IV-Human Physiology-Respiratory System-7-8
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
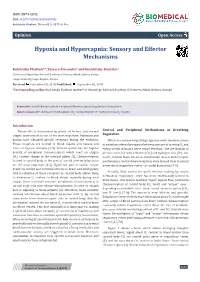
Hypoxia and Hypercapnia: Sensory and Effector Mechanisms
ISSN: 2574-1241 Volume 5- Issue 4: 2018 DOI: 10.26717/BJSTR.2018.08.001692 Kulchitsky Vladimir. Biomed J Sci & Tech Res Opinion Open Access Hypoxia and Hypercapnia: Sensory and Effector Mechanisms Kulchitsky Vladimir1*, Zamaro Alexandra1 and Koulchitsky Stanislav2 1Institute of Physiology, National Academy of Sciences, Minsk, Belarus, Europe 2Liege University, Liege, Belgium, Europe Received: Published: *Corresponding September author: 03, 2018; September 05, 2018 Kulchitsky Vladimir, Institute of Physiology, National Academy of Sciences, Minsk, Belarus, Europe Keywords: + Abbreviations:Central Chemoreceptors; Peripheral Chemoreceptors;2 Regulation of Respiration2 ATP: Adenosine Triphosphate; CО : Carbon Dioxide; H : Hydrogen Ions; О : Oxygen Introduction Human life is determined by plenty of factors, and normal Central and Peripheral Mechanisms of Breathing oxygen environment is one of the most important. Mammals and Regulation These receptors are located in blood vessels and tissues and in situations when discrepancy between amount of arriving O and human have obtained specific receptors during the evolution. Which mechanism helps living organism make timely decisions2 react on hypoxic stimulus [1-3]. Arterial system has the highest energy needs in brain’s nerve tissue develops? The mechanism of density of peripheral chemoreceptors which react on oxygen + precise control of carbon dioxide (CO2) and hydrogen ions (H ) - but (O ) content change in the internal milieu [1]. Chemoreceptors 2 not O2- in brain tissue has been evolutionally chosen. Such receptor located in carotid body in the area of carotid arteries bifurcation mechanisms (central chemoreceptors) were formed close to neural heads via carotid and vertebral arteries to brain, and strategically are the most important [2-5]. Significant part of cardiac output vital localization of those receptors in carotid body allows them networks of respiratory center - at caudal brain stem [7-9]. -

Chapter 22 We Won't Do Much Anatomy Here (Left Column; 22.1-22.3)
Chapter 22 Marieb & Hoehn (2019), p. 8181 We won’t do much anatomy here (left column; 22.1-22.3). Main issues (in lecture and lab): mechanics and measurement of breathing (22.4-22.5), chemoreceptor control of ventilation (22.8), and a few respiratory disorders (22.10). *** Sections 22.6-22.7 were briefly covered in Chapter 17. 1 Ch. 22: Test Question Templates • Q1. If given an appropriate graph of volume of air in lung vs. time, estimate or calculate FEV1/FVC ratio, FVC, residual volume, TLC, tidal volume, and/or minute ventilation. • Example (from Winter 2019 exam): 2 Q1. There are multiple ways to do this. The key is to choose a respiratory rate (breaths per minute) and a tidal volume (milliliters of air per breath) that, when multiplied together, give you 4000 mL air/minute. For example, I can draw a curve to show a tidal volume of 400 mL and a respiratory rate of 10 breaths/minute. Minute ventilation = (tidal volume)*(respiratory rate) = (400 mL air/breath)*(10 breaths/min) = 4000 mL air/min. 2 • Q2. If given two of the three values, calculate the third one: minute ventilation, respiratory rate, and tidal volume. • Example: Lola takes 10 breaths per minute, and her minute ventilation is 6000 mL air per minute. What is her tidal volume? • Q3. If given spirometry data and reference values, determine whether the data are consistent with obstructive pulmonary disease, restrictive pulmonary disease, both, or neither. • Example [from Fall 2019 test]: Rik is put through various pulmonary function tests. At time 0 in the table below, he begins deflating his fully inflated lungs as forcefully and rapidly as he can. -

For Pneumograph
For Pneumograph: Central chemoreceptors are primarily sensitive to changes in the pH in the blood, (resulting from changes in the levels of carbon dioxide) and they are located on the medulla oblongata near to the medullar respiratory groups of the respiratory center (1. Pneumotaxic center - various nuclei of the pons and 2. Apneustic center -nucleus of the pons). The peripheral chemoreceptors that detect changes in the levels of oxygen and carbon dioxide are located in the arterial aortic bodies and the carotid bodies. Information from the peripheral chemoreceptors is conveyed along nerves to the respiratory groups of the respiratory center. There are four respiratory groups, two in the medulla and two in the pons. From the respiratory center, the muscles of respiration, in particular the diaphragm, are activated to cause air to move in and out of the lungs. Hyperventilation: When a healthy person takes several deep and fast breaths (hyperventilation), PCO2 in the lungs and blood falls. As a result there is an increase in diffusion of CO2 to the alveolar air from dissolved state in blood. As the conc. of H2CO3 is in equilibrium with that of dissolved CO2 in blood, hyperventilation increases the [HCO3]/ [H2CO3] ratio by falling of CO2 conc. Thus there is a rise of blood pH (greater than pH 7.4). The breathing centre detects this change and stops or reduces stimulation and work of the respiratory muscles (called apnea). (Blood leaving the lungs is normally fully saturated with oxygen, so hyperventilation of normal air cannot increase the amount of oxygen available.) Breath-holding: The person naturally holds their breath until the CO2 level reaches the initially pre- set value. -

Human Physiology an Integrated Approach
Gas Exchange and Transport Gas Exchange in the Lungs and Tissues 18 Lower Alveolar P Decreases Oxygen Uptake O2 Diff usion Problems Cause Hypoxia Gas Solubility Aff ects Diff usion Gas Transport in the Blood Hemoglobin Binds to Oxygen Oxygen Binding Obeys the Law of Mass Action Hemoglobin Transports Most Oxygen to the Tissues P Determines Oxygen-Hb Binding O2 Oxygen Binding Is Expressed As a Percentage Several Factors Aff ect Oxygen-Hb Binding Carbon Dioxide Is Transported in Three Ways Regulation of Ventilation Neurons in the Medulla Control Breathing Carbon Dioxide, Oxygen, and pH Infl uence Ventilation Protective Refl exes Guard the Lungs Higher Brain Centers Aff ect Patterns of Ventilation The successful ascent of Everest without supplementary oxygen is one of the great sagas of the 20th century. — John B. West, Climbing with O’s , NOVA Online (www.pbs.org) Background Basics Exchange epithelia pH and buff ers Law of mass action Cerebrospinal fl uid Simple diff usion Autonomic and somatic motor neurons Structure of the brain stem Red blood cells and Giant liposomes hemoglobin of pulmonary Blood-brain barrier surfactant (40X) From Chapter 18 of Human Physiology: An Integrated Approach, Sixth Edition. Dee Unglaub Silverthorn. Copyright © 2013 by Pearson Education, Inc. All rights reserved. 633 Gas Exchange and Transport he book Into Thin Air by Jon Krakauer chronicles an ill- RUNNING PROBLEM fated trek to the top of Mt. Everest. To reach the summit of Mt. Everest, climbers must pass through the “death zone” T High Altitude located at about 8000 meters (over 26,000 ft ). Of the thousands of people who have attempted the summit, only about 2000 have been In 1981 a group of 20 physiologists, physicians, and successful, and more than 185 have died. -

Regulation of Respiration
Regulation of respiration Breathing is controlled by the central neuronal network to meet the metabolic ddfthbddemands of the body – Neural regulation – Chemical regulation Respiratory center Definition: – A collection of functionally similar neurons that help to regulate the respiratory movement Respiratory center Medulla Basic respiratory center: produce and control the respiratory Pons rhythm Higher respiratory center: cerebral cortex, hypotha la mus & limb ic syste m Spinal cord: motor neurons Neural regulation of respiration Voluntary breathing center – Cerebral cortex Automatic (involuntary) breathing center – Medulla – Pons Neural generation of rhythmical breathing The discharge of medullary inspiratory neurons provides rhythmic input to the motor neurons innervating the inspiratory muscles. Then the action pottiltential cease, the inspiratory muscles relax, and expiration occurs as the elastic lungs recoil. Inspiratory neurons Exppyiratory neurons Respiratory center Dorsal respiratory group (medulla) – mainly causes inspiration Ventral respiratory group (medulla) – causes either exp itiiration or insp itiiration Pneumotaxic center ((pppupper pons ) – inhibits apneustic center & inhibits inspiration,helps control the rate and pattern of breathing Apneustic center (lower pons) – to promote inspiration Hering-Breuer inflation reflex (Pulmonary stretch reflex) The reflex is originated in the lungs and media te d by the fibers o f the vagus nerve: – Pulmonary inflation reflex: inflation of the lungs, eliciting expiration. -

Math1 Is Essential for the Development of Hindbrain Neurons Critical for Perinatal Breathing
Neuron Article Math1 Is Essential for the Development of Hindbrain Neurons Critical for Perinatal Breathing Matthew F. Rose,1,7 Jun Ren,6,7 Kaashif A. Ahmad,2,7 Hsiao-Tuan Chao,3 Tiemo J. Klisch,4,5 Adriano Flora,4 John J. Greer,6 and Huda Y. Zoghbi1,2,3,4,5,* 1Program in Developmental Biology 2Department of Pediatrics 3Department of Neuroscience 4Department of Molecular and Human Genetics 5Howard Hughes Medical Institute Baylor College of Medicine, Houston, TX 77030, USA 6Department of Physiology, University of Alberta, Edmonton, Canada 7These authors contributed equally to this work *Correspondence: [email protected] DOI 10.1016/j.neuron.2009.10.023 SUMMARY died of SIDS appear to have been unable to arouse from sleep in response to hypoxia (Kato et al., 2003). A more complete Mice lacking the proneural transcription factor Math1 understanding of the respiratory network in the hindbrain could (Atoh1) lack multiple neurons of the proprioceptive provide insight into the pathogenesis of these disorders. and arousal systems and die shortly after birth from Respiratory rhythm-generating neurons reside within the an apparent inability to initiate respiration. We ventral respiratory column (VRC) of the medulla. The pre-Bo¨ t- sought to determine whether Math1 was necessary zinger complex (preBo¨ tC) generates the inspiratory rhythm for the development of hindbrain nuclei involved in (Smith et al., 1991) and receives modulatory input from adjacent nuclei, including a region located around the facial motor nucleus respiratory rhythm generation, such as the parafacial just rostral to the preBo¨ tC. Different investigators refer to respiratory group/retrotrapezoid nucleus (pFRG/ neurons in this region either as the parafacial respiratory group RTN), defects in which are associated with congen- (pFRG) or as the retrotrapezoid nucleus (RTN). -

Physiologic Effects of Noninvasive Ventilation
Physiologic Effects of Noninvasive Ventilation Neil R MacIntyre Introduction NIV Can Augment Minute Ventilation NIV Unloads Ventilatory Muscles NIV Resets the Ventilatory Control System Alveolar Recruitment and Gas Exchange Other Physiologic Effects of NIV: Intended and Unintended Maintaining Upper-Airway Patency Reducing Imposed Triggering Loads From Auto-PEEP Cardiac Interactions: Both Beneficial and Harmful Ventilator-Induced Lung Injury Production of Auto-PEEP Patient-Ventilator Interactions Summary Noninvasive ventilation (NIV) has a number of physiologic effects similar to invasive ventilation. The major effects are to augment minute ventilation and reduce muscle loading. These effects, in turn, can have profound effects on the patient’s ventilator control system, both acutely and chron- ically. Because NIV can be supplied with PEEP, the maintenance of alveolar recruitment is also made possible and the triggering load imposed by auto-PEEP can be reduced. NIV (or simply mask CPAP) can maintain upper-airway patency during sleep in patients with obstructive sleep apnea. NIV can have multiple effects on cardiac function. By reducing venous return, it can help in patients with heart failure or fluid overload, but it can compromise cardiac output in others. NIV can also increase right ventricular afterload or function to reduce left ventricular afterload. Potential det- rimental physiologic effects of NIV are ventilator-induced lung injury, auto-PEEP development, and discomfort/muscle overload from poor patient–ventilator interactions. Key words: invasive ventilation; noninvasive ventilation; minute and alveolar ventilation; ventilation distribution; ventilation-perfusion match- ing; control of ventilation; ventilatory muscles; work of breathing; patient–ventilator interactions; ventilator- induced lung injury. [Respir Care 2019;64(6):617–628. -

Integrative Actions of the Reticular Formation the Reticular Activating System, Autonomic Mechanisms and Visceral Control
University of Nebraska Medical Center DigitalCommons@UNMC MD Theses Special Collections 5-1-1964 Integrative actions of the reticular formation The reticular activating system, autonomic mechanisms and visceral control George A. Young University of Nebraska Medical Center This manuscript is historical in nature and may not reflect current medical research and practice. Search PubMed for current research. Follow this and additional works at: https://digitalcommons.unmc.edu/mdtheses Part of the Medical Education Commons Recommended Citation Young, George A., "Integrative actions of the reticular formation The reticular activating system, autonomic mechanisms and visceral control" (1964). MD Theses. 69. https://digitalcommons.unmc.edu/mdtheses/69 This Thesis is brought to you for free and open access by the Special Collections at DigitalCommons@UNMC. It has been accepted for inclusion in MD Theses by an authorized administrator of DigitalCommons@UNMC. For more information, please contact [email protected]. THE INTEGRATIVE ACTIONS OF THE RETICULAR FORlVIATION The Reticular Activating System, Autonomic Mechanisms and Visceral Control George A. Young 111 Submitted in Partial Fulfillment for the Degree of Doctor of Medicine College of Medicine, University of Nebraska February 3, 1964 Omaha, Nebraska TABLE OF CONTENTS Page I. Introduction. ~4'~ •••••••••••• *"' ••• " ••• "' ••• 1I •• 1 II. The Reticula.r Activa.ting System (a) Historical Review •••.....•..•.•. · ••••• 5 (1) The Original Paper~ ..•.••...••.••••. 8 (2) Proof For a R.A.S •.•...•.....•••.• ll (b) ,The Developing Concept of the R.A.S ••• 14 (1) R.A.S. Afferents •..•.•......••..• 14 (2) The Thalamic R.F •••.••.......••.••. 16 (3) Local Cortical Arousal •••••••.•.••• 18 (4) The Hypothalamus end the R.A.S ••••• 21 (5) A Reticular Desynchronizing System. -

Control of Respiration Central Control of Ventilation
Control of Respiration Control of Respiration Bioengineering 6000 CV Physiology Central Control of Ventilation • Goal: maintain sufficient ventilation with minimal energy – Ventilation should match perfusion • Process steps: – Ventilation mechanics + aerodynamics • Points of Regulation – Breathing rate and depth, coughing, swallowing, breath holding – Musculature: very precise control • Sensors: – Chemoreceptors: central and peripheral – Stretch receptors in the lungs, bronchi, and bronchioles • Feedback: – Nerves – Central processor: • Pattern generator of breathing depth/amplitude • Rhythm generator for breathing rate Control of Respiration Bioengineering 6000 CV Physiology Peripheral Chemosensors • Carotid and Aortic bodies • Sensitive to PO2, PsCO2, and pH (CO2 sensitivity may originate in pH) • Responses are coupled • Adapt to CO2 levels • All O2 sensing is here! • Carotid body sensors more sensitive than aortic bodies Control of Respiration Bioengineering 6000 CV Physiology O2 Sensor Details • Glomus cells • K-channel with O2 sensor • O2 opens channel and hyperpolarizes cell • Drop in O2 causes reduction in K current and a depolarization • Resulting Ca2+ influx triggers release of dopamine • Dopamine initiates action potentials in sensory nerve Control of Respiration Bioengineering 6000 CV Physiology Central CO2/pH Chemoreceptors • Sensitive to pH in CSF • CSF poorly buffered • H+ passes poorly through BBB but CO2 passes easily • Blood pH transmitted via CO2 to CSF • Adapt to elevated CO2 levels (reduced pH) by transfer of - - HCO3 -

Brainstem Dysfunction in Critically Ill Patients
Benghanem et al. Critical Care (2020) 24:5 https://doi.org/10.1186/s13054-019-2718-9 REVIEW Open Access Brainstem dysfunction in critically ill patients Sarah Benghanem1,2 , Aurélien Mazeraud3,4, Eric Azabou5, Vibol Chhor6, Cassia Righy Shinotsuka7,8, Jan Claassen9, Benjamin Rohaut1,9,10† and Tarek Sharshar3,4*† Abstract The brainstem conveys sensory and motor inputs between the spinal cord and the brain, and contains nuclei of the cranial nerves. It controls the sleep-wake cycle and vital functions via the ascending reticular activating system and the autonomic nuclei, respectively. Brainstem dysfunction may lead to sensory and motor deficits, cranial nerve palsies, impairment of consciousness, dysautonomia, and respiratory failure. The brainstem is prone to various primary and secondary insults, resulting in acute or chronic dysfunction. Of particular importance for characterizing brainstem dysfunction and identifying the underlying etiology are a detailed clinical examination, MRI, neurophysiologic tests such as brainstem auditory evoked potentials, and an analysis of the cerebrospinal fluid. Detection of brainstem dysfunction is challenging but of utmost importance in comatose and deeply sedated patients both to guide therapy and to support outcome prediction. In the present review, we summarize the neuroanatomy, clinical syndromes, and diagnostic techniques of critical illness-associated brainstem dysfunction for the critical care setting. Keywords: Brainstem dysfunction, Brain injured patients, Intensive care unit, Sedation, Brainstem -

Brainstem Dysfunction in Critically Ill Patients
Benghanem et al. Critical Care (2020) 24:5 https://doi.org/10.1186/s13054-019-2718-9 REVIEW Open Access Brainstem dysfunction in critically ill patients Sarah Benghanem1,2 , Aurélien Mazeraud3,4, Eric Azabou5, Vibol Chhor6, Cassia Righy Shinotsuka7,8, Jan Claassen9, Benjamin Rohaut1,9,10† and Tarek Sharshar3,4*† Abstract The brainstem conveys sensory and motor inputs between the spinal cord and the brain, and contains nuclei of the cranial nerves. It controls the sleep-wake cycle and vital functions via the ascending reticular activating system and the autonomic nuclei, respectively. Brainstem dysfunction may lead to sensory and motor deficits, cranial nerve palsies, impairment of consciousness, dysautonomia, and respiratory failure. The brainstem is prone to various primary and secondary insults, resulting in acute or chronic dysfunction. Of particular importance for characterizing brainstem dysfunction and identifying the underlying etiology are a detailed clinical examination, MRI, neurophysiologic tests such as brainstem auditory evoked potentials, and an analysis of the cerebrospinal fluid. Detection of brainstem dysfunction is challenging but of utmost importance in comatose and deeply sedated patients both to guide therapy and to support outcome prediction. In the present review, we summarize the neuroanatomy, clinical syndromes, and diagnostic techniques of critical illness-associated brainstem dysfunction for the critical care setting. Keywords: Brainstem dysfunction, Brain injured patients, Intensive care unit, Sedation, Brainstem -
Department of Internal Medicine, Both to End This Pandemic and to Ensure That Racial Inequities Are Ameliorated, E
DEPARTMENTVitals OF INTERNAL MEDICINE internalmedicineiowa.org Vitals Table of Contents From the chair .....................................................................................................................3 RESEARCH ...........................................................................................................................4 UI nephrologists collaborate on new textbook ......................................................6 Gehlbach, Richerson to investigate carbon dioxide role in SUDEP ................7 Abel to lead one of four AHA research networks .................................................8 Model developed to calculate patient risk for NAFLD decompensation .....9 Clinical trials in cancer at Iowa barely lose a step ..............................................10 EDUCATION .....................................................................................................................12 Grand Rounds expands its reach ..............................................................................14 Residency committees spotlight ...............................................................................16 On the cover OSCE gets national exposure, refines and expands again ..............................18 Microscopic image of a mouse lung expressing human ACE2, the receptor PATIENT CARE ................................................................................................................20 for SARS-CoV2. The blue staining represents the normal mouse lung, UI Hospitals & Clinics provides