Fibrotic Lung Diagnosis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Occupational Airborne Particulates
Environmental Burden of Disease Series, No. 7 Occupational airborne particulates Assessing the environmental burden of disease at national and local levels Tim Driscoll Kyle Steenland Deborah Imel Nelson James Leigh Series Editors Annette Prüss-Üstün, Diarmid Campbell-Lendrum, Carlos Corvalán, Alistair Woodward World Health Organization Protection of the Human Environment Geneva 2004 WHO Library Cataloguing-in-Publication Data Occupational airborne particulates : assessing the environmental burden of disease at national and local levels / Tim Driscoll … [et al.]. (Environmental burden of disease series / series editors: Annette Prüss-Ustun ... [et al.] ; no. 7) 1.Dust - adverse effects 2.Occupational exposure 3.Asthma - chemically induced 4.Pulmonary disease, Chronic obstructive - chemically induced 5.Pneumoconiosis - etiology 6.Cost of illness 7.Epidemiologic studies 8.Risk assessment - methods 9.Manuals I.Driscoll, Tim. II.Prüss-Üstün, Annette. III.Series. ISBN 92 4 159186 2 (NLM classification: WA 450) ISSN 1728-1652 Suggested Citation Tim Driscoll, et al. Occupational airborne particulates: assessing the environmental burden of disease at national and local levels. Geneva, World Health Organization, 2004. (Environmental Burden of Disease Series, No. 7). © World Health Organization 2004 All rights reserved. Publications of the World Health Organization can be obtained from Marketing and Dissemination, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel: +41 22 791 2476; fax: +41 22 791 4857; email: [email protected]). -

Bronchiolitis After Lung Transplantation Lymphoid Tissue In
The Role of Intrapulmonary De Novo Lymphoid Tissue in Obliterative Bronchiolitis after Lung Transplantation This information is current as Masaaki Sato, Shin Hirayama, David M. Hwang, Humberto of September 25, 2021. Lara-Guerra, Dirk Wagnetz, Thomas K. Waddell, Mingyao Liu and Shaf Keshavjee J Immunol 2009; 182:7307-7316; ; doi: 10.4049/jimmunol.0803606 http://www.jimmunol.org/content/182/11/7307 Downloaded from References This article cites 46 articles, 4 of which you can access for free at: http://www.jimmunol.org/content/182/11/7307.full#ref-list-1 http://www.jimmunol.org/ Why The JI? Submit online. • Rapid Reviews! 30 days* from submission to initial decision • No Triage! Every submission reviewed by practicing scientists • Fast Publication! 4 weeks from acceptance to publication by guest on September 25, 2021 *average Subscription Information about subscribing to The Journal of Immunology is online at: http://jimmunol.org/subscription Permissions Submit copyright permission requests at: http://www.aai.org/About/Publications/JI/copyright.html Email Alerts Receive free email-alerts when new articles cite this article. Sign up at: http://jimmunol.org/alerts The Journal of Immunology is published twice each month by The American Association of Immunologists, Inc., 1451 Rockville Pike, Suite 650, Rockville, MD 20852 Copyright © 2009 by The American Association of Immunologists, Inc. All rights reserved. Print ISSN: 0022-1767 Online ISSN: 1550-6606. The Journal of Immunology The Role of Intrapulmonary De Novo Lymphoid Tissue in Obliterative Bronchiolitis after Lung Transplantation1 Masaaki Sato,* Shin Hirayama,* David M. Hwang,*† Humberto Lara-Guerra,* Dirk Wagnetz,* Thomas K. Waddell,* Mingyao Liu,* and Shaf Keshavjee2* Chronic rejection after lung transplantation is manifested as obliterative bronchiolitis (OB). -

Silicosis: Pathogenesis and Changklan Muang Chiang Mai 50100 Thailand; Tel: 66 53 276364; Fax: 66 53 273590; E-Mail
Central Annals of Clinical Pathology Bringing Excellence in Open Access Review Article *Corresponding author Attapon Cheepsattayakorn, 10th Zonal Tuberculosis and Chest Disease Center, 143 Sridornchai Road Silicosis: Pathogenesis and Changklan Muang Chiang Mai 50100 Thailand; Tel: 66 53 276364; Fax: 66 53 273590; E-mail: Biomarkers Submitted: 04 October 2018 Accepted: 31 October 2018 1,2 3 Attapon Cheepsattayakorn * and Ruangrong Cheepsattayakorn Published: 31 October 2018 1 10 Zonal Tuberculosis and Chest Disease Center, Chiang Mai, Thailand ISSN: 2373-9282 2 Department of Disease Control, Ministry of Public Health, Thailand Copyright 3 Department of Pathology, Faculty of Medicine, Chiang Mai University, Chiang Mai, Thailand © 2018 Cheepsattayakorn et al. OPEN ACCESS Abstract Ramazzini first described this disease, namely “Pneumonoultramicroscopicsilicovolcanokoniosis” Keywords and then was changed according to the types of exposed dust. No reliable figures on the silica- • Silicosis inhalation exposed individuals are officially documented. How silica particles stimulate pulmonary • Biomarkers response and the exact path physiology of silicosis are still not known and urgently require further • Pathogenesis research. Nevertheless, many researchers hypothesized that pulmonary alveolar macrophages play a major role by secreting fibroblast-stimulating factor and re-ingesting these ingested silica particles by the pulmonary alveolar macrophage with progressive magnification. Finally, ending up of the death of the pulmonary alveolar macrophages and the development of pulmonary fibrosis appear. Various mediators, such as CTGF, FBRS, FGF2/bFGF, and TNFα play a major role in the development of silica-induced pulmonary fibrosis. A hypothesis of silicosis-associated abnormal immunoglobulins has been postulated. In conclusion, novel studies on pathogenesis and biomarkers of silicosis are urgently needed for precise prevention and control of this silently threaten disease of the world. -

Pneumoconiosis
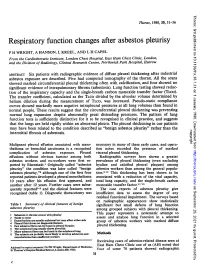
Prim Care Respir J 2013; 22(2): 249-252 PERSPECTIVE Pneumoconiosis *Paul Cullinan1, Peter Reid2 1 Consultant Physician, Royal Brompton and Harefield NHS Foundation Trust, London, UK 2 Consultant Physician, Western General Hospital, Edinburgh, UK Introduction Figure 1. Asbestosis; the HRCT scan shows the typical The pneumoconioses are parenchymal lung diseases that arise from picture of subpleural fibrosis (solid arrow); in addition inhalation of (usually) inorganic dusts at work. Some such dusts are there is diffuse, left-sided pleural thickening (broken biologically inert but visible on a chest X-ray or CT scan; thus, while arrow), characteristic too of heavy asbestos exposure they are radiologically alarming they do not give rise to either clinical disease or deficits in pulmonary function. Others – notably asbestos and crystalline silica – are fibrogenic so that the damage they cause is through the fibrosis induced by the inhaled dust rather than the dust itself. Classically these give rise to characteristic radiological patterns and restrictive deficits in lung function with reductions in diffusion capacity; importantly, they may progress long after exposure to the causative mineral has finished. In the UK and similar countries asbestosis is the commonest form of pneumoconiosis but in less developed parts of the world asbestosis is less frequent than silicosis; these two types are discussed in detail below. Other, rarer types of pneumoconiosis include stannosis (from tin fume), siderosis (iron), berylliosis (beryllium), hard metal disease (cobalt) and coal worker’s pneumoconiosis. Asbestosis Clinical scenario How is the diagnosis made? Asbestosis is the ‘pneumoconiosis’ that arises from exposure to A man of 78 reports gradually worsening breathlessness; he has asbestos in the workplace.1 The diagnosis is made when, on the no relevant medical history of note and has never been a regular background of heavy occupational exposure to any type of asbestos, smoker. -
Respiratory Function Changes After Asbestos Pleurisy
Thorax: first published as 10.1136/thx.35.1.31 on 1 January 1980. Downloaded from Thorax, 1980, 35, 31-36 Respiratory function changes after asbestos pleurisy P H WRIGHT, A HANSON, L KREEL, AND L H CAPEL From the Cardiothoracic Institute, London Chest Hospital, East Ham Chest Clinic, London, and the Division of Radiology, Clinical Research Centre, Northwick Park Hospital, Harrow ABSTRACT Six patients with radiographic evidence of diffuse pleural thickening after industrial asbestos exposure are described. Five had computed tomography of the thorax. All the scans showed marked circumferential pleural thickening often with calcification, and four showed no significant evidence of intrapulmonary fibrosis (asbestosis). Lung function testing showed reduc- tion of the inspiratory capacity and the single-breath carbon monoxide transfer factor (TLco). The transfer coefficient, calculated as the TLCO divided by the alveolar volume determined by helium dilution during the measurement of TLco, was increased. Pseudo-static compliance curves showed markedly more negative intrapleural pressures at all lung volumes than found in normal people. These results suggest that the circumferential pleural thickening was preventing normal lung expansion despite abnormally great distending pressures. The pattern of lung function tests is sufficiently distinctive for it to be recognised in clinical practice, and suggests that the lungs are held rigidly within an abnormal pleura. The pleural thickening in our patients may have been related to the condition described as "benign asbestos pleurisy" rather than the copyright. interstitial fibrosis of asbestosis. Malignant pleural effusion associated with meso- necessary in many of these early cases, and opera- thelioma or bronchial carcinoma is a recognised tion notes recorded the presence of marked http://thorax.bmj.com/ complication of asbestos exposure. -

Pneumoconiosis in Coalminers
6I8 POSTGRADUATE MEDICAL JOURNAL December I949 Postgrad Med J: first published as 10.1136/pgmj.25.290.618 on 1 December 1949. Downloaded from IRVINE, L. G., SIMSON, F. W., and STRACHAN, A. S. (1930), NEW YORK STATE DEPARTMENT OF LABOUR (1949), Proc. Intern. Conf. on Silicosis in Johannesburg, I.L.O. Studies Monthly Review, 28, No. 4, April. and Reports, Series F. (Industrial Hygiene), No. I3, p. 259. PERRY, K. M. A. (1948), Proc. Ninth Intern. Cong. of Ind. Med., JONES, W. R. (I933), ,. of Hyg., 33, 307. London (in the press). KETTLE, E. H. (I932), Y. Path. and Bat., 35, 395. KETTLE, E. H. (I934), Ibid., 38, 20o. POLICARD, A. (1947), Proc. Conf. of the Institution of Mining KING, E. J. (I945), M.R.C. Special Report Series, No. 250, p. 73. Engineers and Institution of Mining and Metalurgy, London, KING, E. J. (I947) Occ. Med., 4, 26. P. 24. KING, E. J., WRI6HT, B. M., and RAY, S. C. (I949), Paper read ROGERS, E. (i944), Paper read to the British Tuberculosis Associa- to the Path. Soc., Great Britain, January, 1949. tion. McLAUGHLIN, A. I. G., ROGERS, E., and DUNHAM, K. C. (I949), Brit. 3Y. Ind. Med., 6, I84. SHAVER, C. G. (1948), Radiology, 50, 760. MINERS' PHTHISIS MEDICAL BUREAU OF SOUTH SHAVER, C. G., and RIDDELL, A. R. (I947), J. Id. Hyg. and AFRICA (1946), Report for the Three Years ending Jy 31, Tox., 29, 145. I944 (South African Government Printer). VORWALD, A. J., and CARR, J. W. (1938), Amer. J7. Path., 14,49. PNEUMOCONIOSIS IN COAL MINERS By J. -

Progressive Plasterer's Pneumoconiosis Complicated By
Kurosaki et al. BMC Pulmonary Medicine (2019) 19:6 https://doi.org/10.1186/s12890-018-0776-4 CASEREPORT Open Access Progressive plasterer’s pneumoconiosis complicated by fibrotic interstitial pneumonia: a case report Fumio Kurosaki1,2*, Tamiko Takemura3, Masashi Bando1, Tomonori Kuroki1,2, Toshio Numao2, Hiroshi Moriyama4 and Koichi Hagiwara1 Abstract Background: Although the prevalence of pneumoconiosis has been decreasing due to improvements in working conditions and regular health examinations, occupational hygiene measures are still being established. Plasterers encounter a number of hazardous materials that may be inhaled in the absence of sufficient protection. Case presentation: A 64-year-old man who plastered without any dust protection for more than 40 years was referred to our hospital with suspected interstitial pneumonia. Mixed dust pneumoconiosis and an unusual interstitial pneumonia (UIP) pattern with fibroblastic foci were diagnosed by video-assisted thoracoscopic surgery, and an elemental analysis detected elements included in plaster work materials. Despite the cessation of plaster work and administration of nintedanib, the patient developed advanced respiratory failure. Conclusion: Plasterers are at an increased risk of pneumoconiosis and may have a poor prognosis when complicated by the UIP pattern. Thorough dust protection and careful monitoring are needed. Keywords: Plasterer, Pneumoconiosis, Usual interstitial pneumonia, Elemental analysis Background unusual interstitial pneumonia (UIP) pattern, the cause of With energy transition from coal to oil and nuclear power, which was identified as plaster work by an elemental coal mines completely disappeared by the early first analysis. Therefore, plasterers need to take proper coun- decade of the 2000s in Japan. Furthermore, improvements termeasures for dust prevention and undergo regular in industrial hygiene and vocational education have examinations. -

Pathological Aspects of Asbestosis
POSTGRAD. MED. J. (1966), 42, 613. Postgrad Med J: first published as 10.1136/pgmj.42.492.613 on 1 October 1966. Downloaded from PATHOLOGICAL ASPECTS OF ASBESTOSIS D. O'B. HOURIHANE, M.D., M.C.Path., D.C.P.(Lond.), M.R.C.P.I. W. T. E. MCCAUGHEY, M.D., M.C.Path. School ofPathology, Trinity College, Dublin WIDESPREAD recognition of asbestosis dates from the work of Merewether and Price in 1930. They investigated 363 asbestos workers and concluded that there was a pneumoconiosis resulting from asbestos inhalation, that this condition shortened life, and that measures to diminish the atmospheric concentration of asbestos dust would reduce the incidence of the disease. In 1931 asbestosis was accepted as a compensatable disease in Great Britain and steps were taken to reduce the risk in the asbestos industry. 18 years later Wyers (1949) found that the age at death in this disorder had Protected by copyright. increased and that finger-clubbing had become more common. He suggested that these changes were due to a more chronic form of the disease resulting from improved dust control in the industry following the legislation of 1931. Currently however, the number of new cases of asbestosis in Great Britain is increasing, their frequency suggesting an incidence rate of at least five per thousand of those occupation- ally exposed (McVittie, 1965). Though earlier reports indicated that tuberculosis was common in asbestosis (Wyers, 1949; Gloyne, 1951; Bonser, Foulds and Stewart, 1955) it appears to be a rare I 0 n < ,. ' complication at the present time (Buchanan, 1965). -

Screening of Pulmonary Hypertension in Chronic Obstructive Pulmonary Disease and Silicosis by Discriminant Functions
Eur Resplr J 1992, 5, 444-451 Screening of pulmonary hypertension in chronic obstructive pulmonary disease and silicosis by discriminant functions H. Evers, F. Liehs, K. Harzbecker, D. Wenzel, A. Wilke, W. Pielesch, J. Schauer, W. Nahrendorf, J. Preisler, A. Luther, D. Scheuler, W. Reimer, W. Schilling Screening of pulmonary hypertension in chronic obstructive pulmonary disease and Research Project Lung Diseases of the silicosis by discriminant functions. H. Evers, F. Liehs, K. Harzbecker, D. Wenzel, A. Ministry of Health, Berlin. Wilke, W. Pielesch, J. Schauer, W. Nahrendorf, J. Preisler, R. Luther, D. Scheuler, W. Reimer, W. Schilling. ABSTRACT: The aim of our prospective multicentric study was to develop a Correspondence: H. Evers Chest Clinic screening method for pulmonary hypertension in patients with chronic lung diseases. Str. nach Fichtenwalde 16 We investigated 710 patients in 10 hospitals: 315 males and 109 females with chronic D(o)·1504 Beelitz-Heilstiitten obstructive pulmonary disease, and 286 males with silicosis. Manifest pulmonary Germany. hypertension was defined as pulmonary artery pressure > 20 mmHg (2.7 kPa) at rest. The multivariate statistical method used was a stepwise discriminant analysis. In males with chronic obstructive pulmonary disease, the diameter of the right Keywords: descending pulmonary artery, forced expiratory volume in one second {FEV ) Chronic obstructive pulmonary disease 1 discriminant analysis ) arterial oxygen tension (Pao1 at rest, and age turned out to be relevant for dis crimilllltion of groups with and without manifest pulmonary hypertension. For pulmonary hypertension screening females the FEV/FVC (forced vital capacity) ratio replaced the absolute value of silicosis. FEV1 in the calculated discriminant function. -

08-0205: N.M. and DEPARTMENT of the NAVY, PUGET S
United States Department of Labor Employees’ Compensation Appeals Board __________________________________________ ) N.M., Appellant ) ) and ) Docket No. 08-205 ) Issued: September 2, 2008 DEPARTMENT OF THE NAVY, PUGET ) SOUND NAVAL SHIPYARD, Bremerton, WA, ) Employer ) __________________________________________ ) Appearances: Oral Argument July 16, 2008 John Eiler Goodwin, Esq., for the appellant No appearance, for the Director DECISION AND ORDER Before: DAVID S. GERSON, Judge COLLEEN DUFFY KIKO, Judge JAMES A. HAYNES, Alternate Judge JURISDICTION On October 30, 2007 appellant filed a timely appeal from a November 17, 2006 decision of the Office of Workers’ Compensation Programs denying his occupational disease claim. Pursuant to 20 C.F.R. §§ 501.2(c) and 501.3, the Board has jurisdiction over the merits of the claim. ISSUE The issue is whether appellant has established that he sustained occupational asthma in the performance of duty due to accepted workplace exposures. On appeal, he, through his attorney, asserts that the Office did not provide Dr. William C. Stewart, the impartial medical examiner, with a complete, accurate statement of accepted facts. FACTUAL HISTORY On December 8, 2004 appellant, then a 57-year-old insulator, filed an occupational disease claim (Form CA-2) asserting that he sustained occupational asthma and increasing shortness of breath due to workplace exposures to fiberglass, silicates, welding smoke, polychlorobenzenes, rubber, dusts, gases, fumes and smoke from “burning out” submarines from 1991 through January -

Concurrent Silicosis and Pulmonary Mycosis at Death
DISPATCHES B35–B49 (any mycosis). We defi ned pulmonary myco- Concurrent sis as death with ICD-9 and ICD-10 codes 112.4/B37.1 (candidiasis); 114/B38.0, B38.1, B38.2, B38.9 (coccid- Silicosis and ioidomycosis); 115/B39.0, B39.1, B39.2, B39.4, B39.9 (histoplasmosis); 116.0/B40.0, B40.1, B40.2, B40.9 (blas- Pulmonary tomycosis); 116.1/B41.0, B41.9 (paracoccidioidomyco- sis); 117.1/B42.0, B42.9 (sporotrichosis); 117.7/B46.0, Mycosis at Death B46.5, B46.9 (zygomycosis); 117.3/B44.0, B44.1, B44.9 Yulia Iossifova,1 Rachel Bailey, John Wood, (aspergillosis); 117.5/B45.0, B45.9 (cryptococcosis); and and Kathleen Kreiss 118/B48.7 (opportunistic mycoses). For many mycoses, ICD-9 codes do not differentiate pulmonary from other To examine risk for mycosis among persons with sili- types of mycoses. For ICD-10 codes, we limited data to cosis, we examined US mortality data for 1979–2004. Per- mycoses coded as pulmonary, opportunistic, and some sons with silicosis were more likely to die with pulmonary unspecifi ed type of mycoses (e.g., B38.9, B39.4, B39.9, mycosis than were those without pneumoconiosis or those with more common pneumoconioses. Health profession- B40.9, B41.9, B42.9, B44.9, B45.9, B46.5, and B46.9). als should consider enhanced risk for mycosis for silica- We provided results with and without ICD-9 code for op- exposed patients. portunistic mycoses and ICD-10 codes for unspecifi ed mycoses and opportunistic mycoses. We computed prevalence rate ratios and 95% con- he pneumoconioses are a group of irreversible but fi dence intervals (CIs) to separately compare pulmonary Tpreventable interstitial lung diseases, most commonly mycosis prevalence at death among persons with silicosis, associated with inhalation of asbestos fi bers, coal mine asbestosis, and CWP with that for persons in the refer- dust, or crystalline silica dust. -

The Lung in Rheumatoid Arthritis
ARTHRITIS & RHEUMATOLOGY Vol. 70, No. 10, October 2018, pp 1544–1554 DOI 10.1002/art.40574 © 2018, American College of Rheumatology REVIEW The Lung in Rheumatoid Arthritis Focus on Interstitial Lung Disease Paolo Spagnolo,1 Joyce S. Lee,2 Nicola Sverzellati,3 Giulio Rossi,4 and Vincent Cottin5 Interstitial lung disease (ILD) is an increasingly and histopathologic features with idiopathic pulmonary recognized complication of rheumatoid arthritis (RA) fibrosis, the most common and severe of the idiopathic and is associated with significant morbidity and mortal- interstitial pneumonias, suggesting the existence of com- ity. In addition, approximately one-third of patients have mon mechanistic pathways and possibly therapeutic tar- subclinical disease with varying degrees of functional gets. There remain substantial gaps in our knowledge of impairment. Although risk factors for RA-related ILD RA-related ILD. Concerted multinational efforts by are well established (e.g., older age, male sex, ever smok- expert centers has the potential to elucidate the basic ing, and seropositivity for rheumatoid factor and anti– mechanisms underlying RA-related UIP and other sub- cyclic citrullinated peptide), little is known about optimal types of RA-related ILD and facilitate the development of disease assessment, treatment, and monitoring, particu- more efficacious and safer drugs. larly in patients with progressive disease. Patients with RA-related ILD are also at high risk of infection and drug toxicity, which, along with comorbidities, compli- Introduction cates further treatment decision-making. There are dis- Pulmonary involvement is a common extraarticular tinct histopathologic patterns of RA-related ILD with manifestation of rheumatoid arthritis (RA) and occurs, to different clinical phenotypes, natural histories, and prog- some extent, in 60–80% of patients with RA (1,2).