Space Shuttle Disaster
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Challenger Accident in a Rogers Commission Hearing at KSC
CHALLENGER By Arnold D. Aldrich Former Program Director, NSTS August 27, 2008 Recently, I was asked by John Shannon, the current Space Shuttle Program Manager, to comment on my experiences, best practices, and lessons learned as a former Space Shuttle program manager. This project is part of a broader knowledge capture and retention initiative being conducted by the NASA Johnson Space Center in an “oral history” format. One of the questions posed was to comment on some of the most memorable moments of my time as a Space Shuttle program manager. Without question, the top two of these were the launch of Challenger on STS‐51L on January 28, 1986, and the launch of Discovery on STS‐26 on September 29, 1988. Background The tragic launch and loss of Challenger occurred over 22 years ago. 73 seconds into flight the right hand Solid Rocket Booster (SRB) broke away from the External Tank (ET) as a result of a burn‐ through in its aft most case to case joint and the Space Shuttle vehicle disintegrated resulting in the total loss of the vehicle and crew. The events leading up to that launch are still vivid in my mind and deeply trouble me to this day, as I know they always will. This paper is not about what occurred during the countdown leading up to the launch – those facts and events were thoroughly investigated and documented by the Rogers Commission. Rather, what I can never come to closure with is how we, as a launch team, and I, as one of the leaders of that team, allowed the launch to occur. -

Toward a History of the Space Shuttle
Toward a History of the Space Shuttle An Annotated Bibliography Compiled by Roger D. Launius and Aaron K. Gillette NASA History Office Code JCH NASA Headquarters Washington, DC 20546 MONOGRAPHS IN AEROSPACE HISTORY Number 1 December 1992 PREFACE Since the idea of a reusable rocket-plane was first seriously-studied by Eugen Sänger in the 1930s, the concept has e xerted s trong i nfluence o n t he d evelopment o f human s paceflight. I n t he U nited S tates, detailed proposals for a reusable space vehicle were developed as early as the 1950s, and several projects reached the design and test stage in the 1960s. Initially, the Space Shuttle was envisioned as a fully reusable, commercial spaceplane. During the early 1970s, however, its development faced considerable obstacles, budgetary shortfalls, some congressional opposition, increasing public apathy, and design difficulties. What emerged was a smaller, semi-reusable vehicle, advertised as an economical and efficient means of space transport. Whether the Shuttle has fulfilled these goals is a topic of some controversy. Even so, the Space Shuttle has been the cornerstone of the U.S. space program, and the driving force behind much of the budget and programs of NASA for over two decades. Throughout the long history of the Space Shuttle concept, numerous books, studies, reports, and articles have been written. This selective, annotated bibliography discusses those works judged to be most essential for researchers writing scholarly studies on the Space Shuttle's history. A thematic arrangement of material concerning the Shuttle will, it is hoped, b ring clarity and simplicity to such a complex subject. -

Space Shuttle CHALLENGER Accident
National Aeronautics and Space Administration Report to the President I Actions to Implement the Recommendations of The Prazdential Commission on the Space Shuttle ChulhgmAcczdent July 14,1986 3 Washington, D.C. L DEDICATION Those of us at NASA, who have worked incessantly since that day in January when the CHALLENGER and her crew, our friends, were lost, dedicate this report to those who willfly again into space in the future. THE WHITE HOUSE WASHINGTON June 13, 1986 Dear Jim: I have completed my review of the report from the Commission on the Space Shuttle CHALLENGER Accident. I believe that a program must be undertaken to implement its recommenda- tions as soon as possible. The procedural and organizational changes suggested in the report will be essential to resuming effective and efficient Space Transportation System operations , and will be crucial in restoring U.S. space launch activities to full operational status. Specifically, I would like NASA to report back to me in 30 days on how and when the Commission's recommendations will be implemented. This report should include milestones by which progress in the implementation process can be measured. Let me emphasize, as I have so many times, that the men and women of NASA and the tasks they so ably perform are essential to the nation if we are to retain our leadership in the pursuit of technological and scientific progress. Despite misfortunes and setbacks, we are determined to press on in our space programs. Again, Jim, we turn to you for leadership. You and the NASA team have our support and our blessings to do what has to be done to make our space program eafe, reliable, and a source of pride to our nation and of benefit to all mankind. -
Spacewalk Database
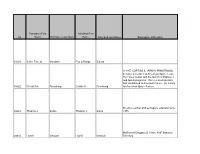
Purchaser First Inscribed First ID Name Purchaser Last Name Name Inscribed Last Name Biographic_Infomation 01558 Beth / Forrest Goodwin Ron & Margo Borrup In 1957 CURTISS S. (ARMY) ARMSTRONG became a member of America's Space Team. His career began with the launch of Explorer I and Apollo programs. His tireless dedication has contributed to America's future. He is truly 00022 Cheryl Ann Armstrong Curtiss S. Armstrong an American Space Pioneer. Science teacher and aerospace educator since 00023 Thomas J. Sarko Thomas J. Sarko 1975. McDonnell Douglas 25 Years, AMF Board of 00024 Lowell Grissom Lowell Grissom Directors Joined KSC in 1962 in the Director's Protocol Office. Responsible for the meticulous details for the arrival, lodging, and banquets for Kings, Queens and other VIP worldwide and their comprehensive tours of KSC with top KSC 00025 Major Jay M. Viehman Jay Merle Viehman Personnel briefing at each poi WWII US Army Air Force 1st Lt. 1943-1946. US Civil Service 1946-1972 Engineer. US Army Ballistic Missile Launch Operations. Redstone, Jupiter, Pershing. 1st Satellite (US), Mercury 1st Flight Saturn, Lunar Landing. Retired 1972 from 00026 Robert F. Heiser Robert F. Heiser NASA John F. Kennedy S Involved in Air Force, NASA, National and Commercial Space Programs since 1959. Commander Air Force Space Division 1983 to 1986. Director Kennedy Space Center - 1986 to 1 Jan 1992. Vice President, Lockheed Martin 00027 Gen. Forrest S. McCartney Forrest S. McCartney Launch Operations. Involved in the operations of the first 41 manned missions. Twenty years with NASA. Ten years 00028 Paul C. Donnelly Paul C. -

An Analysis of the Progress in Automation of Manned Space-Craft Test and Checkout
University of Central Florida STARS Retrospective Theses and Dissertations 1975 An Analysis of the Progress in Automation of Manned Space-craft Test and Checkout John E. Malone University of Central Florida Part of the Engineering Commons Find similar works at: https://stars.library.ucf.edu/rtd University of Central Florida Libraries http://library.ucf.edu This Masters Thesis (Open Access) is brought to you for free and open access by STARS. It has been accepted for inclusion in Retrospective Theses and Dissertations by an authorized administrator of STARS. For more information, please contact [email protected]. STARS Citation Malone, John E., "An Analysis of the Progress in Automation of Manned Space-craft Test and Checkout" (1975). Retrospective Theses and Dissertations. 164. https://stars.library.ucf.edu/rtd/164 AN .ANALYSIS OF 1HE PROGRESS IN AlJ'fG1ATION OF MANNED SP.A£ECRAFf TEST AND OiECKOUT BY JOHN E. MALONE B.S., Tuskegee Institute, 1964 RESEARCH REPORT Submitted in partial fulfillment of the requirements for the degree of Master of Science in Engineering in the Graduate Studies Program of Florida Technological University Orlando, Florida 1975 iii ABSTRACT Manned Spacecraft Programs are the largest research and develop ment tasks ever undertaken by the government o~ by private industry in the United States~ Under the direction of the National Aeronautic and Space Administration (NASA) these programs have advanced from Project Mercury ~n the early 1960's through Gemini, Apollo, including ?vbon Landing, . and Skylab Progr~ . to the present day Space Shuttle Program. With the development of each new program, there comes a growing awareness of the ever increasing complexity of tasks relating to integrated preflight test and checkout. -
A Reproduced Copy OF
A Reproduced Copy OF = (NASA-TM-X-69471) INSTITUTICNAL N74 10302 ENVIRONMENTAL IMPACT STATEMENT (SPACE SHUTTLE DEVELOPMENT AND OPERATIONS) AMENDMENT NO. 1 (NASA) --4*6 p HC $9.50 Unclas 1'S CSCL 14B G3/11 21647 Reproduced for NASA by the NASA Scientific and Technical Information Facility FFNo 672 Aug 65 August, 1973 JOHN F. KENNEDY SPACE CENTER OCT 9 - 1973 1OHN F. KENNEDY SPACE CENTEI NASA ULIBRARY CIRCULATION COPY, 7 AMENDMENT NUMBER 1 TO THE INSTITUTIONAL ENVIRONMENTAL IMPACT STATEMENT (SPACE SHUTTLE DEVELOPMENT AND OPERATIONS) SHUTTLE PROJECT OFFICE / AMENDMENT NUMBER 1 TO THE INSTITUTIONAL ENVIRONMENTAL IMPACT STATEMENT (SPACE SHUTTLE DEVELOPMENT AND OPERATIONS) Prepared by: Shuttle Project Office John F. Kennedy Space Center, NASA Kennedy Space Center, Florida 32899 // SUMMARY AMENDMENT NUMBER 1 INSTITUTIONAL ENVIRONMENTAL IMPACT STATEMENT (SPACE SHUTTLE DEVELOPMENT AND OPERATIONS) ( ) DRAFT (X) FINAL Responsible Federal Agency: National Aeronautics and Space Administration (NASA), Office of Manned Space Flight, Space Shuttle Program. a. ( X ) Administrative Action ( X ) Legislative Action b. This action proposes to establish, at John F. Kennedy Space Center (KSC), NASA, facilities for receiving, inspection, checkout, launch, recovery and refurbishment of Space Shuttle flight hardware. Many existing facilities and systems, constructed for the Apollo and Skylab programs, are capable of supporting Shuttle operations with little or no modification. Presently identified modifications to such areas as the Vehicle Assembly .Building (VAB) for Orbiter maintenance and checkout, Orbiter tank storage and space vehicle vertical integration; the Mobile Launchers (ML) and Launch Pad for adaptation to a new space vehicle configuration; and numerous minor modifications to existing shop and laboratory areas are structural in nature and generally fall within the modification and rehabilitation category. -

Space Transportation System 22 STS Elements Which Have Been Baselined 25 STS Elements Which Have Not Been Baselined 27
U. S. GElXERALACCOUNTINGOFFKE SWFSTUDY SPACETRCLNSPORTATION SYSTEM mTIOIX4.L AERONAUTICSAND SPACE ADMINISTRATION P JUNE 1974 I’ _-w--w--CONTENTS SUMMARY 1 CHAPTER 1 INTRODUCTION 15 Description 16 History 17 Status 19 Space Shuttle Responsibility 19 Restrictions on Review 20 2 THE SPACE TRANSPORATION SYSTEM COST 22' Estimated Cost of the Space Transportation System 22 STS Elements Which Have Been Baselined 25 STS Elements Which Have Not Been Baselined 27 3 STATUS OF STS ELEMENTS WITH BASELINE COST ESTIMATES 35 Space Shuttle Research, Development, Test, and Evaluation Construction of Facilities Cost Per Flight 4 SCHEDULE: 43 NASA Milestones - -__ 43 Level I Milestones 44 Level II Milestones 45 5 PERFORMANCE 47 Level I Requirements 47 Level II Requirements 48 Contractor Support of Performance Characteristics 49 6 PROCRAM MANAGEMENT Responsibilities and Authorities Performance Management -._ 7 UPPER STAGES History cost Schedule Performance APPENDIX I Space Shuttle Contract Data 63 II NASA Explanation for Changes in Shuttle Facility Est5:ates at April 15,1972, and December 13, 1973 64 ..I ABBREYIATIONS . ‘. C of F Construction of Facilities DOD Department of Defense DTMO Development, Test, and Mission Operations ET External Tank G?lO General Accounting Office JSC Lyndon B. Johnson Space Center Ksc John F. Kennedy Space Center MSFC George C. Marshall Space Flight Center NASA National Aeronautics and Space Administration OAST Office of Aeronautics and Space Technology OMSF Office of Manned Space Flight 00s Orbit to Orbit Stage R&D Research and Development RDT&E Research, Development, Test and Evaluation R&PM Research and Program Management - --__ SRI3 Solid Rocket Booster SSME Space Shuttle Main Engines STS Space Transportation System USAF United States Air Force c SUMMARY This is the first of a series of annual staff studies which will provide data on the cost, schedule, and technical performance of the Space Transportation System (STS). -

Finding Aid to the Roy D. Bridges Jr. Papers, 1957-2010
FINDING AID TO THE ROY D. BRIDGES JR. PAPERS, 1957-2010 Purdue University Libraries Virginia Kelly Karnes Archives and Special Collections Research Center 504 West State Street West Lafayette, Indiana 47907-2058 (765) 494-2839 http://www.lib.purdue.edu/spcol © 2015 Purdue University Libraries. All rights reserved. Processed by: Mary A. Sego, January 14, 2015 Descriptive Summary Creator Information Bridges, Roy D., Jr., 1943- Title Roy D. Bridges Jr. papers Collection Identifier MSA 6 Date Span 1957-2010 Abstract This collection includes documents, photographs, awards and certificates, textbooks, briefs and records, artifacts, audiovisual materials, and scrapbooks that document the life and career of astronaut and retired United States Air Force Major General Roy Bridges Jr. Included are numerous awards, drawings, and personalized photographs and mementos given to Bridges in appreciation of his service and leadership. Extent 68.90 cubic feet (24 cubic feet boxes, 2 legal mss boxes, 37 letter mss boxes, 12, ½ letter mss boxes, 6 small flat boxes, 3 medium flat and 8 large flat boxes, and 3 oversized, loose wrapped items) Finding Aid Author Mary A. Sego Languages English Repository Virginia Kelly Karnes Archives and Special Collections Research Center, Purdue University Libraries Administrative Information Location ASC and ASC-R Information: Access Collection is open for research. The collection is stored offsite; 24 hours Restrictions: notice is required to access the collection. Acquisition Donated by Roy D. Bridges Jr., 2009-2013. Information: Accession 20090409 Number: 20091111 20100104 12/2/2015 2 20100421 20100604 20100910 20110119 20110427 20110505 20110622 20120405 20130308 20130425 Preferred MSA 6, Roy D. Bridges Jr. -
A Retrospective ® Provide Power for the Orbiter’S Three Independent Hydraulic Systems
A Retrospective ® Provide power for the orbiter’s three independent hydraulic systems. Each system provides hydraulic pressure to position hydraulic actuators for: ° Thrust vector control of the main engines by gimbaling the three SSMEs ° Actuation of various control valves on the SSMEs ° Movement of the orbiter aerosurfaces (elevons, body flap, rudder/speed brake) ° Retraction of the external tank/orbiter 17-inch liquid oxygen and liquid hydrogen disconnect umbilicals within the orbiter at external tank jettison ° Main/nose landing gear deployment (system 1)/(system 1 or 2) ° Main landing gear brakes and anti-skid ° Nose wheel steering (system 1 with backup from system 2). ® During a typical flight, the APUs are started 5 minutes before lift-off and operate through the Orbital Maneuvering System-1 (OMS-1) burn when hydraulic power is no longer required. ® The APUs are basically inactive on orbit. ® One APU is run briefly the day before deorbit to support the Flight Control Surface (FCS) checkout. ® The APUs are restarted for the deorbit burn and entry. They are shut down shortly after landing. ® Circ pumps run to flow hydraulic fluid through system ® APU prestart at T - 6:15 minutes ® APU start at T - 5 minutes ® The HYD system provides hydraulic pressure to ° Throttle and steer the orbiter main engines ° Actuate the orbiter aerosurfaces ° Retract the external tank/umbilical plates ® All APUs are operated from T -5 minutes through the OMS-1. If there is no OMS-1 burn then APU shutdown comes after repositioning the main engines for orbit. ® The HYD system provides hydraulic pressure to ° Actuate the orbiter aerosurfaces ° Deploy the landing gear ° Provide braking ° Provide nosewheel steering ® At D/O - 5 minutes, one APU is started to insure that an APU is operating through the entry flight phase. -

STS-113 Shuttle Press Kit
STS-113 Shuttle Press Kit Station Crew Exchange, Port Truss Segment Installation Highlight Endeavour's Mission WWW.SHUTTLEPRESSKIT.COM Updated October 25, 2002 STS-113 Shuttle Press Kit National Aeronautics and Space Administration Table of Contents Mission Overview ..................................................................................................... 1 Timeline Overview ................................................................................................... 9 Mission Objectives ................................................................................................ 13 Mission Factoids .................................................................................................... 14 Mission Profile ....................................................................................................... 17 Crewmembers ........................................................................................................ 19 Rendezvous and Docking ..................................................................................... 45 Spacewalks STS-113 Extravehicular Activities ............................................................................ 49 Payloads Payload Overview..................................................................................................... 56 P1 Truss .................................................................................................................. 59 International Space Station S1 and P1 Truss Summary ......................................... -

The Gerard K. O'neill Collection Finding Aid
The Gerard K. O'Neill Collection Finding Aid by Tyler Love 2014 This finding aid was generated automatically on December 22, 2014 National Air and Space Museum Archives Division 14390 Air & Space Museum Parkway Chantilly, VA, 20151 Phone: 703-572-4045 [email protected] http://airandspace.si.edu/research/resources/archives Table of Contents Collection Overview......................................................................................................... 1 Administrative Information .............................................................................................. 1 Biographical Note............................................................................................................. 2 Scope and Content Note................................................................................................. 3 Arrangement..................................................................................................................... 3 Names and Subject Terms ............................................................................................. 3 Container Listing.............................................................................................................. 4 Series 1: Professional Papers, 1940s-1993............................................................. 4 Series 2: Publications & Reports, 1959-1992........................................................ 25 Series 3: Personal Papers, circa 1949-1990......................................................... 26 Series 4: Images, 1960s-1993.............................................................................. -

Payload Specialist Bio: Charles D. Walker 2/99
Payload Specialist Bio: Charles D. Walker 2/99 National Aeronautics and Space Administration Lyndon B. Johnson Space Center Houston, Texas 77058 Biographical Data NAME: CHARLES D. WALKER MDC PAYLOAD SPECIALIST PERSONAL DATA: Born in Bedford, Indiana, August 29, 1948. Married to the former Susan Y. Flowers, of Joplin, Missouri. They have one daughter and one granddaughter. Recreational interests include photography, running, hiking, scuba diving, reading, collecting books on Space, and bonsai. His mother, Donna Lake Walker, resides in Bedford; his father is deceased. EDUCATION: Graduated from Bedford High School, Bedford, Indiana, in 1966; received a bachelor of science degree in aeronautical and astronautical engineering from Purdue University in 1971. SPECIAL HONORS: U.S. Patent No. 4,394,246, Electrophoresis Apparatus with Flow Control, issued 19 July 1983; NASA Space Flight Medal (1984, and twice in 1985); Sagamore of the Wabash, State of Indiana (November 1984); Doctor of Science, honoris causa, St. Louis College of Pharmacy (1985); Aerospace Laurels Award, Aviation Week and Space Technology Magazine (1985); Lindbergh Award, American Institute of Aeronautics and Astronautics - St. Louis Section (1986); NASA Group Achievement Award, as consultant to the 1987-88 Space Station Operations Task Force; Engineering Astronaut Alumnus Award, Purdue University Schools of Engineering (September 1989); Kentucky Colonel, Commonwealth of Kentucky (May 1990). EXPERIENCE: Following graduation from Purdue University he worked as a civil engineering technician, land acquisition specialist and forest firefighter for the U.S. Forest Service. Subsequently he was a design engineer with the Bendix Aerospace Company where he worked on aerodynamic analysis, missile subsystem design, and flight testing. He also was employed as project engineer with the Naval Sea Systems Command with responsibility for computer-controlled manufacturing systems.