer Inbofe Morella Solomon will translate that faithfulness into the Eshoo Lewis (GA) Schenk lstook Murphy Spence words we use so they do not become Evans Lipinski Schumer Jacobs Nussle Stearns weapons of discord, but vehicles of rec Farr Lloyd Scott Johnson (CT) Oxley Stump Fazio Long SeITano Kim Paxon Sundquist onciliation and sensitivity and toler Filner Lowey Sharp King Petri Talent ance. -

Mondale Delivers in Encore Appearance
I October 25, ,984 ____V_—•___SS__M____PI_••_______________P_____B____H_HIII_>g__P*—_—__•_—••_• Mondale delivers in encore appearance by Rob Priewe Victory Hall, Cudahy. Walter Mondale. The setting was ideal; the star- "You got him" studded cast of characters, per "You got him," he responded fectly suited for their roles, play softly before endearing the crowd ed them to perfection. And when with "Just when I needed that ex the biggest star of all finally made tra oomph, I've come to Victory his appearance, he could do no Hall in Cudahy." The rejoicing wrong. had only just begun. He did no wrong, driving the blue-collar crowd into a frenzy, wiping out any notion that Walter A crowd of thousands lined up Mondale might fail in his bid for outside the tiny hall hours before the presidency. the event and when the Secret For those among the 3,500 who Security flung wide the gates, the crammed Victory Hall Wednesday people poured in, pressing as night, it could be long-remembered close to the podium as possible. as that perfect night when the Democratic challenger made a A lederhosen-clad oompah special effort to appear before band entertained against a back "his" people of Cudahy; shortly drop of banners: "Willkomen before the biggest day of his life— Fritz," "Dobro Dosli Fritz," Nov. 6. "Bienvenue Fritz," "Rainbow Mondale satisfied the enthusi- Coalition Welcomes Fritz," Democratic presidential candidate Walter Mondale delighted an over-capacity crowd Wednes "Bmvenuto Fritz," "Shalom day evening during a campaign stop at Victory Hall in Cudahy. Fritz," "In all languages.. -

§ 14. in General Carl Albert, of Oklahoma, Moved the Appeal Be Laid on the Table Parliamentary Inquiries Are in Which Motion Was Successful
Ch. 31 § 13 DESCHLER-BROWN PRECEDENTS On Oct. 8, 1968, (11) the reading THE SPEAKER: The gentleman from of the Journal was interrupted by California moves to reconsider the vote numerous points of order of no on the motion to lay the appeal from the decision of the Chair on the table, quorum. A motion was made by and the gentleman from Oklahoma Mr. Brock Adams, of Washington, moves that that motion be laid on the and adopted by the House, that table. absent Members be sent for and MR. HOSMER: Mr. Speaker, I make a thereafter detained until the dis- point of order against the motion of the position of the pending business of gentleman from Oklahoma to lay my the day. This motion provoked motion on the table because that mo- some Members to express concern tion does not lie. THE SPEAKER: The Chair will state about their personal liberty and that a motion to lay on the table, on a rights. In this context, Mr. Robert motion to reconsider, is a recognized Taft, Jr., of Ohio, attempted to in- motion. terrupt the reading of the Journal The question is on the motion to lay with what he contended was a on the table. question of privilege, but which MR. HOSMER: Mr. Speaker, on that I Speaker John W. McCormack, of demand the yeas and nays. Massachusetts, determined not to The yeas and nays were ordered. properly raise a question of privi- . lege of the House in the form and So the motion to lay on the table was agreed to. -

SA Candidates Meet for Last Time in Dorm Debate
<;?:-:-:;' Tuesday, April 8, 1986 The University of Wisconsin-Milwaukee Volume 30, Number 50 SA candidates meet for last time in dorm debate UPB votes to went on to name conflicts between nations cutbacks in education and increase services toy Doug Hissbm presently going on in the world, while his to students,'' she said. allow carry-out running mate Richard Schulte flicked toy Parris Brady, the Green vice presidential he four executive slates in the Student army soldiers off the debate table and into candidate, also gave a list of cuts. beer, wine sale Association election race squared off the audience. "There will be tuition increases. There will Tfor the last time Thursday in a debate Wearing a black executioner-type hood, also be effects in the cuts on campus," he in Sandburg at Sandburg Halls. Schulte then quoted from the Bible book said. "The only thing we can do about this is The elections will be held April 8 and 9. Revelation, while Novy smashed a model get students involved.'' he executive committee of The forum, which drew about nine airplane with a gavel. Mike Price, vice presidential candidate the Union Policy Board spectators, featured the candidates corn- "The time has come to destroy those who from the Slumber Party, touted the party's Tvoted to accept a Sandburg full slate of senate candidates. Commons Policy Board recom mendation Thursday authorizing ' 'Right now all of the people out there have the sale of beer and wine coolers the opportunity to bring student government at the Sandburg Emporium. The out of the darkness it's been in the past motion passed with 7 votes and years," he said. -

H. Doc. 108-222
NINETY-EIGHTH CONGRESS JANUARY 3, 1983, TO JANUARY 3, 1985 FIRST SESSION—January 3, 1983, to November 18, 1983 SECOND SESSION—January 23, 1984, 1 to October 12, 1984 VICE PRESIDENT OF THE UNITED STATES—GEORGE H. W. BUSH, of Texas PRESIDENT PRO TEMPORE OF THE SENATE—J. STROM THURMOND, of South Carolina SECRETARY OF THE SENATE—WILLIAM F. HILDENBRAND, of the District of Columbia SERGEANT AT ARMS OF THE SENATE—HOWARD S. LIEBENGOOD, of Virginia; LARRY E. SMITH, 2 of Virginia SPEAKER OF THE HOUSE OF REPRESENTATIVES—THOMAS P. O’NEILL, JR., 3 of Massachusetts CLERK OF THE HOUSE—BENJAMIN J. GUTHRIE, 3 of Virginia SERGEANT AT ARMS OF THE HOUSE—JACK RUSS, 3 of Maryland DOORKEEPER OF THE HOUSE—JAMES T. MOLLOY, 3 of New York POSTMASTER OF THE HOUSE—ROBERT V. ROTA, 3 of Pennsylvania ALABAMA Eldon D. Rudd, Scottsdale Tom Lantos, San Mateo SENATORS James F. McNulty, Jr., Bisbee Edwin V. W. Zschau, Los Altos Norman Y. Mineta, San Jose Howell T. Heflin, Tuscumbia ARKANSAS Norman D. Shumway, Stockton Jeremiah Denton, Mobile SENATORS Tony Coelho, Merced REPRESENTATIVES Dale Bumpers, Charleston Leon E. Panetta, Carmel Valley Jack Edwards, Mobile David H. Pryor, Camden Charles Pashayan, Jr., Fresno William L. Dickinson, Montgomery Richard H. Lehman, Sanger Bill Nichols, Sylacauga REPRESENTATIVES Robert J. Lagomarsino, Ventura Tom Bevill, Jasper Bill Alexander, Osceola William M. Thomas, Bakersfield Ronnie G. Flippo, Florence Ed Bethune, Searcy Bobbi Fiedler, Northridge Ben Erdreich, Birmingham John P. Hammerschmidt, Harrison Carlos J. Moorhead, Glendale Richard C. Shelby, Tuscaloosa Beryl F. Anthony, Jr., El Dorado Anthony C. Beilenson, Los Angeles Henry A. -

One Hundred Second Congress January 3, 1991 to January 3, 1993
ONE HUNDRED SECOND CONGRESS JANUARY 3, 1991 TO JANUARY 3, 1993 FIRST SESSION—January 3, 1991, to January 3, 1992 SECOND SESSION—January 3, 1992, to October 9, 1992 VICE PRESIDENT OF THE UNITED STATES—J. DANFORTH QUAYLE, of Indiana PRESIDENT PRO TEMPORE OF THE SENATE—ROBERT C. BYRD, of West Virginia SECRETARY OF THE SENATE—WALTER J. STEWART, of Washington, D.C. SERGEANT AT ARMS OF THE SENATE—MARTHA S. POPE, 1 of Connecticut SPEAKER OF THE HOUSE OF REPRESENTATIVES—THOMAS S. FOLEY, 2 of Washington CLERK OF THE HOUSE—DONNALD K. ANDERSON, 2 of California SERGEANT AT ARMS OF THE HOUSE—JACK RUSS, 3 of Maryland; WERNER W. BRANDT, 4 of New York DOORKEEPER OF THE HOUSE—JAMES T. MALLOY, 2 of New York POSTMASTER OF THE HOUSE—ROBERT V. ROTA, 2 of Pennsylvania DIRECTOR OF NON-LEGISLATIVE AND FINANCIAL SERVICES 5—LEONARD P. WISHART III, 6 of New Jersey ALABAMA John S. McCain III, Phoenix Pete Wilson, 9 San Diego 10 SENATORS REPRESENTATIVES John Seymour, Anaheim Dianne Feinstein, 11 San Francisco Howell T. Heflin, Tescumbia John J. Rhodes III, Mesa Richard C. Shelby, Tuscaloosa Morris K. Udall, 7 Tucson REPRESENTATIVES REPRESENTATIVES Ed Pastor, 8 Phoenix Frank Riggs, Santa Rosa Wally Herger, Rio Oso Sonny Callahan, Mobile Bob Stump, Tolleson William L. Dickinson, Montgomery Jon Kyl, Phoenix Robert T. Matsui, Sacramento Glen Browder, Jacksonville Jim Kolbe, Tucson Vic Fazio, West Sacramento Tom Bevill, Jasper Nancy Pelosi, San Francisco Bud Cramer, Huntsville ARKANSAS Barbara Boxer, Greenbrae George Miller, Martinez Ben Erdreich, Birmingham SENATORS Claude Harris, Tuscaloosa Ronald V. Dellums, Oakland Dale Bumpers, Charleston Fortney Pete Stark, Oakland ALASKA David H. -

EXTENSIONS of REMARKS March 7, 1990 EXTENSIONS of REMARKS
3806 EXTENSIONS OF REMARKS March 7, 1990 EXTENSIONS OF REMARKS LEGISLATION TO CONTROL THE water supplies and fish populations gets barrel and fresh bread was available only on INFESTATION OF THE WATERS worse. the weekends. OF THE UNITED STATES BY Congressman NOWAK's "Nonindigenous Over the years, of course, modern conven THE ZEBRA MUSSEL Aquatic Nuisance Act of 1990" looks toward iences such as prepackaged goods and proc solving this problem for the Great Lakes as essed foods were incorporated into the HON. ROBERT W. DAVIS well as other infested U.S. waters. Mr. NOWAK stores' inventories, but it was the personal OF MICHIGAN mandates Coast Guard regulations directing service and the heartfelt caring for their neigh IN THE HOUSE OF REPRESENTATIVES mid-ocean ballast water exchange or other bors that kept people coming back to Click's measures to control infestation of U.S. waters Wednesday, March 7, 1990 Store. with unwelcome visitors. Violations of these I want to extend to the entire Click family Mr. DAVIS. Mr. Speaker, today I join my col requirements will result in a $25,000 penalty. my sincere hope for a happy and healthy re league, Congressman NOWAK of New York, in In addition, this bill establishes groups to co tirement. I would also like to request that the the introduction of legislation that will lead to ordinate research on aquatic nuisance spe attached newspaper article be inserted in the control the infestation of the waters of the cies, including a Great Lakes Regional Com United States by the zebra mussel. RECORD as a tribute to a family that serves as mission. -

Llint'tij-Jlmu Urns
A P R IL , 1967 llint’tij-Jlmu U rn s z f k c_Afmety-c_Afmeg ^ C o umn Spring has sprung! And with the new bership wants unless you COMMUNI 'w growth of Spring, there also comes a CATE. Perhaps you have an idea on renewed desire to improve . up fund raising that no one else has grade . do something constructive. thought about . tell it! Or you Everything seems to take a ‘new have an idea on how to interest your lease on life’ about this time of year community airport on sponsoring a APRIL, 1967 and it should be no different with the race stop . tell it! Or you know Ninety Nines. a group of women who would like to This is the month of Spring Section become Ninety Nines but aren’t sure THE NINETY-NINES, Inc. meetings . so be sure you plan of the proceedures . tell them! It International Headquarters to attend yours. It is too late for you is only through letting our wants and Will Rogers World Airport to send that nomination, resolution, wishes be made known, that we get Oklahoma City, Oklahoma 73159 or application for the AE Scholarship, them accomplished. Headquarters Secretary but it is not too late for you to make MARY VIAL, Phoenix Chairman, DARLA BULLARD your contributions to the AE Fund and I had such a delightful time with or the AWTAR. Wouldn’t it be wonder LADY McREYNOLDS, Tennessee ful if each chapter would send in their Chairman, during her visit in Phoenix. Editor contributions NOW and when the re We had lunch together around the pool PEG ONG ports are read at convention, we would and talked about (of all things) fly 2900 Rockbrook Drive have the TOTAL amounts given and ing! LADY told us what a wonderful Plano, Texas 75074 EVERY CHAPTER contributing? Job EVELYN BRYAN JOHNSON is This is also the month your Execu doing on the Morristown Airport.