Traditional Japanese Medicine Daikenchuto Improves Functional Constipation in Poststroke Patients
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

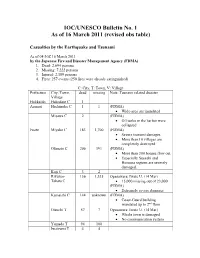
Map Indicating Locations of Activities by Rescue Teams from Foreign Countries/Territories International Organizations, Etc
Map Indicating Locations of Activities by Rescue Teams from Foreign Countries/Territories International Organizations, etc. [as of March 28th] Rescue Team Operation by countries Republic of Korea(3/14~3/23) 107 Rescue Workers, 2 Search Dogs Sendai, MIYAGI Singapore(3/13~3/15) 5 Rescue Workers, 5 Search Dog Soma, FUKUSHIMA Germany(3/14~3/15) 41 Rescue Workers, 3 Search Dogs Minami Sanriku, MIYAGI Switzerland(3/14~3/16) 27 Rescue Workers, 9 Search Dogs Minami Sanriku, MIYAGI USA(3/15~3/19) 144 Rescue Workers(incl. Search Dogs) AOMORI Hachinohe Ofunato, Kamaishi, IWATE, Kakuda, MIYAGI China(3/14~3/20) 15 Rescue Workers Ofunato, IWATE UK(3/15~3/17) 77 Rescue Workers(including 8 journalists), 2 Search Dogs Ofunato, Kamaishi, IWATE, Kakuda, MIYAGI Mexico(3/15~3/17) 12 Rescue Workers, 6 Search Dogs Natori, MIYAGI Australia(3/16~3/19) 75 Rescue Workers, 2 Search Dogs Minami Sanriku, MIYAGI IWATE New zealand(3/16~3/18) 52 Rescue Workers Minami Sanriku, MIYAGI France(3/16~3/23) 134 Rescue Workers(incl. 11Monacans) After operation in Natori, MIYAGI, They had moved to Hachinohe, AOMORI Kamaishi Taiwan(3/16~3/18) 28 Rescue Workers Sendai, MIYAGI Russia(3/16~3/18) Ofunato 75 First Rescue Workers, 80 Second Rescue Workers Ishinomaki, MIYAGI Mongolia(3/17~3/19) kesennuma 12 Rescue Workers Sendai, Natori, Iwanuma, MIYAGI Minami Sanriku Turkey(3/20~) MIYAGI 32 Rescue Workers Tagajo, Ishinomaki, Nanagahama, MIYAGI Ishinomaki Indonesia(3/19~) 11 Rescue Workers, staff, 4 Medical staff Kesennuma, Shiogama, Ishinomaki, MIYAGI Shiogama South Africa(3/19~3/25) -

Matsushima Bay As an Early Holocene Coastal Mega-Landslide, Northeast Japan
Matsushima Bay as an Early Holocene coastal mega-landslide, Northeast Japan Shuichi Hasegawa (Kagawa University, Japan) Timihiro Sawada (Sawa Soft Science, Japan) Ranjan Kumar Dahal (Kagawa University, Japan and Tribhuvan University, Nepal) Atsuko Nonomura (Kagawa University, Japan) Minoru Yamanaka (Kagawa University, Japan) Abstract. Matsushima, a group of island at Matsushima Bay visited both Matsushima and Kisakata. He composed three in Miyagi Prefecture, northeast Japan, is one of the three haiku poems for Kisakata, but he could not express his famous scenic spots of Japan. It is composed of more than excitement in a haiku poem for Matsushima. 200 islands in Matsushima Bay and the islands just out into Matsushima and Matsushima Bay have long been the sea. Topographically Matsushima Bay suddenly breaks considered as a typical submerged coast, but they are inferred the gently concaved coastline from Sendai Bay to Ishinomaki to have been formed by a coastal mega-landslide in middle Bay. Matsushima and Matsushima Bay have been considered Holocene age from geological and topographical inferences. as a typical submerged coast, but they are inferred to have been formed by a coastal mega-landslide in middle Holocene age from geological and topographical evidences. Keywords. Mega-landslide, Holocene, Jomon transgression, Active fault, topography 1. Introduction Mega-landslides due to volcanic activities and earthquakes have caused severe damage to the surrounding areas. Sector collapse of volcanoes is one of the most destructive landslides. Debris avalanche deposits from a sector collapse generally form strange topography punctuated by hundreds of small hills, ridges and closed depressions. The 1792 Mayuyama sector collapse of Unzen volcano in Kyushu, southern Japan, caused debris avalanche which flowed through ancient Shimabara City and entered the sea. -

Strategies of the 77 Bank, Ltd Growth Strategy
Strategies of The 77 Bank, Ltd Growth Strategy Best Consulting Bank Human Resource Development In order to become a bank that is truly supported by its customers and to establish a solid management base for the future, we have set the image of the bank we aspire to become as the following, and actively trained specialist resources. Interview 01 “Best Consulting Bank” that responds to customersʼ needs by offering the optimum solutions Striving to solve the issues of quality assurance Corporate Support Department and manpower shortage on the front line of manufacturing. Kei Akama I was assigned to Tohoku Electronics Industry Co., Ltd. with Tohoku Electronics Industry has about 1,000 employees in the headquarters in Ishinomaki City, Miyagi Prefecture for one year entire group, I was forced to be keenly aware of the issue of the under the Local Company Trainee program that started in 2018. shortage of manpower at the manufacturing front line. I believe I was assigned to the Quality Assurance Department, where I that these valuable experiences as a trainee at a local company dealt with automobile manufacturers and interacted with manu- can be utilized in my current work. I am currently working in the facturing sites to ensure the quality of automobile-related parts. Corporate Support Office, providing support mainly to custom- I was interested in the manufacturing industry, including ers in the fishery processing industry in the coastal areas of the automobiles and machinery, and I thought I had acquired some prefecture that are still on the road to recovery from the Great prior knowledge before I was transferred to the company, but I East Japan Earthquake. -

Historical Fish Specimens Collected from the Tohoku District by the Saito Ho-On Kai Museum of Natural History
Bull. Natl. Mus. Nat. Sci., Ser. A, 35(1), pp. 9–54, March 22, 2009 Historical Fish Specimens Collected from the Tohoku District by the Saito Ho-on Kai Museum of Natural History Keiichi Matsuura1, Gento Shinohara2 and Masanori Nakae1 1 Collection Center, National Museum of Nature and Science, 3–23–1 Hyakunin-cho, Shinjuku-ku, Tokyo, 169–0073 Japan E-mail: [email protected]; [email protected] 2 Department of Zoology, National Museum of Nature and Science, 3–23–1 Hyakunin-cho, Shinjuku-ku, Tokyo, 169–0073 Japan E-mail: [email protected] Abstract The fish collection of the Saito Ho-on Kai Museum of Natural History was transferred to the National Museum of Nature and Science, Tokyo in February 2006. Ninety percent of the fish collection contains specimens collected from the Tohoku District during the period from 1930 to 1933 when natural environments of Japan were in good condition for various groups of fishes. The fish specimens from the Tohoku District were classified into 361 species/subspecies of 273 genera belonging to 131 families of 31 orders. A list of the species is shown with remarks on distribution. Key words: Fish specimens, Saito Ho-on Kai Museum, Tohoku District, inventory. stead of natural sicence. The museum has tried to Introduction keep its activity at the level before the war, but it The Saito Ho-on Kai Museum was established failed to do so because of financial difficulties. In in November 1933 in Sendai City, Miyagi Pre- 2005, the Saito Ho-on Kai Museum of Natural fecture, Japan. -

2016 Economic Census for Business Activity (Definitive Report) Tabulations Across Industries Summary of Census Results
2016 Economic Census for Business Activity (Definitive Report) Tabulations across Industries Summary of Census Results I Overview ..................................................................................................................................... 1 II Situations of Number of Enterprises, etc., Sales, and Added Value .......................................... 3 1. Number of Enterprises, etc., Sales, and Added Value ........................................................... 3 2. Added Value Ratio ................................................................................................................. 13 3. Sales by Business Activity ..................................................................................................... 14 4. Capital Investment ................................................................................................................. 18 5. Electronic Commerce (e-commerce) ..................................................................................... 24 6. Situation of Added Value by Prefecture ................................................................................ 27 III Situations of Number of Establishments and Number of Persons Engaged ............................. 29 1. Number of Establishments and Number of Persons Engaged by Industry Division.............. 29 2. Number of Persons Engaged by Status in Employment ........................................................ 33 3. Number of Establishments and Number of Persons Engaged by Size of Persons Engaged -

Feel More Alive / in Higashi-Matsushima
Tohoku Shinkansen Shinkansen Tohoku Tohoku 4 Ishinomaki city Tsukidate IC JR Rikuu-East Line 47 45 Furukawa IC 108 JR Ishinomaki Line Sanriku Expressway Furukawa Misato Town Tohoku Expressway Naruse Ishinomaki Onagawa Oku-Matsushima IC JR Senseki Line Tomiya JCT Ishinomaki port IC JR Senzan Line Rifu JCT Sendai Higashi-Matsushima City Sendai Minami IC Higashi- 4 Wakabayashi JCT Matsushima City Sanriku Expressway Murata JCT Rikuzen-Akai Station Yamoto IC Higashi-Yamoto Station To Ishinomaki Higashi-Matsushima City Hall 45 Yamoto station Naruse Oku-Matsushima IC Japan Air Self-Defense Force, Matsushima Air Base Naruse JR Senseki Line River your Higashi-Matsushima guidebook! Discovery Center Higashi-Matsushima City Hall, Naruse Office Kazuma station Higashi-Matsushima Tourist Association Yamoto Seaside Park Rikuzen-Ono Station Town of Matsushima Yoshida River To Matsushima・ Nobiru Station Sendai Rikuzen-Otsuka Station Higashimatsushima City Great East Japan Earthquake Recovery Memorial Park Tona Station Ishinomaki Bay Oku-Matsushima Nobiru Beach Lane Hotel Oku-Matsushima Clubhouse Matsushima Bay KIBOTCHA Oku-Matsushima Pleasure Boat Information Center (in Aomina) Otakamori Satohama The Historical Museum of Jomon Village, Miyato Oku-Matsushima Island Murohama Oku-Matsushima Experience Network Ohama Sagakei Gorge Feel More Alive / Tsukihama in Higashi-Matsushima Transportation Guide Sendai station Tohoku Shinkansen Tokyo JR Senseki-Tohoku Line about 95 minutes about 40 minutes To the land of whispering winds and blue seas JR Senseki Line Matsushima -

Miyagi Prefecture Is Blessed with an Abundance of Natural Beauty and Numerous Historic Sites. Its Capital, Sendai, Boasts a Popu
MIYAGI ACCESS & DATA Obihiro Shin chitose Domestic and International Air Routes Tomakomai Railway Routes Oshamanbe in the Tohoku Region Muroran Shinkansen (bullet train) Local train Shin Hakodate Sapporo (New Chitose) Ōminato Miyagi Prefecture is blessed with an abundance of natural beauty and Beijing Dalian numerous historic sites. Its capital, Sendai, boasts a population of over a million people and is Sendai仙台空港 Sendai Airport Seoul Airport Shin- filled with vitality and passion. Miyagi’s major attractions are introduced here. Komatsu Aomori Aomori Narita Izumo Hirosaki Nagoya(Chubu) Fukuoka Hiroshima Hachinohe Osaka(Itami) Shanghai Ōdate Osaka(kansai) Kuji Kobe Okinawa(Naha) Oga Taipei kansen Akita Morioka Honolulu Akita Shin Miyako Ōmagari Hanamaki Kamaishi Yokote Kitakami Guam Bangkok to the port of Hokkaido Sakata Ichinoseki (Tomakomai) Shinjō Naruko Yamagata Shinkansen Ishinomaki Matsushima International Murakami Yamagata Sendai Port of Sendai Domestic Approx. ShiroishiZaō Niigata Yonezawa 90minutes Fukushima (fastest train) from Tokyo to Sendai Aizu- Tohoku on the Tohoku wakamatsu Shinkansen Shinkansen Nagaoka Kōriyama Kashiwazaki to the port of Nagoya Sendai's Climate Naoetsu Echigo Iwaki (℃)( F) yuzawa (mm) 30 120 Joetsu Shinkansen Nikko Precipitation 200 Temperature Nagano Utsunomiya Shinkansen Maebashi 20 90 Mito Takasaki 100 10 60 Omiya Tokyo 0 30 Chiba 0 1 2 3 4 5 6 7 8 9 10 11 12 Publication Date : December 2019 Publisher : Asia Promotion Division, Miyagi Prefectural Government Address : 3-8-1 Honcho, Aoba-ku, Sendai, Miyagi -
IOC UNESCO Bulletin No 1
IOC/UNESCO Bulletin No. 1 As of 16 March 2011 (revised obs table) Casualties by the Earthquake and Tsunami As of 04:30Z 16 March 2011 by the Japanese Fire and Disaster Management Agency (FDMA) 1. Dead: 2,694 persons 2. Missing: 7,222 persons 3. Injured: 2,189 persons 4. Fires: 257 events (250 fires were already extinguished) C: City, T: Town, V: Village Prefecture City, Town, dead missing Note: Tsunami related disaster Village Hokkaido Hakodate C 1 Aomori Hachinohe C 1 1 (FDMA) • Wide-area are inundated Misawa C 2 (FDMA) • Oil tanks in the harbor were collapsed Iwate Miyako C 183 1,700 (FDMA) • Severe tsunami damages • More than 10 villages are completely destroyed Ofunato C 206 191 (FDMA) • More than 300 houses flow out • Especially Suesaki and Hosoura regions are severely damaged. Kuji C 3 2 Rikuzen- 136 1,535 Ogasawara; Iwate U. (14 Mar) Takata C • 15,000 missing out of 23,000 (FDMA) • Extremely severe damages Kamaishi C 144 unknown (FDMA) • Coast-Guard building inundated up to 2nd floor Otsuchi T 57 7 Ogasawara; Iwate U. (14 Mar) • Whole town is damaged • No communication system Yamada T 94 100 Iwaizumi T 4 4 Tanohata V 11 28 (FDMA) • 249 houses flow out Fudai V 5 (FDMA) • Tanabe and Horiuchi fishing ports are severely damaged. Noda V 26 20 Youno T (FDMA) • 20 houses flow out • Many fishing boats flow out • JR train bridge collapsed Miyagi Sendai C 13 Koshimura; Tohoku U (12 Mar) • Near Sendai air-port: inundated area is up-to 3- 4km from coast (depth: about 1 m) • Difficult to go to coastal area due to inundated water • Wakabayashi-ku: severely damaged. -

Globally Important Agricultural Heritage Systems (GIAHS) Application
Globally Important Agricultural Heritage Systems (GIAHS) Application SUMMARY INFORMATION Name/Title of the Agricultural Heritage System: Osaki Kōdo‟s Traditional Water Management System for Sustainable Paddy Agriculture Requesting Agency: Osaki Region, Miyagi Prefecture (Osaki City, Shikama Town, Kami Town, Wakuya Town, Misato Town (one city, four towns) Requesting Organization: Osaki Region Committee for the Promotion of Globally Important Agricultural Heritage Systems Members of Organization: Osaki City, Shikama Town, Kami Town, Wakuya Town, Misato Town Miyagi Prefecture Furukawa Agricultural Cooperative Association, Kami Yotsuba Agricultural Cooperative Association, Iwadeyama Agricultural Cooperative Association, Midorino Agricultural Cooperative Association, Osaki Region Water Management Council NPO Ecopal Kejonuma, NPO Kabukuri Numakko Club, NPO Society for Shinaimotsugo Conservation , NPO Tambo, Japanese Association for Wild Geese Protection Tohoku University, Miyagi University of Education, Miyagi University, Chuo University Responsible Ministry (for the Government): Ministry of Agriculture, Forestry and Fisheries The geographical coordinates are: North latitude 38°26’18”~38°55’25” and east longitude 140°42’2”~141°7’43” Accessibility of the Site to Capital City of Major Cities ○Prefectural Capital: Sendai City (closest station: JR Sendai Station) ○Access to Prefectural Capital: ・by rail (Tokyo – Sendai) JR Tohoku Super Express (Shinkansen): approximately 2 hours ※Access to requesting area: ・by rail (closest station: JR Furukawa -

To View Dr. Daniel Aldrich Slides From
Building, Repairing, and Connecting Social Support Networks Across Boundaries Daniel P. Aldrich [email protected] Twitter @danielpaldrich Trust, neighbors, networks 10 minute breakout session • Please work with your group to try to map the networks you and your organization work with • Are these ties bonding, bridging, or linking? • Can you remember times that these times have activated or times when you weren’t able to effectively coordinate because of a lack of ties? Exit vs. Voice Collective Action Informal Insurance Evacuation Survival Survival not well correlated with height .15 Onagawa Rikuzentakata Otsuchi .1 Rifu Natori Kamaishi Yamamoto Yamada Minamisanriku Namie Tomioka .05 Minamisoma Soma Futaba Okuma HigashimatsushimaIshinomaki Kesennuma Miyako Iwanuma Shinchi Ofunato Watari Naraha Tanohata Tagajo Iwaki Noda Shichigahama Iwaizumi Shiogama Hirono 0 MoriokaHanamakiKitakamiTonoIchinosekiNinoheHachimantaiOshuShizukuishiKuzumakiIwateTakizawaShiwaYahabaNishiwagaKanegasakiHiraizumiFujisawaSumitaKarumaiKunoheIchinoheAobaIzumiShiroishiKakudaTomeKuriharaOsakiZaoShichikashukuOgawaraMurataShibataKawasakiMarumoriTaiwaOsatoTomiyaOhiraShikamaKamiWakuyaMisatoFukushimaAizuwakamatsuKoriyamaShirakawaSukagawaKitakataNihonmatsuTamuraDateMotomiyaKoriKunimiKawamataOtamaKagamiishiTeneiShimogoHinoemataTadamiMinamiaizuKitashiobaraNishiaizuBandaiInawashiroAizubangeYugawaYanaizuMishimaKaneyamaShowaAizumisatoNishigoIzumizakiNakajimaYabukiTanaguraYamatsuriHanawaSamegawaIshikawaTamakawaHirataAsakawaFurudonoMiharuOnoKawauchiKatsuraoIitate choTaihakuMatsushima -

East Japan Earthquake and Tsunami
East Japan Earthquake International Environment and Disaster Management UNESCO Bangkok Laboratory Education for Sustainable Development Graduate School of Global Environmental Studies 920 Sukhumvit Rd, Prakanong, Klongtoey and Tsunami KYOTO UNIVERSITY Bangkok 10110, Thailand Yoshida Honmachi, Sakyo-ku, Kyoto 606-8501, JAPAN Tel/ Fax: 81-75-753-5708 Tel. +6623910577 ext 221. Fax. +6623910866 Key Lessons for the Education Sector Web: http://www.iedm.ges.kyoto-u.ac.jp/ http://www.unesco.org/bangkok Key Lessons and Issues New Role of of Schools Structure, Function and Human Effectiveness School and E-HFA Tasks Location, Educational Resources of Disaster Multi- stakeholder Layout Continuity and Training Education Dialogue of Schools Tasks1 Tasks2 E-HFA1 Tasks3 Tasks4 Tasks5 E-HFA E-HFA2 Tasks6 Tasks7 Tasks8 E-HFA3 Tasks9 Tasks10 Tasks11 Tasks12 E-HFA4 E-HFA1: Tasks13 Tasks14 Tasks15 E-HFA5 Task1~4 Tasks16 Low Performance, Need improvements Moderate Performance High Performance an of an Disclaimer: The designations employed and the presentation of material throughout this publication do not imply the expression of any opinion whatsoever on the part of UNESCO Bangkok concerning the legal status of any country, territory, city or area or of its authorities, or the delimitation of its frontiers or boundaries. The authors are responsible for the choice and the presentation of the facts contained in this book and for the opinions expressed therein, which are not necessarily those of UNESCO Bangkok and do not commit the Organization. Authors: Rajib Shaw Yukiko Takeuchi Kyoto University, Japan Contacts: Rajib Shaw Associate Professor Graduate School of Global Environmental Studies KYOTO UNIVERSITY Yoshida Honmachi, Sakyo-ku, Kyoto 606-8501, JAPAN Tel/ Fax: 81-75-753-5708 Web: http://www.iedm.ges.kyoto-u.ac.jp/ E-mail: [email protected] East Japan Earthquake and Tsunami Key Lessons in the Education Sector Contents 1. -

< 3 Trails Version >
Guide Book Special hikes through magnificent landscapes and hot springs let you explore the region’s distinct history and culture with your five senses. Come experience this healing journey, Miyagi Olle. At long last, a healing journey through magnificent landscapes and rich history < 3 Trails Version > Issue Date: First Edition September 2019 Miyagi Olle Trail, a Healing Journey Matsushima, its picturesque bay dotted with islands large and small, is the start of the journey to Miyagi Prefecture, a region rich with natural beauty. In the west is a range of mountains stretching from Mt. Zao to Mt. Funagata to Mt. Kurikoma. In the center, rice fields stretch out as far as the eye can see, with a beauty that changes from season to sea- son, and is ideal for experiencing traditional culture. The coastal area was badly damaged by tsunami caused by the 2011 Great East Japan Earthquake, but the coastal and mountain trails are being restored to their former beauty. Disaster became the opportunity which sparked the creation of the Miyagi Olle Trail, and with assistance from the Jeju Olle Foundation, in 2018 the Miyagi Olle Trail was created as a sister trail to those in Jeju (Korea), Kyushu and Mongolia. Miyagi Olle Trail has diverse routes, ranging from trails which travel by the endless stretch of the Pacific Ocean, to the natural richness of forested trails, to country roads with opportunities to meet local res- idents. While there are similarities to the Jeju Olle and Kyushu Olle, Miyagi has its own unique features. Olle trails are characterized by people coexisting with nature, and this is firmly embedded in Miyagi Olle as well.