Implementing a Public Private Partnership Model for Managing Urban Health in Ahmedabad
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Hon'ble PM Speech
Transcription of Hon’ble Prime Minister Shri Narendra Modi’s speech on the inauguration of Gandhinagar Railway Station Shri Narendra Modi Prime Minister of India My colleagues in the Council of Ministers, the Parliamentarians of Gandhinagar, Shri Amit Shah Ji, Railway Minister Ashwini Vaishnaw Ji, Gujarat Chief Minister Rupani Ji, Deputy Minister Nitin Bhai, Union Minister, Smt. Darshana Jardosh, other ministers in the Government of Gujarat, my colleagues in the Parliament, President of Bhartiya Janata Party, Gujarat, Shri C.R. Patil Ji, other members of Parliament, MLAs and my dear brothers and sisters, Greetings to all of you. I hope all is well. Today is the day of 21st century India's aspirations, a prominent symbol of Indian youth's feelings and possibilities, be it science and technology, better urban landscape. The modern infrastructure exemplifying connectivity is adding another chapter to the new identity of New India. I have inaugurated all the projects from Delhi here, but I am eager to come and see them myself. Brothers and sisters, today, the goal of the country is not only to build concrete structures but today, the infrastructure of such scale is being constructed in the country, which has a character of its own. Better public space is our need. It has reimagined urban planning like never thought before. In the urban planning of the past, it (better public space) was perceived as a luxury. The real estate and housing companies focus on park-facing houses, as most of the population has been deprived of quality public space and quality public life. -
Shri Amit Shah
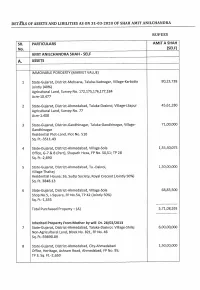
DETAILS OF ASSETS AND LIBILITIES AS ON 31-03-2020 OF SHAH AMIT ANILCHANDRA RUPEES SR. PARTICULARS AMIT A SHAH No. (SELF) AMIT ANILCHANDRA SHAH - SELF A. ASSETS IMMOVABLE POROERTY (MARKET VALUE) 1 State-Gujarat, District-Mehsana, Taluka-Vadnagar, Village-Karbatia 80,23,738 Jointly (40%) Agricultural Land, Survey No. 172,175,176,177,184 Acre-10.477 2 State-Gujarat, District-Ahmedabad, Taluka-Daskroi, Village-Lilapur 45,61,280 Agricultural Land, Survey No. 77 Acre-1.408 3 State-Gujarat, District-Gandhinagar, Taluka-Gandhinagar, Village- 71,00,000 Gandhinagar Residential Plot-Land, Plot No. 510 Sq. Ft.-3511.43 4 State-Gujarat, District-Ahmedabad, Village-Sola 1,55,40,075 Office, G-7 & 8 (Part), Shapath Hexa, FP No. 50,51; TP 28 Sq. Ft.-2,690 5 State-Gujarat, District-Ahmedabad, Ta.-Dakroi, 1,50,00,000 Village-Thaltej Residential House; 16, Sudip Society, Royal Crecent (Jointly 50%) Sq. Ft. 3848.13 6 State-Gujarat, District-Ahmedabad, Village-Sofa 68,83,500 Shop No.5, I-Square, FP No.54, TP 42 (Jointly 50%) Sq. Ft.-1,355 Total Purchased Property — (A) 5,71,08,593 Inherited Property From Mother by will Dt. 28/02/2013 7 State-Gujarat, District-Ahmedabad, Taluka-Daskroi, Village-Shilaj 6,00,00,000 Non-Agricultural Land, Block No. 821, FP No. 48 Sq. Ft.-59890.89 8 State-Gujarat, District-Ahmedabad, City-Ahmedabad 1,50,00,000 Office, Heritage, Ashram Road, Ahmedabad, FP No. 95; TP 3, Sq. Ft.-2,650 State-Gujarat, District-Ahmedabad, Village-Memnagar 15,00,000 Office, A-01, Surya Complex, Gurukul Road, Memnagar, Ahmedabad Sq. -

President Shri Ram Nath Kovind Performed Bhoomi Pujan (Ground
Ministry of Home Affairs President Shri Ram Nath Kovind performed Bhoomi Pujan (ground breaking ceremony) of a huge sports enclave in Ahmedabad, Gujarat named after Bharat Ratna and brave son of Gujarat, Sardar Vallabhbhai Patel िवि ितिथ: 24 FEB 2021 10:11PM by PIB Delhi Respected President also inaugurated the world's largest sports stadium, 'Narendra Modi Cricket Stadium', this largest cricket stadium in the world is part of the Sardar Vallabhbhai Patel sports complex Union Home Minister Shri Amit Shah also present on the occasion Shri Amit Shah said today is a golden day in India's sports history 1.32 lakh spectators will be able to enjoy the match in the stadium, the stadium has 11 pitches, unrivalled by any stadium in the world Union Home Minister said 'Sardar Vallabh Bhai Sports Enclave' is an ambitious project It will be the largest sports enclave in the country to be built on 233 acres of land and will have world class sports facilities Dream project of Prime Minister Shri Narendra Modi when he was Chief Minister of Gujarat, has been fulfilled today Ahmedabad will be known as Sports City of India More than 600 schools in Gandhinagar and Ahmedabad rural district will be connected to the sports enclave and children of schools that do not have their own playgrounds will be able to avail of sports facilities Accommodation for 250 coaches and 3,000 children will be available to make them able to train together By setting up Sardar Vallabhbhai Patel Sports Enclave, Shri Modi has expressed special reverence for Sardar Patel Sardar -

Motera Stadium Named After Modi Conceptualised by PM When He Was Gujarat CM: President Kovind
Motera stadium named after Modi Conceptualised by PM when he was Gujarat CM: President Kovind Mahesh Langa AHMEDABAD The world’s largest cricket arena at Motera in Ahmeda- bad, the Sardar Patel Cricket Stadium, was renamed Na- rendra Modi Stadium and was inaugurated on Wednes- day by President Ram Nath Kovind in the presence of Un- ion Home Minister Amit Shah, his son Jay Shah, who is BCCI Secretary, and others. The rebuilt stadium is part of the proposed Sardar Val- labhbhai Patel Sports En- At the launch: President Ram Nath Kovind and Union Home Minister Amit Shah during the clave to be spread over 220 Bhumi Pujan of the Sardar Vallabhbhai Patel Sports Enclave. * PTI acres on the Sabarmati river bank in the North East of Ah- complex will also be built in in 2016 and has been com- ter Narendra Modi when he medabad. The foundation Naranpura,” Home Minister pleted at the estimated cost was Chief Minister of Gujarat. stone for the Enclave was al- Amit Shah announced in his of ₹800 crore. He was president of the Guja- so laid on Wednesday by the speech. “These three will be The refurbished venue is rat Cricket Association at that President. It will comprise a ready to host any interna- spread over 63 acres and has time," President Ram Nath natatorium, athletics track, tional sports event.” a seating capacity of 1.1 lakh, Kovind said during his inaug- football, hockey and tennis The initiative at Motera more than double the pre- ural address. stadia, velodrome/skating was the dream project of vious number of 49,000. -

Pib.Gov.In “5” (Home-MHA)
pib.gov.in “5” (Home-MHA) Press Information Bureau Government of India ***** Union Home Minister Shri Amit Shah visited the newly constructed Dhanvantari Covid Hospital in Ahmedabad Shri Amit Shah reviewed the healthcare facilities available in the hospital This hospital, starting services tomorrow, was set up in a short span of 10 days This Covid Hospital, located at the Gujarat University Convention and Exhibition Center in Ahmedabad, has been set up by the Government of Gujarat in collaboration with the Defence Research and Development Organization (DRDO), Union Home Ministry and Ministry of Defence This hospital, with a capacity of more than 900 beds, has all necessary facilities including intensive and critical care for Covid patients All beds are equipped with oxygen, 150 of these beds will be ICU beds with ventilators More than 200 medical and paramedical staff including 50 doctors and Duty Medical Officers will be deployed in the hospital The Union Home Minister also held a meeting with the Chief Minister of Gujarat, Shri Vijay Rupani, Deputy CM Shri Nitinbhai Patel and senior state officials to review the Covid situation in Gujarat Shri Amit Shah will also provide healthcare facilities worth Rs 10 crore for Covid patients in government hospitals of his parliamentary constituency Gandhinagar today These facilities, provided on a war footing, include 100 Bipap machines as oxygen Concentrators, including 50-50 machines and 25 ventilators for Gandhinagar Civil Hospital and Sola Civil Hospital Also provided 6 ambulances, 2 ICU on wheels and 2 mobile testing laboratory, this facility will be made available exclusively to the rural population of 160 villages of Ahmedabad district and 100 villages of Gandhinagar district and 4 for municipalities New Delhi: 23.04.2021 The Union Home Minister Shri Amit Shah visited the newly constructed Dhanvantari Covid Hospital in Ahmedabad today. -

'5' Press Information Bureau Government of India
‘5’ www.pib.nic.in Press Information Bureau Government of India *** Shri Amit Shah assumes charge as Union Home Minister Shri G. Kishan Reddy and Shri Nityanand Rai also took charge as MoS (Home) New Delhi, June 1, 2019 Shri Amit Shah, Union Minister of Home Affairs, assumed charge of his office here today. He was greeted by Union Home Secretary Shri Rajiv Gauba and Director, Intelligence Bureau Shri Rajiv Jain upon arrival at the North Block. Shri Amit Shah was also felicitated by new Ministers of State (Home), Shri G. Kishan Reddy and Shri Nityanand Rai who also took charge of office today. Shri Amit Shah was recently elected to the 17th Lok Sabha from Gandhinagar constituency. He has been a Rajya Sabha member, Minister in Gujarat Government and MLA in the Gujarat Legislative Assembly. Professionally he pursued Agriculture and has been a Political and Social Worker. Born to Smt. Kusumben and Shri Anilchandra Shah, an affluent Gujarati family, in the year 1964 in Mumbai, Shri Amit Shah lived and studied in his paternal village Maansa, Gujarat until the age of 16, when upon completion of his school education, his family shifted to Ahmedabad. He acquired his B.Sc. (Second Year) degree from Gujarat University, Ahmedabad. Shri Amit Shah has been a member of the Gujarat Legislative Assembly from 1997 to 2017 and he served as a Minister in the Government of Gujarat from 2002 to 2010, and held key portfolios including Home, Transport, Prohibition, Parliamentary Affairs, Law, and Excise. In August, 2017 he was elected to the Rajya Sabha, and ceased to be a Member w.e.f. -

Jagan to Pick Mayors, Deputies
Follow us on: @TheDailyPioneer facebook.com/dailypioneer RNI No. TELENG/2018/76469 Established 1864 SPORTS 11 Published From ANALYSIS 7 MONEY 8 HYDERABAD DELHI LUCKNOW WHO IS RESPONSIBLE FOR ASTRAZENECA REASSURES SAFETY OF KOHLI & CO EYE SERIES BHOPAL RAIPUR CHANDIGARH THE HIGH FUEL PRICES? COVID VAX; SAYS NO EVIDENCE OF RISKS LEAD BHUBANESWAR RANCHI DEHRADUN VIJAYAWADA *LATE CITY VOL. 3 ISSUE 123 VIJAYAWADA, TUESDAY MARCH 16, 2021; PAGES 12 `3 *Air Surcharge Extra if Applicable ANAND ANNOUNCES TWO NEW FILMS { Page 12 } www.dailypioneer.com YOUTUBER LILLY SINGH'S PRO-FARMER NCB MOVES SUPREME COURT AGAINST THE 7-LETTER WORD GOT TWITTER IM TERRORIST ARIZ GETS DEATH PENALTY MESSAGE AT THE GRAMMYS RED CARPET HC ORDER GRANTING RHEA BAIL USERS BANNED FOR NO REASON IN BATLA HOUSE ENCOUNTER CASE ouTuber and content creator Lilly Singh he Narcotics Control Bureau has moved witter users who used the word Delhi court Monday awarded death penal- made a statement at the Grammy the Supreme Court challenging the Bo- "Memphis" found themselves ty to Ariz Khan for the murder of deco- YAward ceremony by wearing mask Tmbay High Court order granting bail Ttemporarily locked out of their Arated Delhi Police Inspector Mohan that showed her support for the farmer' to actress Rhea Chakraborty, arrested accounts at the weekend because of a Chand Sharma in connection with the protest in India. Ms Singh, who has been over drugs-related charges in actor bizarre bug. Several users shared sensational 2008 Batla House encounter vocal about her support for the Sushant Singh Rajput's death case. A screenshots showing messages from case, saying the offence fell under the protesting farmers, posed in a mask with bench of Chief Justice Bobde and Twitter saying their account was being "rarest of the rare category" warranting a message: "I stand with farmers". -

Kopran Ltd Unpaid Dividend 2020-21 Interim NAME ADD1 ADD2 ADD3 CITY PIN AMOUNT A
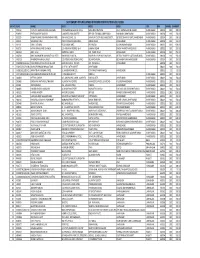
Kopran Ltd Unpaid dividend 2020-21 Interim NAME ADD1 ADD2 ADD3 CITY PIN AMOUNT A . PADMANABHAN NO.24/16 VEDACHALA GARDEN MANDAVELI CHENNAI 600028 2700.00 A KUMAR 24 1 1 ALIPORE ROAD FLAT 12 CALCUTTA 700027 1500.00 A MUTHIAH 496 KK NAGAR MADURAI 625020 9.00 A N NAGARAJAIAH C/O DHONDUSA EXPORT HOUSE 273 S C ROAD BANGALORE 560009 150.00 A NAGAVENI 8-82 TEMPLE ALWAL HYDERABAD 500010 798.00 A S G PAVOON THILAGAM OLD NO 133/2G NEW NO 452 KAMARAJAR ROAD VIRUDHUNAGAR TAMILNADU 626123 450.00 A SADIGBASHA 9/1/124 WARD 8/9 INDHRA NAGAR VEERAKKALPUTHUR SP SALEM 636403 1.50 A SUNDARARAJAN NO 238 MELATHERU KAKKARAI PO ORATHANADU THANJAVUR 614625 225.00 A T FRANCIS XAVIER AMBALAMKANDAM HOUSE, THOTTAKOM P O VAIKOM, KOTTAYAM DIST KERELA 686145 225.00 A. ABDUL SUBHAN 13/B C V MOSES STREET PAMMAL CHENNAI 600075 150.00 A. RAMREDDY H NO 6-1-118/3, PADMARAO NAGAR, SECUNDARABAD 500025 225.00 A.K.SRIVASTAVA KOPRAN LIMITED, VILLAGE-SAVROLI, RAIGAD(DIST) 410202 150.00 A.K.SRIWASTAVA KOPRAN LTD., VILLAGE SAVROLI, RAIGAD(DIST) 410202 225.00 A.MAKIN 23/25 BUXI BAZAR ALLAHABAD 211003 150.00 A.P SUBRAMANIAN 14 MULUND POONAM CO OP HSG SOCIETY IIDR FL R.P ROAD B/H MUNCIPAL HOSPITAL MULUND MUMBAI 400080 150.00 A.S.KUMAR B-144A, SECTOR-26, GHAZIABAD(DIST) 201301 225.00 AABHA JANGRA HOUSE NUMBER-1 GOVT POLYTECHNIC BOYS SIRSA NEAR GOVT POLYTECHNIC SCHOOL SIRSA 125055 300.00 AASHISH VYAS 5, PRAGATI, 60, J K MEHTA ROAD, SANTACRUZ(W) BOMBAY 400054 75.00 AASHITA ASHWINKUMAR PATEL 23-NANDANVAN SOC B/H RAILWAY STATON VADODARA 390005 300.00 AASIF U SURTI C/O HANI INDUSTRIES LTD 211-212 SAMPANNANAVARANGPURA AHMEDABAD 380009 75.00 ABBAS FAKHRUDDIN FURNITUREWALA PO BOX 6218 C/O ELEMENT MIDDLE EAST DUBAI DUBAI UAE 237.00 ABDUL MUJEER KHAN 22/109,NEAR HALL TALIM MASQUE POTTERS STREET A.P. -
Unclaimed Dividend for 2017-2018
STATEMENT OF UNCLAIMED DIVIDEND FOR THE YEAR 2017‐2018 SR. NO FLNO NAME1 ADD1 ADD2 ADD3 CITY PIN SHARES AMOUNT 1 P00132 PURSHOTTAMBHAI GOKALDAS PATEL C/O ISWARBHAI LALBHAI PATEL NAVA MADHAVPURA DELHI DARWAJAAHMEDABAD AHMEDABAD 380004 200 300.00 2 P00494 PRITI KAMLESH SANGHVI 9, NAMRTA PARK SOCIETY OPP.OLD TOLNAKA CAMP ROAD SHAHIBAUGAHMEDABAD AHMEDABAD 380004 100 150.00 3 S02299 SANJAYKUMAR DASHARATHBHAI PATEL OM NIVAS, B.NO. 24, SHAHPUR CO‐OP HOUSING SOCIETY, OUTSIDE SHAHPUR GATE,AHMEDABAD AHMEDABAD 380004 200 300.00 4 S00201 SOHANRAJ SHAH 704/8 CHINUBHAI BUILDING., SAKAR BAZAR AHMEDABAD AHMEDABAD 380002 100 150.00 5 S01102 SUNIL LUTHARIA 95/4,JUMANI MKT, REVI BAZAR KALUPURAHMEDABAD AHMEDABAD 380002 400 600.00 6 R00715 RATAN TARACHAND CHAWLA C/O ARDHANA TEXTILE 46‐A JUMANI BAZAR SINDHI MARKETAHMEDABAD AHMEDABAD 380002 100 150.00 7 A00694 AMIT SHAH AMP INVESTMENT 505‐ PANCHKUVA AHMEDABAD AHMEDABAD 380002 500 750.00 8 M00201 MRS. MADHUBEN DASHARATHLAL PATEL "OM NIVAS" B NO.24., SHAHPUR CO‐OP HOUSING SOCY., OUTSIDE SHAHPUR GATEAHMEDABAD AHMEDABAD 380004 100 150.00 9 M01430 MAHENDRA MANILAL VASA C/O.PREMCHAND TORACHAND, OLD MADHPURA, OLD MADHPURA,AHMEDABAD AHMEDABAD 380004 100 150.00 10 IN30098210313361 PRAVINSING ACHALSING CHAUHAN BAVA NU DEHLU ‐ NO.276 O/S. PREM GATE AHMEDABAD 380002 100 150.00 11 IN30154914223280 MAHADEV PRASAD BHAGATRAM 42 NEW CLOTH MARKET AHMEDABAD 380002 100 150.00 12 IN30226911052413 AMRATBHAI BABABHAI PATEL 36, HARIDARSHAN SOC, CTM 4 RASTA AMRAIWADI, AHMEDABAD 380001 15 22.50 13 1207100000114863 GANESHBHAI KHANABHAI CHAUHAN 4, UPASANA SOCIETY, SARKHEJ, . AHMEDABAD 380001 100 150.00 14 D00603 DEEPAK GANDHI 102, ANURADHA COMM. -

Profile of GCA President: Shri Amit Shah
Profile of GCA President: Shri Amit Shah A man known for proven organisational abilities and strategic planning, Amit Shah is a politician of the hinterland with a distinguished political record and commitment for the ideals he stands for. He is a man of commitment and determination in whatever he does. Born on October 22, 1964, Shah has not inherited either public administration or politics. Instead, he drew inspiration from philanthropist family and entered into the public life to serve the society. Sports Administration: Shri Amit Shah got elected as vice president of the Gujarat Cricket Association (GCA) in 2009, while the then chief minister of Gujarat and now Prime Minister of India Shri Narendra Modi was president of GCA. The duo, with their organizational skills and visionary outlook started revamping the CGA administration. Soon, the results were seen not only on the storyboard of the organization but also in the performance of the cricketers on the ground. Shri Amit Shah took over as President, GCA in 2014 as Shri Narendra Modi moved to Delhi to lead the nation as the Prime minister. Shri Amit Shah too became the national president of BJP but took upon his shoulders the responsibility to realize dream of Shri Narendra Modi to make Motera the world's largest stadium. With ground-breaking done, the site is humming up with all round construction activities. In the meantime, GCA team has won all three formats – T-20, 50 Overs and First Class cricket trophies. Till the time, Shri Amit Shah got associated with GCA, only handful of cricketers of Gujarat had got opportunity to show their skills. -

Shri Amit Shah
UNION HOME MINISTER Shri Amit Shah Shri Amit Shah Shri Amit Shah Amit Shah was born to Smt. Kusumben and Shri Anilchandra Shah, in an affluent Gujarati family on 22nd October 1964. Amit Shah represents the emerging New India in every sense of the term. Leading the Party from the front for the last five years, he has been remarkably successful in expanding BJP’s organisational foot print, securing one electoral victory after the other in State assembly elections. During his tenure, Party has become the world’s largest political party with over 10 crore registered members. Amit Shah has risen to Head the ruling Party of India literally from the grass roots. Initially, he joined the Rashtriya Swayamsevak Sangh and later became an active member of the Akhil Bharatiya Vidyarthi Parishad (ABVP), to become its Ahmedabad city unit secretary. Later, he also shouldered the responsibilities of Secretary as well as Vice President of BJP,Gujarat State. In 1997, he became National Treasurer of the Bharatiya Janata Yuva Morcha (BJYM).His dedication, dexterity and above all result oriented performance made him In-Charge of several election campaigns of the National Leaders including that of L K Advani in 1991, Atal Bihari Vajpayee in 1996, both in Gandhi Nagar Parliamentary constituency. No wonder, when Shri Narendra Modi had decided to contest his first Assembly Election in 2001 from Rajkot-2 assembly constituency, Amit Shah was again theCampaign Chief Beyond campaigns, Amit Shah also became known for his adroit handling of organisational matters. In 2013, he was appointed as National General Secretary of the BJP and In-Charge of Uttar Pradesh. -

Amit Shah - Minister of Home Affairs
AMIT SHAH - MINISTER OF HOME AFFAIRS DETAILS OF ASSETS AND LIBILITIES AS ON 31-03-2019 RUPEES SR. PARTICULARS AMIT A SHAH No (SELF) AMIT ANILCHANDRA SHAH - SELF A. ASSETS I IMMOVABLE PROPERTY (MARKET VALUE) 1 State-Gujarat, District-Mehsana, Taluka-Vadnagar, Village- 80,23,738 Karbatia(Jointly - 40%) Agricultural Land, Survey No. 172,175,176,177,184 Acre-10.477 2 State-Gujarat, District-Ahmedabad, Taluka-Daskroi, Village- 45,61,280 Lilapur Agricultural Land, Survey No. 77 Acre-1.408 3 State-Gujarat, District-Gandhinagar, Taluka-Gandhinagar, 71,00,000 Village-Gandhinagar Residential Plot-Land, Plot No. 510 Sq. Ft.-3511.43 4 State-Gujarat, District-Ahmedabad, Village-Sola 1,55,40,075 Office, G-7 & 8 (Part), ShapathHexa, FP No. 50,51; TP 28 Sq. Ft.-2,690 5 State-Gujarat, District-Ahmedabad, Ta.-Dakroi, 1,50,00,000 Village-Thaltej Residential House; 16, Sudip Society, Royal Crecent (Jointly 50%) Sq. Ft. 3848.13 5,02,25,093 Total Purchased Property — (A1) 6 Inherited Property from Mother by will Dt. 28/02/2013 6,00,00,000 State-Gujarat, District-Ahmedabad, Taluka-Daskroi, Village- Shilaj Non-Agricultural Land, Block No. 821, FP No. 48 Sq. Ft.-59890.89 7 State-Gujarat, District-Ahmedabad, City-Ahmedabad 1,50,00,000 Office, Heritage, Ashram Road, Ahmedabad, FP No. 95; TP 3, Sq. Ft.-2,650 8 State-Gujarat, District-Ahmedabad, City-Ahmedabad, Village- 15,00,000 Memnagar, Office, A-01, Surya Complex, Gurukul Road, Memnagar, AhmedabadSq. Ft.-293 9 State-Gujarat, District-Gandhinagar, Ta.-Mansa, Village-Mansa 20,00,000 Residential House, (Survey No.