POLIO NSW INC Formerly Post-Polio Network (NSW) Inc
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Slim Dusty the Very Best of Slim Dusty Mp3, Flac, Wma
Slim Dusty The Very Best Of Slim Dusty mp3, flac, wma DOWNLOAD LINKS (Clickable) Genre: Folk, World, & Country Album: The Very Best Of Slim Dusty Country: Australia Released: 1998 MP3 version RAR size: 1773 mb FLAC version RAR size: 1551 mb WMA version RAR size: 1515 mb Rating: 4.9 Votes: 780 Other Formats: MP2 AA MOD AIFF RA MP1 MPC Tracklist 1 –Slim Dusty Pub With No Beer 2:55 2 –Slim Dusty Lights On The Hill 3:02 3 –Slim Dusty The Biggest Disappointment 3:00 4 –Slim Dusty Three Rivers Hotel 3:23 5 –Slim Dusty Ringer From The Top End 2:27 6 –Slim Dusty Where Country Is 3:47 7 –Slim Dusty Leave Him In The Long Yard 2:50 8 –Slim Dusty Plains Of Peppimenarti 3:10 9 –Slim Dusty Duncan 2:34 10 –Slim Dusty Charleville 3:00 11 –Slim Dusty Indian Pacific 3:25 12 –Slim Dusty Sweeney (Live) 3:12 13 –Slim Dusty G'day G'day 3:08 14 –Slim Dusty Walk A Country Mile 2:43 15 –Slim Dusty When The Rain Tumbles Down In July 2:37 16 –Slim Dusty I'm Going Back Again To Yarrawonga (Live) 1:32 –Slim Dusty With Joy McKean And Anne 17 Old Time Country Halls 2:32 Kirkpatrick 18 –Slim Dusty Camooweal 4:11 19 –Slim Dusty We've Done Us Proud 4:25 20 –Slim Dusty Country Revival 2:17 21 –Slim Dusty Cunnamulla Feller 2:09 22 –Slim Dusty By A Fire Of Gidgee Coal 2:57 23 –Slim Dusty Losin' My Blues Tonight 3:20 24 –Slim Dusty Featuring Rolf Harris Wobbly Boat 3:00 Companies, etc. -

Politics and Country Music Merry Christmas and Happy New Year!
Politics and Country Music Just a Thought ‘Thanks KFC for your sponsorship’ From Have you ever experienced bribery? Of course you have! Bill Northcott! ‘We Like it Like Do you truly believe what politicians say? Of course you don’t! That!’ ‘Push’ is more important than ‘Pull’ Well you can believe this if you like. It contains bribery and especially if you’re going through a promises. revolving door. The life and career of country music legend and bush icon, Slim Dusty , mentioned many times in previous Gawler Country Music Club Newsletters, will be celebrated in a new development in Aunty Kay’s Kempsey, NSW, ‘….if the Coalition wins government.’ Question Time How’s that for genuine political generosity and sincerity………. Q. There is a train one kilometre long, Sorry but ‘Bullshit!’ travelling at a rate of one kilometre per minute Venue: Munno Para Bowling & Recreation Club Monte Carlo Winners through a tunnel which is 1 kilometre long. Cnr. Curtis & Main North Roads Munno Para Deputy Prime Minister, Mark Vaile , and local Nationals MP, Luke Hartsuyker, recently announced a $6 million pledge at a Well done Jennifer and Rob. You obviously never won a Christmas Turkey! How long would it take for the train to pass special fund-raising concert in Kempsey where members of the completely through the tunnel? late Slim Dusty 's family performed. "For those of us who live in regional Australia in particular, but Jeanette’s Four in a Row also for those in the cities, Slim Dusty was the quintessential When a country artist has four hit records in a row Aussie," Mr Vaile said. -

SACCM Gig Guide
Keith Keep it Urban Country Christmas Love Pain and the whole Gift Ideas crazy thing The Slim Dusty Movie (Australia Limited Edition) 2DVD/2CD Price: $31.95 Price: $49.95 Love, Pain & the whole crazy thing is the Released November 5 2006 , starring Slim new album from Grammy Award winner and Dusty, Joy McKean, Anne Kirkpatrick with John Blake as the three time Country Music Association (CMA) Male Artist of the Year, Keith young Slim Dusty. Urban. The follow up to double platinum Be Here , this is one of the most anticipated Journey back to an Australia of country showgrounds, back- releases of 2006 and showcases Urban’s breaking roads, irrepressible bush larrikins, long trains and ever- consummate songwriting and vocal talents, rolling trucks, paddocks of ripened wheat and kegs of amber fluid. as well as his searing guitar work. Welcome to the world of SLIM DUSTY. Filmed over 20,000 SACCM kilometres in a variety of frontier towns, truck stops, rodeo arenas It includes “Once In A Lifetime,” the and concert halls; THE SLIM DUSTY MOVIE is a film album’s first single, which upon its release experience like no other! Combining nostalgic historical in the US became the highest debuting single recreations, exhilarating concert scenes and on-the-road candid Gig Guide since the inception of the Billboard Chart. footage with the man himself, this big screen adventure spans 50 Keith is quoted as saying “I think it’s the years in the life of a remarkable performer who was known the sound of being happy and extremely excited world over as "The Man Who Is Australia". -

Slim Dusty Movie Music Credits
Music Production Rod Coe (Cast, singing) Slim Dusty Joy McKean Anne Kirkpatrick and the Travelling Country Band David Kirkpatrick Gordon Parsons Buck Taylor (Tail credits) The Travelling Country Band Lead Guitar Mick Reid Fiddle and Mandolin Mike Kerin Drums Alan Hockley Banjo and Dobro Ian Simpson Pedal Steel Michel Rose Bass Guitar Bill Graham Location Sound Supervisor Paul Clark Boom Operator/ Recordist Steve Haggerty AAV Technical Supervision Steve Pyle Music Engineer Scott Heming Sound Assistant Chris Piper Concert Sound Mixer Clive Jones Featured Music Where Country is Barry "Morchi" Moyses The Band Played on Traditional Song for the Aussies Slim Dusty Aristocrat Tex Morton Simmo's Tune Ian Simpson Old Sunlander Van Joy McKean Anne Kirkpatrick G. Paige Losin' my Blues Tonight Slim Dusty Wind up Gramophone Joy McKean Trouble Joy McKean Walk a Country Mile Joy McKean Old Feller Joy McKean Drownin' my Blues Slim Dusty My Final Song Slim Dusty When the Rain Tumbles down in July Slim Dusty Camoweal "Mack" Cormack So many Ballads to Play Slim Dusty The Man from the Northland Buck Taylor Old Time Country Halls Slim Dusty Biggest Disappointment Joy McKean Lights on the Hill Joy McKean Gymkhana Yodel Joy McKean Stay Away from me Slim Dusty Keep the Love Light Shining Joy McKean Country Revival Slim Dusty The Isa Rodeo Slim Dusty Stan Coster Rough Riders Slim Dusty A. E. Brooks Cunnamulla Feller Stan Coster Isa R. Ryan Plains of Peppimenarti Slim Dusty How will I go with him Mate "Mack" Cormack Just Rollin' Slim Dusty Pushin' Time Slim Dusty A. E. -

Gig Guide Hit
Australia’s First Ever Out and About with Number One Hit Keith Urban Australia’s first ever Number 1 Hit Single has Love, Pain & The Whole Crazy World Tour newly celebrated its comes to Adelaide. First Half Century . April 2007 marked 50 Don’t miss – Keith Urban on Sun 20 May years since the recording when he appears at Adelaide Entertainment of Australia’s first ever Centre. hit single ‘A Pub With No Beer’. This iconic song recorded by Slim Dusty and written by Gordon Parsons , was not only the first ever #1 hit record by an Australian artist , but also Australia’s first ever international Gig Guide hit. Recorded back in April 1957 in the EMI 301 studios, Slim’s best mate Gordon Parsons , known as ‘The Yodelling Bushman’ lent a hand when Slim fell short of songs to record. The song stayed in the charts for over six months and Acknowledgement to sales climbed to unprecedented sales for an Aussie http://www.saccm.com/gigguide/gigguide.htm artist. See www.chuggentertainment.com where Keith speaks Gordon Parsons wife Jeanette indicated that frankly on video about what he has experienced in his Gordon’s song was about a fictitious little country personal life since last October. pub. But we all know the pub is real ….. Don’t we? He has obviously revalued his life-style and good luck In further praise to the song sung by her beloved to this superstar performer . husband, Slim’s wife, Joy McKean , says… “It’s an amazing feat for any song to live so long in the "I have so much at home to be thankful for; everyone consciousness of people and remain so popular for who has supported me through the years, the warm so many years that it becomes almost an anthem, embrace that we've received there," but that is what ‘the Pub’ has done. -
Great Aussie Toaster
SLIM DUSTY 10. Aug/Sep 2014 AND JOY MCKEAN RRP $5.95 ‘We lived in caravans 17 years’ ESSENTIAL Great Aussie BUYING GUIDE Toaster Should you buy old or new? Remembering the 1950s icon and its demise In print and online timetoroam.com.au AUSTRALIA’S NEW FAVOURITE CARAVAN AND CAMPING MAGAZINE Issue 10 Aug/Sep 2014 1 BRISBANE 104KM Tweed Heads BRUNSWICK HEADS BYRON BAY LENNOX HEAD BALLINA EVANS HEAD Grafton RED ROCK CORINDI BEACH MOONEE BEACH COFFS HARBOUR MYLESTOM URUNGA HUNGRY HEAD NAMBUCCA HEADS SCOTTS HEAD Port Macquarie BONNY HILLS NORTH HAVEN Taree TUNCURRY FORSTER SEAL ROCKS HAWKS NEST Newcastle SYDNEY 160KM upfront | contents 10 AUG/SEP 2014 upfront 07 / REGO RIP OFF NSW considers changes to soaring caravan fees 08 / ANNEXE GAS BOMBSHELL Red tape forces job cuts 08 / WICKED SLAP DOWN Lewd camper company finally bows to pressure features 18 / CARAVAN CONQUERS THE MURRAY Plonk the floating van completes epic journey RISE AND FALL OF THE TOASTER 20 / RISE AND FALL OF THE TOASTER Heavy metal favourite from the 50s riding high again 28 / NEW OR SECOND HAND? on the roam Help to make the right caravan purchase JAYCO 48 / PEOPLE AND PLACES CONQUEST The VIC caravan industry’s night of nights, 31 / OUR RENO RESCUE plus show highlights Big changes ahead for Roam’s 1969 Viscount 38 52 / MAGNIFICENT MACLEAY tried+tested Coastal gems, land of legends 52 54 / FLAVOURS Magnificent 32 / CARAVAN REVIEW Thai green curry is seafood heaven Macleay Atlantic Caravans New Generation 56 / CELEBRITY CAMPER 38 / MOTORHOME REVIEW Joy McKean, Grand Lady of Music, Caravan Queen Jayco Conquest 59 / MY TOP FIVE 42 / CAMPER REVIEW ON THE COVER Gerry Ryan reveals plans to hit the road in 2015 Freedom Offroad Beyond Carapark caravans, Broken Hill NSW 64 / WHAT’S ON Photo by Phillip Terry Australia’s best guide to regional events this Spring 4 timetoroam.com.au Discover the seven wonders of the Tweed Tweed Coast Holiday Camping Parks has seven exciting destinations that will keep the kids happy. -

Sing! 1975 – 2014 Song Index
Sing! 1975 – 2014 song index Song Title Composer/s Publication Year/s First line of song 24 Robbers Peter Butler 1993 Not last night but the night before ... 59th St. Bridge Song [Feelin' Groovy], The Paul Simon 1977, 1985 Slow down, you move too fast, you got to make the morning last … A Beautiful Morning Felix Cavaliere & Eddie Brigati 2010 It's a beautiful morning… A Canine Christmas Concerto Traditional/May Kay Beall 2009 On the first day of Christmas my true love gave to me… A Long Straight Line G Porter & T Curtan 2006 Jack put down his lister shears to join the welders and engineers A New Day is Dawning James Masden 2012 The first rays of sun touch the ocean, the golden rays of sun touch the sea. A Wallaby in My Garden Matthew Hindson 2007 There's a wallaby in my garden… A Whole New World (Aladdin's Theme) Words by Tim Rice & music by Alan Menken 2006 I can show you the world. A Wombat on a Surfboard Louise Perdana 2014 I was sitting on the beach one day when I saw a funny figure heading my way. A.E.I.O.U. Brian Fitzgerald, additional words by Lorraine Milne 1990 I can't make my mind up- I don't know what to do. Aba Daba Honeymoon Arthur Fields & Walter Donaldson 2000 "Aba daba ... -" said the chimpie to the monk. ABC Freddie Perren, Alphonso Mizell, Berry Gordy & Deke Richards 2003 You went to school to learn girl, things you never, never knew before. Abiyoyo Traditional Bantu 1994 Abiyoyo .. -
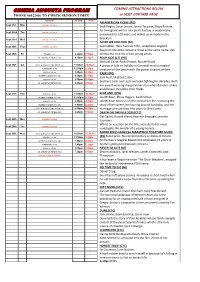
CINEMA AUGUSTA PROGRAM COMING ATTRACTIONS BELOW PHONE 86422466 to CHECK SESSION TIMES Or VISIT OUR WEB PAGE
CINEMA AUGUSTA PROGRAM COMING ATTRACTIONS BELOW PHONE 86422466 TO CHECK SESSION TIMES or VISIT OUR WEB PAGE MOVIE START END AN AMERICAN PICKLE (PG) Sept 21st Mon CINEMA CLOSED Seth Rogen, Sarah Snook, Jorma Taccone, Maya Erskine. An immigrant worker at a pickle factory is accidentally Sept 22nd Tue CINEMA CLOSED preserved for 100 years and wakes up in modern day Sept 23rd Wed CINEMA CLOSED Brooklyn. AFTER WE COLLIDED (M) Sept 24th Thur CINEMA CLOSED Selma Blair, Hero Fiennes Tiffin, Josephine Langford. Based on the 2014 romance novel of the same name, this Sept 25th Fri TROLLS (G) 6.20pm 7.50pm follows the love life of two young adults. AN AMERICAN PICKLE (PG) 8.10pm 9.40pm FOUR KIDS & IT (PG) Michael Caine, Paula Patton, Russell Brand. Sept 26th Sat CATS & DOGS 3 PAWS UNITE (G) 11.00am 12.30pm A group of kids on holiday in Cornwall meet a magical ASTRO KID (G) 90 12.50pm 2.20pm creature on the beach with the power to grant wishes. TROLLS (G) 90 2.40pm 4.10pm RAMS (PG) SECRET GARDEN (PG) 100 4.30pm 6.10pm Sam Neill, Michael Caton. TROLLS (G) 90 6.30pm 8.00pm Brothers Colin and Les have been fighting for decades. Both AN AMERICAN PICKLE (PG) 8.20pm 9.50pm are award-winning sheep farmers but when disaster strikes and disease threatens their flocks. Sept 27th Sun TROLLS (G) 90 11.00am 12.30pm SLIM AND I (PG) SECRET GARDEN (PG) 100 12.50pm 2.30pm Joy McKean, Missy Higgins, Keith Urban. TROLLS (G) 90 2.50pm 4.20pm Joy McKean takes us on the road of her life, revealing the SECRET GARDEN (PG) 100 4.40pm 6.20pm story of her career, her touring around Australia, and her CATS & DOGS 3 PAWS UNITE (G) 6.30pm 8.00pm marriage of more than fifty years to Slim Dusty. -
Newsletter May 2010
May 2010 Newsletter ------------------------------------------- Yesterday & Today Records P.O.Box 54 Miranda NSW 2228 Ph: (02)95311710 Email: [email protected] Web: www.yesterdayandtoday.com.au ------------------------------------------------------ Post: 1 cd $2/ 2 cds $3/ 3-4 Cds $6.50 Registered or express post available. ------------------------------------------------------ This may be a bold statement but I believe this is the best newsletter I have ever put out. There are Literally hundreds upon hundreds of great titles. If you would like to order from this newsletter you can email, phone or post an order. If phoning please feel free to call after hours From 8.00am up until 7.00pm is fine. I have a couple of pieces of bad news. Firstly my dear mum, Rose Reid, passed away on February 23rd. Many knew her as she worked Wednesdays at the old Parramatta store from 1990-2000 and filled in when I went on buying trips. It has been a trying period but I can honestly say she loved her time in the shop especially meeting and talking to many fine people and was a keen music buff, something that has passed on through the genes. Secondly, we lost a dear friend in Norm Pyne. Many who went to the Parramatta store would have seen a blind guy getting round with only a cane. My admiration for Norm was limitless. I never considered him handicapped in any way and he was always thankful for his independence. It is a sad irony of life that it is probably this independence which saw him involved in an horrific accident which cost him his life. -

Stars Unite for Slim Dusty Day Some of the Biggest Names in Australia Are Behind the Industry Life He Lived
Can you help us take the last steps to make June 13 – “National Slim Dusty Day”? June 13 is Slim Dusty’s birthday, and the Slim Dusty Foundation and makes us who we are. Together, in the spirit of true Aussie is asking all Australians to write to the Australian Government to mateship, our voice for Slim can be heard! voice their support for the official recognition of National Slim Please email or write to: Dusty Day. For more than half a century, Slim Dusty told the story of Australia. Senator the Hon George Brandis QC Our strengths and weaknesses, triumphs and failures. Minister for Arts His was a rich canvas inspired by Lawson, early explorers and PO Box 6100 Aboriginal people, but it was one on which he painted in music the Senate – Parliament House, Canberra ACT 2600 triumph of Australian character against the odds. email [email protected] He saw beauty and simple, gritty poetry in the everyday Australian — ringers, truckies, barmen, diggers, dreamers, story tellers and In this way, you are joining with your mates to call upon the battlers. Australian Federal Government to declare June 13 as “National Slim He loved Australia, town and country. He is us and we are him. Dusty Day” on an annual basis to celebrate our musical heritage, the National Slim Dusty Day celebrates our musical heritage, the people’s people’s King of Country and the everyday Australian who built our King of Country and the everyday Australian who built our nation nation and makes us who we are. -

Beyond the Bush Ballad: Authenticity in Australian Country Music
Beyond The Bush Ballad: Authenticity in Australian Country Music Amy Bauder Bachelor of Arts (Hons), Sydney University Macquarie University Faculty of Arts Department of Music, Media, Communication and Cultural Studies A thesis submitted in fulfilment of the requirements for the degree of Doctor of Philosophy August 2016 Table of Contents Table of Contents 1 List of Figures 3 Abstract 4 Statement of Authenticity 5 Acknowledgements 6 Part One: Contexts 9 Chapter One: Introduction 9 “Just Make Sure It Is Australian” 9 Defining Country Music: It Is About More Than the Sound 12 The Great Country Songbook: Ethnographic Fieldwork 13 “Distinctions” in the “Field”: Theoretical Framework 15 Contested Traditions and Mateship 20 “True Blue Bust-Up” 25 Thesis Structure 30 Chapter Two: Literature Review, Theoretical Framework and Methodology 33 Literature Review 33 Theoretical or Analytic Framework 59 Methodology 69 Fieldwork 78 Chapter Three: Roots and Heritage 89 “Honouring an Australian ‘Legend’”: Fieldwork Account 89 Slim Dusty as Touchstone for Australian Country Music 91 The Country Music Canon 92 Slim’s Life Story 95 Sources of the Legend 96 Part Two: People and RelationshipsWhat Are the elements? 10197 Introduction 101 Family 103 Coming Home: Fieldwork Account 103 Public Private Lives 107 Travelling Family Band: The Slim Dusty Family as Pioneers 108 The Family Business 112 Professionals and Stars 118 The Family Business Redux 119 Mateship 127 Troy Cassar-Daley & Friends: Fieldwork Account 127 “It’s Good to See You Mate”: Friendship in the -

Winners of the 2019 Australian Women in Music Awards Announced
WINNERS OF THE 2019 AUSTRALIAN WOMEN IN MUSIC AWARDS ANNOUNCED JOY McKEAN, CHRISTINE ANU, MOJO JUJU, ALICE SKYE, CAROLINE ALMONTE, ANGE McCORMACK and KATIE NOONAN are among the winners of the 2019 AUSTRALIAN WOMEN IN MUSIC AWARDS. In only its second year, AWMA has become a beacon of women’s contributions and achievements across all areas of the Australian music industry. CHRISTINE ANU picked up two AWMAs – DIVERSITY IN MUSIC and ARTISTIC EXCELLENCE – in acknowledgement of decades of work and her extensive contribution and commitment to Australia’s cultural music scene. Singer-songwriter ALICE SKYE took out the EMERGING ARTIST AWARD. With a voice described as “a combination of hopeful and haunting”, Alice Skye’s songs centre around well-crafted and articulate lyrics of love, loss and life. Now living in Melbourne, this young Wergaia woman released her captivating debut album, Friends with Feelings, in 2018 and toured nationally with Emily Wurramara. Winner of this year’s SONGWRITER AWARD, MOJO JUJU's third album, Native Tongue, was released in August 2018 to critical acclaim. Through the telling of family history and her own personal experiences, Mojo Juju’s songwriting explores her relationships with Elders and Ancestry and how that informs her own identity. As a fierce female advocate in the music industry, KATIE NOONAN was awarded the 2019 AWMA for CREATIVE LEADERSHIP, acknowledging her unwavering perseverance in aiding the development of Australia’s diverse musical landscapes. Katie Noonan has proven herself one of Australia’s most hardworking, versatile and prolific artists, as well as championing female-fronted and community projects.