Effectiveness of 4 Weeks Task Specific Training in Improving Postural
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Belgaum District Lists
Group "C" Societies having less than Rs.10 crores of working capital / turnover, Belgaum District lists. Sl No Society Name Mobile Number Email ID District Taluk Society Address 1 Abbihal Vyavasaya Seva - - Belgaum ATHANI - Sahakari Sangh Ltd., Abbihal 2 Abhinandan Mainariti Vividha - - Belgaum ATHANI - Uddeshagala S.S.Ltd., Kagawad 3 Abhinav Urban Co-Op Credit - - Belgaum ATHANI - Society Radderahatti 4 Acharya Kuntu Sagara Vividha - - Belgaum ATHANI - Uddeshagala S.S.Ltd., Ainapur 5 Adarsha Co-Op Credit Society - - Belgaum ATHANI - Ltd., Athani 6 Addahalli Vyavasaya Seva - - Belgaum ATHANI - Sahakari Sangh Ltd., Addahalli 7 Adishakti Co-Op Credit Society - - Belgaum ATHANI - Ltd., Athani 8 Adishati Renukadevi Vividha - - Belgaum ATHANI - Uddeshagala S.S.Ltd., Athani 9 Aigali Vividha Uddeshagala - - Belgaum ATHANI - S.S.Ltd., Aigali 10 Ainapur B.C. Tenenat Farming - - Belgaum ATHANI - Co-Op Society Ltd., Athani 11 Ainapur Cattele Breeding Co- - - Belgaum ATHANI - Op Society Ltd., Ainapur 12 Ainapur Co-Op Credit Society - - Belgaum ATHANI - Ltd., Ainapur 13 Ainapur Halu Utpadakari - - Belgaum ATHANI - S.S.Ltd., Ainapur 14 Ainapur K.R.E.S. Navakarar - - Belgaum ATHANI - Pattin Sahakar Sangh Ainapur 15 Ainapur Vividha Uddeshagal - - Belgaum ATHANI - Sahakar Sangha Ltd., Ainapur 16 Ajayachetan Vividha - - Belgaum ATHANI - Uddeshagala S.S.Ltd., Athani 17 Akkamahadevi Vividha - - Belgaum ATHANI - Uddeshagala S.S.Ltd., Halalli 18 Akkamahadevi WOMEN Co-Op - - Belgaum ATHANI - Credit Society Ltd., Athani 19 Akkamamhadevi Mahila Pattin - - Belgaum -

Prl. District and Session Judge, Belagavi. SRI. BASAVARAJ I ADDL
Prl. District and Session Judge, Belagavi. SRI. BASAVARAJ I ADDL. DISTRICT AND SESSIONS JUDGE BELAGAVI Cause List Date: 18-09-2020 Sr. No. Case Number Timing/Next Date Party Name Advocate 1 M.A. 8/2020 Moulasab Maktumsab Sangolli A.D. (HEARING) Age 70Yrs R/o Bailhongal Dist SHILLEDAR IA/1/2020 Belagavi. Vs The Chief officer Bailhongal Town Municipal Council Tq Bailhongal Dist Belagavi. 2 L.A.C. 607/2018 Laxman Dundappa Umarani age C B Padnad (EVIDENCE) 65 Yrs R/o Kesaral Tq Athani Dt Belagavi Vs The SLAO Hipparagi Project , Athani Dist Belagavi. 3 L.A.C. 608/2018 Babalal Muktumasab Biradar C B Padanad (EVIDENCE) Patil Age 55 yrs R/o Athani Tq Athani Dt Belagavi. Vs The SLAO Hipparagi Project , Athani, Tq Athani Dist Belagavi. 4 L.A.C. 609/2018 Gadigeppa Siddappa Chili age C B padanad (EVIDENCE) 65 Yrs R/o Athani Tq Athani Dt Belagavi Vs The SLAO Hipparagi Project , Athani Dist Belagavi. 5 L.A.C. 610/2018 Kedari Ningappa Gadyal age 45 C B Padanad (EVIDENCE) Yrs R/o Athani Tq Athani Dt Belagavi Vs The SLAO Hipparagi Project , Athani Dist Belagavi. 6 L.A.C. 611/2018 Smt Kallawwa alias Kedu Bhima C B padanad (EVIDENCE) Pujari Vs The SLAO Hipparagi Project , Athani Dist Belagavi. 7 L.A.C. 612/2018 Kadappa Bhimappa Shirahatti C B Padanad (EVIDENCE) age 55 Yrs R/o Athani Tq Athani Dt Belagavi Vs The SLAO Hipparagi Project , Athani. Dist Belagavi. 1/8 Prl. District and Session Judge, Belagavi. SRI. BASAVARAJ I ADDL. DISTRICT AND SESSIONS JUDGE BELAGAVI Cause List Date: 18-09-2020 Sr. -

Government of Karnataka Revenue Village, Habitation Wise
Government of Karnataka O/o Commissioner for Public Instruction, Nrupatunga Road, Bangalore - 560001 RURAL Revenue village, Habitation wise Neighbourhood Schools - 2015 Habitation Name School Code Management Lowest Highest Entry type class class class Habitation code / Ward code School Name Medium Sl.No. District : Belgaum Block : BAILHONGAL Revenue Village : ANIGOL 29010200101 29010200101 Govt. 1 7 Class 1 Anigol K.H.P.S. ANIGOL 05 - Kannada 1 Revenue Village : AMATUR 29010200201 29010200201 Govt. 1 8 Class 1 Amatur K.H.P.S. AMATUR 05 - Kannada 2 Revenue Village : AMARAPUR 29010200301 29010200301 Govt. 1 5 Class 1 Amarapur K.L.P.S. AMARAPUR 05 - Kannada 3 Revenue Village : AVARADI 29010200401 29010200401 Govt. 1 8 Class 1 Avaradi K.H.P.S. AVARADI 05 - Kannada 4 Revenue Village : AMBADAGATTI 29010200501 29010200501 Govt. 1 7 Class 1 Ambadagatti K.H.P.S. AMBADAGATTI 05 - Kannada 5 29010200501 29010200502 Govt. 1 5 Class 1 Ambadagatti U.L.P.S. AMBADAGATTI 18 - Urdu 6 29010200501 29010200503 Govt. 1 5 Class 1 Ambadagatti K.L.P.S AMBADAGATTI AMBADAGATTI 05 - Kannada 7 Revenue Village : ARAVALLI 29010200601 29010200601 Govt. 1 8 Class 1 Aravalli K.H.P.S. ARAVALLI 05 - Kannada 8 Revenue Village : BAILHONGAL 29010200705 29010200755 Govt. 6 10 Ward No. 27 MURARJI DESAI RESI. HIGH SCHOOL BAILHONGAL(SWD) 19 - English 9 BAILHONGAL 29010200728 29010200765 Govt. 1 5 Class 1 Ward No. 6 KLPS DPEP BAILHONGAL BAILHONGAL 05 - Kannada 10 29010200728 29010212605 Govt. 1 7 Class 1 Ward No. 6 K.B.S.No 2 Bailhongal 05 - Kannada 11 Revenue Village : BAILWAD 29010200801 29010200801 Govt. 1 7 Class 1 Bailawad K.H.P.S. -
Department of Public Instruction - Karnataka
Department of Public Instruction - Karnataka Office / School / Designation / subject wise Vacancy details - Secondary - 2016 Note: Notified Vacancies are reserved at District Level,Total Vacancy includes Notified Vacancy Designation DISE CODE / School Name SUBJECT Total Cadre_Group Vacancy District: BELAGAVI Taluk: - Arts Instructor DRAWING 1 SPECIAL TEACHER Taluk Total 1 Taluk: BAILHONGAL 29010202502 - GOVT HIGHSCHOOL CHIKKABELLIKATTI Physical Education Teacher ( PET) PE - GRADE 1 1 PET CRAFT GRADE II CRAFT -TAILORING 1 SPECIAL TEACHER 29010204904 - GOVT HIGHSCHOOL HANNIKERI Assistant Master ( AM ) LANGUAGE KANNADA 1 AM GROUP 29010205604 - GOVT HIGHSCHOOL HANABARATTI Assistant Master ( AM ) LANGUAGE KANNADA 1 AM GROUP Assistant Master ( AM ) PCM KANNADA 1 AM GROUP Special Teacher CRAFT -TAILORING 1 SPECIAL TEACHER 29010212205 - GOVT HIGHSCHOOL VANNUR Assistant Master ( AM ) LANGUAGE KANNADA 1 AM GROUP Taluk Total 7 Taluk: BELAGAVI CITY 29010301904 - SARASWATI COMP JR COLLEGE W.NO.19.BGM.CITY. Assistant Master ( AM ) ARTS MARATHI 1 AM GROUP 29010302404 - GOVT CHINTMANRAO PU COLLEGE W.NO.24.BGM.CITY. Special Teacher MUSIC 1 SPECIAL TEACHER Taluk Total 2 Taluk: BELAGAVI RURAL. 29010404511 - GOVT HIGHSCHOOL HIREBAGEWADI Assistant Master ( AM ) LANGUAGE KANNADA 1 AM GROUP 29010407206 - GOVT HIGHSCHOOL K.K.KOP. Assistant Master ( AM ) ARTS KANNADA 2 AM GROUP 29010408101 - KHPS MASTMARDI Assistant Master ( AM ) ARTS KANNADA 1 AM GROUP 29010408102 - GOVT HIGHSCHOOL MASTMARDI Assistant Master ( AM ) LANGUAGE KANNADA 1 AM GROUP 29010408202 - GOVT -

Prl. District and Session Judge, Belagavi. Sri
Prl. District and Session Judge, Belagavi. Sri. Chandrashekhar Mrutyunjaya Joshi PRL. DISTRICT AND SESSIONS JUDGE BELAGAVI Cause List Date: 05-09-2020 Sr. No. Case Number Timing/Next Date Party Name Advocate 11.00 AM-02.00 PM 1 R.A. 64/2020 Sidram Vaijanaik Shivanaikar B.B. (NOTICE) age 40 yrs R/o No. 356 M Block Lakkannavar IA/1/2020 Ramappa nagar Mysore IA/2/2020 Vs Usharani Chandrashekhar Kenganur age 65 yrs R/o Kabbur Tq /Dt Dharwad 2 COMM.O.S 47/2020 Jayashri C Konnur age 42 yrs V.A.chandargi (NOTICE) R/o Laxmi Badawane Gokak Vs Vijay B. Bhutda R/o Wali Shield Products Belagavi 3 COMM.O.S 7/2020 M/s Sairaj Builders and R.B.Deshpande (A.D.R.) Developers 356/1A MG road Tilakwadi Belagavi Vs Govind Mahadev Raut age 77 yrs R/o P.No.2 Swami Vivekanand Colony Tilakwadi Belagavi 4 R.A. 63/2020 Yallappa Balu More age 65 yrs M.M.Shaikh (ARGUMENTS) R/o H.No.5/B Chavat galli IA/1/2020 Kavallawadi Tq /Dt Belagavi IA/2/2020 Vs Appasaheb Tavanappa Desai age 54 yrs R/o H.No.51 Kutalwadi Tq/Dt Belagavi 5 A.S. 16/2019 Shri Bhakti construction Pvt Satish G (Steps) Ltd,R/by R.S.Patil,Eknath Biradar IA/3/2019 Hunnargikar R/o.1809/3,Kelkar IA/1/2019 Bag Belagavi IA/2/2019 Vs Shreemata Co Op Credit Society Ltd (Multi State) O/at. New Goodshed Rd,Belagavi,R/by Umesh S Gavade 6 A.S. -

Belagavi (Belgaum)
KARNATAKA EXAMINATIONS AUTHORITY Admission to Karnataka Residential Educational Institutions Society, Bengaluru - 2020-21 RANK LIST DISTRICT: DD BELAGAVI (BELGAUM) SL CETNO CANDIDATE NAME Sex DOB FATHER NAME SCORE STATE RANK NO 1 DP814 HALAPPA ANAND ANTRAGATTI M 06-MAR-09 ANAND ANTRAGATTI 88 1 2 DU003 PADMARAJ GANAPATI PUJERI M 19-JAN-09 GANAPATI PUJERI 87 2 3 DQ249 VASANTAGOUDA SIDDAPPA B M 27-JAN-09 SIDDAPPA B PATIL 86 4 PATIL 4 EC137 ASWINI MADIVALAR F 01-MAR-09 MANTESH 86 5 5 DP701 SAMBRHAM RAVINDRA KUMBAR M 03-DEC-08 RAVINDRA KUMBAR 85 9 6 EM256 SANDEEP PARASHURAM LAMANI M 23-APR-09 PARSHURAM LAMANI 85 11 7 DR726 SUNANDA MALYAGOL F 01-JUN-09 MALLAPPA 85 13 8 DH176 VISHAL YARAGATTI M 29-AUG-08 BASAPPA 84 17 9 DR122 MANJUNATH MANNIKERI M 27-NOV-08 MALLAPPA 84 19 10 EM212 VAIBHAVI SANGAPPA EALAJARI F 10-FEB-09 SANGAPPA EALAJARI 84 23 11 DR686 AISHWARY. R. SURRANNAVAR F 17-NOV-09 RAGHAVENDRA 84 26 12 EK366 BASAVARAJ SIDABASANAVAR M 14-MAY-08 BALAPPA 83 27 13 DJ507 YALLALING HADIMANI M 29-JUL-08 RAVEENDRA 83 28 14 DQ003 SHUSHANT HIPPARAGI M 04-NOV-08 KRISHNAPPA 83 29 15 DR635 SANJANA MALLIKARJUN BELKUD F 27-NOV-08 MALLIKARJUN BELKUD 83 31 16 DR470 LAXMI BIRADAR,PATIL F 21-DEC-08 BHIMAPPA 83 32 17 DS289 PRAMOD KARTAMMAD M 16-JAN-09 SURESH 83 33 18 DD153 ADITYA ISHWAR KHICHADI M 24-JAN-09 ISHWAR GHATIGEPPA KHICHADI 83 35 19 EB812 DHANESWARI SHASHIDHAR F 08-FEB-09 SHASHIDHAR KURGUND 83 36 KURGUND 20 DA576 SANGAMESH GOUDAPPA M 18-JUL-09 GOUDAPPA ISHWAR CHANNANNAVAR 83 44 CHANNANNAVAR 21 DP792 OMKAR NELADHARI M 24-DEC-09 AJIT 83 48 22 DQ145 -

Government AYUSHMAN BHARAT
AYUSHMAN BHARAT - AROGYA KARNATAKA EMPANELLED HOSPITALS LIST Govt/Priv Sl.no Hospital Name Address District Taluk Division Contact Mail id Scheme Speciality ate Government Community Health Centre Obstetrics and VijayapuraDevanahalli Ayushman gynaecology Community Health Centre Road Vijayapura Bangalore chcvijayapura@g 1 Bangalore Devanahalli govt 8027668505 Bharat - Arogya Dental Vijayapura Devanhalli division mail.com Karnataka Simple secondary general TalukBengaluru Rural- procedure 562135 Obstetrics and Ayushman Community Health Centre B M Road Kengeri Kote Bangalore girijagowdab@g gynaecology Paediatrics 2 Bangalore Bengaluru govt 8028483265 Bharat - Arogya Kengeri Bangalore 560060 division mail.com Simple secondary General Karnataka procedure Paediatric surgeries Community Health Centre Obstetrics and Ayushman Community Health Centre ThyamagondluNear Police Bangalore thyamagondluchc gynaecology 3 Bangalore Nelemangala govt 8027731202 Bharat - Arogya Thyamagondlu StationBangalore - Rural- division @gmail.com Dental Karnataka 562132 Simple secondary General procedure Paediatric Surgery Community Health Center Ayushman General Medicine Community Health Center Near Water Bangalore mophcavalhalli@ 4 Bangalore Bengaluru govt 8028473108 Bharat - Arogya Dental Avalahalli PlantationBangalore - division gmail.com Karnataka Obstetrics and Urban-560049 gynaecology Dental Obstetrics and Ayushman Tavarekere Hobli South Bangalore dr.candrappacercl gynaecology 5 CHC Chandrappa Cercle Bangalore Bengaluru govt 8028438330 Bharat - Arogya TalukBengaluru -

Kle Institute of Technology, Hubballi Form Iso 9001: 2015
K.L.E. Society’s FORM K.L.E. INSTITUTE OF TECHNOLOGY, HUBBALLI ISO 9001: 2015 - KLEIT Document #: FMTP0506 Title: Branch wise Placement Details Rev: 2.0 Academic Year: 2019-2020 SL Salary Company Students Name No Package 1 TCS 1. Sahana 2. Sereen Kouser M Mokhashi 4 LPA 2 KPIT 1. Vilas Chandrashekhar Hosur 3.25 LPA 1. Venkamma Veman Shalavadi Hexaware Software 2. Shreshta ShivanandvJodalli 3 3. Nireeksha Manohar Shetty 4. Saumya Shivanand Rane 4 LPA 5. Sachin Ramesh Ukkali 1. Shivaprasad T. Shirawar 2. Vishal Shalgar 3. Vijayalakshmi Paramshetti 4 Cognizant Technologies 4. Sameerbanu Budihal 5. Swathi C. Shyavi 6. Vijaylaxmi A. Pujari 3.6 LPA 7. Chaitra S. Biradar 8. Sneha Grampurohit 9. Megha A. Naragund 10. Akshaykumar B. Harnal 1. Deepa S. Banakar 5 INFOSYS 2. Kaveri M. Bhavanur 3. Seema S. Kanagond 4 LPA 4. Abhijeet A. Saralaya K.L.E. Society’s FORM K.L.E. INSTITUTE OF TECHNOLOGY, HUBBALLI ISO 9001: 2015 - KLEIT Document #: FMTP0506 Title: Branch wise Placement Details Rev: 2.0 5. Vaishnavi R. Dhotargavi 6. Akshata P. Patil 6 WIPRO 1. Nireeksha M. Shetty 2. Vishal R. Shalgar 3.5 LPA 3. Akshaykumar B. Haranal 1. Manjunathgouda Patil 7 SLK 2. Mallikarjun Somanni 3. Shreya Arkasali 3.20 LPA 4. Ashwini Benni 5. Asha Naik 8 SiFive 1. Gayatri Pattar 2.5 LPA nd 9 WIPRO (2 time) 1. Shivanand Satyannavar 3.5 LPA 2. Vijaylaxmi Pujari nd 10 Cognizant (2 time) 1. Seema S. Kanagond 3.6 LPA K.L.E. Society’s FORM K.L.E. INSTITUTE OF TECHNOLOGY, HUBBALLI ISO 9001: 2015 - KLEIT Document #: FMTP0506 Title: Branch wise Placement Details Rev: 2.0 Academic Year: 2018-2019 SL Company Students Name Salary Package No 1. -

List of Members
Karnataka Jain Association (R.) No. 81, K.R. Road, Shankarapuram, Bangalore - 560 004 Revised Members (Voters) list as on 01.03.2019 Sl.No. Name M.S. No. Place Taluk District 1 Abha Jain 2277 Bangalore Bangalore Bangalore 2 Abhay Kumar Jayakumar Patil 6814 Konnur Gokak Belagavi 591 231 3 Abhay Kumar M. Sooji 6677 Hubli Hubli Hubli 580 023 4 Abhay Kumar Managavi 4949 Rajajinagar Bangalore Bangalore 560 010 5 Abhay Kumar Padiwal M 2744 Bangalore Bangalore Bangalore 6 Abhay Kumar Payappa Vaghe 6909 Sadalaga Chikkodi Belagavi 591 239 7 Abhay Prasad 4725 Nagarabavi Bangalore Bangalore 560 072 8 Abhay Sridhar Rokhade 3867 Deshpande Nagar Hubli Dharwad 580 029 9 Abhay Vidyadhar Avalakki 5221 Patil Galli Angol Belagavi 590 006 10 Abhaya Bhupal Nagave 3282 Borgaon Chikkodi Belgaum 591216 11 Abhaya H.D. 7812 B.M Road Hassan Hassan 573 201 12 Abhaya Kumar Banappa Muggannavar 3414 Mahishavadagi Athani Belgaum 591240 13 Abhaya Kumar H D 198 Hassan Hassan Hassan 14 Abhaya Kumar S.A. 3244 Vijayanagar Bangalore Bangalore 560040 15 Abhaya Kumar Shanthinatha 2151 Harugeri Rayabag Belgaum Khemalapure 16 Abhaya Kumar Shreepal Karole 3279 Borgaon Chikkodi Belgaum 591216 17 Abhaya S Kagi Dr. 5448 Sindagi Sindagi Bijapur 586 128 18 Abhayachandra K 2779 Moodbidri Moodbidri Dakshina Kannada 19 Abhayakumar A.J. 7481 Vidyanagar Tumkur Tumkur 572 102 20 Abhayakumar Bhujabali Hardi 1717 Belgaum Belgaum Belgaum 21 Abhayakumar Jinagouda Koth 6503 Shamanewadi Chikkodi Belagavi 591 214 22 Abhayakumar Magadum 6465 R V College Bangalore Bangalore 560 059 23 Abhayakumar Mallappa Kaddu 7823 Kudachi Rayabagh Belagavi 591 311 24 Abhayakumar P 329 Bangalore Bangalore Bangalore 25 Abhayakumar P. -
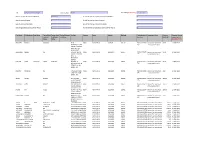
Dividend for the Year 2006-2007
CIN L01542KA1995PLC019046 Company Name BLANK Date Of AGM(DD-MON-YYYY) 28-AUG-2013 Sum of unpaid and unclaimed dividend 882971.43 Sum of interest on unpaid and unclaimed dividend 0 Sum of matured deposit 0 Sum of interest on matured deposit 0 Sum of matured debentures 0 Sum of interest on matured debentures 0 Sum of application money due for refund 0 Sum of interest on application money due for refund 0 First Name Middle Name Last Name Father/Husb Father/Husb Father/Husband Address Country State District PINCode Folio Number of Investment Type Amount Proposed Date of and First and Middle Last Name Securities Due(in Rs.) transfer to IEPF Name Name (DD-MON-YYYY) NINGAPPA DEGINAL SIDDARAY NEAR INDIA KARNATAKA BIJAPUR 586117 IN30113526529 Amount for unclaimed 20.00 11-MAR-2015 REVANASIDDESWA 187 and unpaid dividend R TEMPLE AT POST HORTI INDI TQ BIJAPUR DIST BASAVARAJ KARADI NA SHIVAPUTRAPPA INDIA KARNATAKA BAGALKOT 587207 IN30214810605 Amount for unclaimed 10.00 11-MAR-2015 KARADI TEACHER 216 and unpaid dividend H P S S L MALHAPUR BADAMI HAROON SATAR PEERJADE SATAR PEERJADE PLOT NO. 92 INDIA KARNATAKA BELGAUM 590001 IN30189510231 Amount for unclaimed 54.00 11-MAR-2015 SECTOR NO. 9 M M 792 and unpaid dividend EXTN BELGAUM, KARNATAKA MADHAV MIRAJKAR NA 3 HAVLOCK ROAD INDIA KARNATAKA BELGAUM 590001 IN30036010348 Amount for unclaimed 4.00 11-MAR-2015 CAMP BELGAUM 679 and unpaid dividend KARNATAKA SAHAR JEELANI AKRAM 4877/36 RACE INDIA KARNATAKA BELGAUM 590001 IN30113526647 Amount for unclaimed 104.00 11-MAR-2015 COURSE DOUBLE 273 and unpaid dividend -

Bedkar Veedhi S.O Bengaluru KARNATAKA
pincode officename districtname statename 560001 Dr. Ambedkar Veedhi S.O Bengaluru KARNATAKA 560001 HighCourt S.O Bengaluru KARNATAKA 560001 Legislators Home S.O Bengaluru KARNATAKA 560001 Mahatma Gandhi Road S.O Bengaluru KARNATAKA 560001 Rajbhavan S.O (Bangalore) Bengaluru KARNATAKA 560001 Vidhana Soudha S.O Bengaluru KARNATAKA 560001 CMM Court Complex S.O Bengaluru KARNATAKA 560001 Vasanthanagar S.O Bengaluru KARNATAKA 560001 Bangalore G.P.O. Bengaluru KARNATAKA 560002 Bangalore Corporation Building S.O Bengaluru KARNATAKA 560002 Bangalore City S.O Bengaluru KARNATAKA 560003 Malleswaram S.O Bengaluru KARNATAKA 560003 Palace Guttahalli S.O Bengaluru KARNATAKA 560003 Swimming Pool Extn S.O Bengaluru KARNATAKA 560003 Vyalikaval Extn S.O Bengaluru KARNATAKA 560004 Gavipuram Extension S.O Bengaluru KARNATAKA 560004 Mavalli S.O Bengaluru KARNATAKA 560004 Pampamahakavi Road S.O Bengaluru KARNATAKA 560004 Basavanagudi H.O Bengaluru KARNATAKA 560004 Thyagarajnagar S.O Bengaluru KARNATAKA 560005 Fraser Town S.O Bengaluru KARNATAKA 560006 Training Command IAF S.O Bengaluru KARNATAKA 560006 J.C.Nagar S.O Bengaluru KARNATAKA 560007 Air Force Hospital S.O Bengaluru KARNATAKA 560007 Agram S.O Bengaluru KARNATAKA 560008 Hulsur Bazaar S.O Bengaluru KARNATAKA 560008 H.A.L II Stage H.O Bengaluru KARNATAKA 560009 Bangalore Dist Offices Bldg S.O Bengaluru KARNATAKA 560009 K. G. Road S.O Bengaluru KARNATAKA 560010 Industrial Estate S.O (Bangalore) Bengaluru KARNATAKA 560010 Rajajinagar IVth Block S.O Bengaluru KARNATAKA 560010 Rajajinagar H.O Bengaluru KARNATAKA -

Prl. District and Session Judge, Belagavi. Sri
Prl. District and Session Judge, Belagavi. Sri. Chandrashekhar Mrutyunjaya Joshi PRL. DISTRICT AND SESSIONS JUDGE BELAGAVI Cause List Date: 09-09-2020 Sr. No. Case Number Timing/Next Date Party Name Advocate 11.00 AM-02.00 PM 1 Crl.Misc. 556/2020 Manjula Iranagouda Patil age 30 B.J.Gangai (HEARING) yrs R/o Marganakoppa Tq Kittur Dt Belagavi Vs The State of Karnataka R/by PP Belagavi 2 Crl.Misc. 596/2020 Kasimsab Sultansab Nadaf Age. V.S.Karajagi (HEARING) 33 years R/o Sankeshwar ,Tal. Hukkeri, Belagavi. Vs Salma W/o Kasimsab Nadaf Age. 31 years R/o M.G Colony, Bailhongal, Belagavi. 3 SC 102/2017 State of Karnataka R/by PP SPL.PP (EVIDENCE) Belagavi. Vs Najim Nilawar @ Mahammad Najim Nilawar age 51yrs R/o Bandar Road Batkal Dt Uttar Kannada. 4 SC 129/2014 State of Karnataka Addl SP UK Public Prosecutor (OBJECTION) Karwar Dist Vs HCS/A M Aakash Vivekumar Vijaykumar Angadi/PAK/PSS/BJG/MMS/NP/ARP Upadhya age 27 yrs Ro Kaitapur Roohaniya Varanasi UP 5 SC 351/2019 The State of Karnataka R/by PP, PP (HBC) Belagavi. Vs Ibrahim Amanulla Saiyyad Age. 23 years R/o Rukmini Nagar, Belagavi. 6 Crl.Misc. 1282/2020 Suresh Ramappa Dange Age R.G. PATIL (OBJECTION) 29Yrs R/o Itanal Village, in Raibag Tq, Dist Bealgavi. Vs The State of Karnataka Through PSI Raibag P.S. R/by Learned P.P. Bealgavi. 7 Crl.Misc. 1323/2020 Basu @ Basavaraj S/o Rudrappa A.C.Dongare. (OBJECTION) Nesaragi Age 27Yrs R/o Killa Gokak Tq Gokak Dt Belagavi.