Download File
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Appointing the UN Secretary-General
Updated October 13, 2016 United Nations Issues: Appointing the U.N. Secretary-General The second five-year term of United Nations (U.N.) for consideration. The Council’s deliberations generally Secretary-General (SG) Ban Ki-moon ends on December occur in private meetings, with decisions taken by secret 31, 2016. For the past several months, the U.N. Security ballot by an affirmative vote from at least seven Council Council and General Assembly have considered candidates members, including the five permanent members (P-5). to serve as the ninth SG. On October 6, the Council When a decision is made, the Council adopts a resolution recommended António Guterres of Portugal, and the recommending a candidate; generally, the resolution is Assembly appointed him on October 13. Guterres served as considered during a private Council meeting. the Prime Minister of Portugal from 1995 to 2002 and as the U.N. High Commissioner for Refugees from 2005 to In years when there have been multiple candidates, the 2015. His term will begin on January 1, 2017. Council has developed the practice of conducting informal straw polls to indicate member states’ initial level of The United States maintains a significant interest in the SG support for individuals. (In the current process, Guterres appointment process, with the hope that the perspectives won all six straw polls held by the Council.) In years when and policies of the new SG align with U.S. foreign policy there has been one candidate (for example, when an SG is and national security priorities. As one of five permanent being considered for a second term), the Council generally members of the Council with veto power, it has adopts a resolution without prior polling, usually by considerable influence in the selection of the SG. -

Martin Shichtman Named Director of EMU Jewish Studies
Washtenaw Jewish News Presort Standard In this issue… c/o Jewish Federation of Greater Ann Arbor U.S. Postage PAID 2939 Birch Hollow Drive Ann Arbor, MI Federation Biking 2010 Ann Arbor, MI 48108 Permit No. 85 Main Event Adventure Election In Israel Results Page 5 Page 7 Page 20 December 2010/January 2011 Kislev/Tevet/Shevat 5771 Volume XXXV: Number 4 FREE Martin Shichtman named director of EMU Jewish Studies Chanukah Wonderland at Geoff Larcom, special to the WJN Briarwood Mall Devorah Goldstein, special to the WJN artin Shichtman, a professor of Shichtman earned his doctorate and mas- English language and literature ter’s degree from the University of Iowa, and What is white, green, blue and eight feet tall? M who has taught at Eastern Michi- his bachelor’s degree from the State Univer- —the menorah to be built at Chanukah Won- gan University for 26 years, has been appointed sity of New York, Binghamton. He has taught derland this year. Chabad of Ann Arbor will director of Jewish Studies for the university. more than a dozen courses at the graduate sponsor its fourth annual Chanukah Wonder- As director, Shichtman will create alliances and undergraduate levels at EMU, including land, returning to the Sears wing of Briarwood with EMU’s Jewish community, coordinate classes on Chaucer, Arthurian literature, and Mall, November 29–December 6, noon–7 p.m. EMU’s Jewish Studies Lecture Series and de- Jewish American literature. Classes focusing New for Chanukkah 2010 will be the building of velop curriculum. The area of Jewish studies on Jewish life include “Imagining the Holy a giant Lego menorah in the children’s play area includes classes for all EMU students inter- Land,” and “Culture and the Holocaust.” (near JCPenny). -
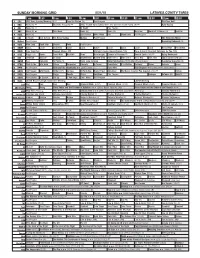
Sunday Morning Grid 5/31/15 Latimes.Com/Tv Times
SUNDAY MORNING GRID 5/31/15 LATIMES.COM/TV TIMES 7 am 7:30 8 am 8:30 9 am 9:30 10 am 10:30 11 am 11:30 12 pm 12:30 2 CBS CBS News Sunday Morning (N) Å Face the Nation (N) Paid Program PGA Tour Golf 4 NBC News (N) Å Meet the Press (N) Å 2015 French Open Tennis Men’s and Women’s Fourth Round. (N) Å Auto Racing 5 CW News (N) Å In Touch Paid Program 7 ABC News (N) Å This Week News (N) News (N) News Å World of X Games (N) IndyCar 9 KCAL News (N) Joel Osteen Mike Webb Paid Woodlands Paid Program 11 FOX In Touch Joel Osteen Fox News Sunday Midday Paid Program The Simpsons Movie 13 MyNet Paid Program Becoming Redwood (R) 18 KSCI Man Land Rock Star Church Faith Paid Program 22 KWHY Cosas Local Jesucristo Local Local Gebel Local Local Local Local RescueBot RescueBot 24 KVCR Easy Yoga Pain Deepak Chopra MD JJ Virgin’s Sugar Impact Secret (TVG) Suze Orman’s Financial Solutions for You (TVG) 28 KCET Raggs Pets. Space Travel-Kids Biz Kid$ News Asia Insight Echoes of Creation Å Sacred Earth (TVG) Å Aging Backwards 30 ION Jeremiah Youssef In Touch Bucket-Dino Bucket-Dino Doki (TVY7) Doki (TVY7) Dive, Olly Dive, Olly Taxi › (2004) (PG-13) 34 KMEX Paid Conexión Al Punto (N) Hotel Todo Incluido Duro Pero Seguro (1978) María Elena Velasco. República Deportiva (N) 40 KTBN Walk in the Win Walk Prince Carpenter Liberate In Touch PowerPoint It Is Written Pathway Super Kelinda Jesse 46 KFTR Paid Program Alvin and the Chipmunks ›› (2007) Jason Lee. -

BBC Ultimately Successful in Russian “Top Gear” Trademark Saga
DE BERTI JACCHIA FRANCHINI FORLANI BBC ultimately successful in Russian “Top Gear” trademark saga 09/12/2019 INTELLECTUAL PROPERTY, RUSSIA Alisa Pestryakova of the assignment of the earlier mark and rademark “Top Gear” was registered registration of a new trademark by the T entrepreneur was to create an obstacle in Russia by the British Broadcasting to BBC’s mark. The British company Corporation (BBC) in 2015. Another asked the Court that its trademark “Top trademark “TopGear” owned by a Gear” should be maintained and also Russian company was registered in 2005 filed a cancellation application on non- for similar services, but the Russian PTO use basis against the earlier mark of the did not find grounds for refusal, and entrepreneur. The Court upheld the registered BBC’s mark. The mark cancellation decision of the Russian PTO “TopGear” owned by the Russian entity and held that neither the argument of was assigned to a Russian entrepreneur BBC on the abuse of right by the in 2016, who later also registered entrepreneur nor the cancellation of the another mark “TopGear” for the same earlier mark could affect the judgement. services in 2017. The details of the case were also described in the article “Battle for BBC Based on the application of the Top Gear trademark in Russia” published entrepreneur, the Russian PTO on Lexology on July 23, 2019. cancelled the “Top Gear” mark of BBC in (https://www.lexology.com/library/detail.a 2018 on the ground of the existence of a spx?g=14572e67-3758-4e95-8bce- similar mark with an earlier priority. -

Dr. Cicely Williams Cicely Williams Was Born in 1893 at Kew Park, Darliston, Westmoreland, and Was Educated in Jamaica, Partly at Walmer's Girls' School
Dr. Cicely Williams Cicely Williams was born in 1893 at Kew Park, Darliston, Westmoreland, and was educated in Jamaica, partly at Walmer's Girls' School. During World War I in 1914 she started to take First Aid and nursing classes and thought seriously about studying medicine. In 1916, after her fathers death she decided to go to Oxford, her father's alma mater. She was one of the women admitted because there were so few male students during the war. After graduation in 1923 Cicely decided to specialize in paediatrics and soon applied to the British Colonial Office for an overseas posting. She was sent to the Gold Coast (now Ghana) in 1929 and spent 7 years there, learning to speak Twi and working to improve health conditions. She established clinics and hospitals and improved record keeping. She also worked with African herbal doctors to learn their treatments for diseases for which European medicine had no cures. Dr. Williams· most important work in Africa was her diagnosis of the common and often fatal condition kwashiorkor. She learned that ..kwashiorkor .. meant the sickness the older child gets when the next baby is born. This seemed to indicate that, when they were no longer breast-fed, children were not receiving enough to eat. The cure for kwashiorkor was therefore education on children's nutritional needs. She quickly published her diagnosis of kwashiorkor as a protein deficiency disease, which attracted the attention of the medical world. In the late 1930s she was transferred to Malaya. After suffering from terrible conditions and bad treatment during World War II in Japanese prisoner of war camps, which brought her near to death, she returned to Malaya and was first woman placed in charge of the maternity and child welfare services. -
Who Wants to Be a Millionaire Host on 'Worst Year'
7 Ts&Cs apply Iceland give huge discount Claire King health: Craig Revel Horwood Kate Middleton pregnant Jenny Ryan: ‘The cat is out to emergency service Emmerdale star's health: ‘It was getting with twins on royal tour in the bag’ The Chase quizzer workers - find… diagnosis ‘I was worse’ Strictly… Pakistan?… announces… Jeremy Clarkson: ‘Wanted to top myself’ Who Wants To Be A Millionaire host on 'worst year' JEREMY CLARKSON - who fronts ITV show Who Wants To Be A Millionaire? - shared his thoughts on a recent study which claimed 1978 was the “worst year” in British history. Who Wants to Be a Millionaire: Jeremy criticises the contestant Earlier this week, researchers from Warwick University claimed people of Britain were at their most unhappy in 1978. The latter year and the first two months of 1979 are best remembered for the Winter of Discontent, where strikes took place and caused various disruptions. ADVERTISING 1/6 Jeremy Clarkson (/search?s=jeremy+clarkson) shared his thoughts on the study as he recalled his first year of working during the strikes. PROMOTED STORY 4x4 Magazine: the SsangYong Musso is a quantum leap forward (SsangYong UK)(https://www.ssangyonggb.co.uk/press/first-drive-ssangyong-musso/56483&utm-source=outbrain&utm- medium=musso&utm-campaign=native&utm-content=4x4-magazine?obOrigUrl=true) In his column with The Sun newspaper, he wrote: “It’s been claimed that 1978 was the worst year in British history. RELATED ARTICLES Jeremy Clarkson sports slimmer waistline with girlfriend Lisa Jeremy Clarkson: Who Wants To Be A Millionaire host on his Hogan weight loss (/celebrity-news/1191860/Jeremy-Clarkson-weight-loss-girlfriend- (/celebrity-news/1192773/Jeremy-Clarkson-weight-loss-health- Lisa-Hogan-pictures-The-Grand-Tour-latest-news) Who-Wants-To-Be-A-Millionaire-age-ITV-Twitter-news) “I was going to argue with this. -
Rally Panel Report 13/4/15
Rally Panel Report 13/4/15 Prepared for: State Council Prepared by: Matt Martin, Rally Panel Chairman. 2015 Registrations 2015 Registrations as at 13/4. 2015 2014 2013 NSWRC 71 70 34 DRS 36 68 11 DRS4 26 (new series for 2015) ERS 3 11 2 RSS 68 58 6 PRS 27 (new series for 2015) Total 231 207 53 The Rallysrpint series continues to grow, with both new competitors and new events joining the series. After consulting registered competitors, the Panel has added a 7th round on 27/6/15 at WSID in Sydney. The discipline of Rallysprinting is considered strategically important by the Rally Panel, as it is our number one gateway event for new competitors. The State championship is back. The panel has devoted much energy and resources into this area, and the 2015 championship is showing great signs. Bega has returned for 2015, as well as a new event in Glen Innes, which saw 51 entries on 28/3/15. The panel is aware of another landmark state championship event which will most likely return for 2016, and are very excited by that. We look forward to releasing the 2016 calendar later in the year. The DRS in 2015 has been split into 2, which allows for 4WD turbo cars. Whilst numbers in the DRS4 component are up, the participation in the 2WD sections is lower than last year at this stage. Number in Hyundai series are also down, but we are aware of at least 3 crews who are planning on contesting the later rounds. -

Hiscocks List
Liddell Hart Centre for Military Archives King's College London Brief List HISCOCKS, Prof Charles Richard 1. Publications by and about the United Nations, 1946-83 (19 items) 2. Publications by and about the North Atlantic Treaty Organisation (NATO), 1952- 1981 (7 items) 3. Publications by the International Labour Organisation (ILO), 1955-1971 (14 items) 4. Publications by and about the International Development Association, 1972-1982 (3 items) 5. Publications relating to specific geographical areas, 1928, 1949-1964 6. Other publications, 1946-1980 (5 items) Detailed List 1. Publications by and about the United Nations, 1946-83 (19 items) United Nations documents, 1941-1945 (Royal Institute of InternationalAffairs, London, 1946) Report of the ad hoe committee on forced labour (United Nations and International Labour Organisation, Geneva, 1953) Rules of procedure of the functional commissions of the economic and social council (United Nations, New York, 1953) World economic report, 1951-1952 (United Nations Department of Economic Affairs, New York, 1953) The United Nations family: the work of the specialised agencies by Leslie Aldous (United Nations Association, London, 1968) Britain and the United Nations (Central Officeof Information, London, 1969) A principle in torment: i) The United Nations and SouthernRhodesia ii) The United Nations and Portuguese administered territories (United Nations Office of Public Information,DRAFT New York, 1969, 2 volumes) Provisional rules of procedure of the Security Council (United Nations, New York, 1969) -

Nazi War Crimes Disclosure Ac
CONFIDENTIAL FOUO DOCUMENT ID: 21578164 INQNO: DOC8D 00282509 DOCNO: TEL 002784 88 PRODUCER: VIENNA SOURCE: STATE DOCTYPE: IN DOR: 19880309 TOR: 025847 DOCPREC: R ORIGDATE: 198803081446 MHFNO: 88 8125375 I I . [CATION REVIEW DOCCLASS: C o Ret:.:.:1 CAVEATS: FOUO iz1. 1 col1C.; rrence of HEADER EO 1253. 25X RR RUEAIIB IRSICRAR by ZNY CCCCC ZOC STATE ZZH UTS8452 RR RUEHC DE RUFHVI #2784/01 0681448 ZNY CCCCC ZZH R 081446Z MAR 88 FM AMEMBASSY VIENNA TO SECSTATE WASHDC 0431 BT D ECLASSIFIED AND RELEASED BY CONTROLS CENTRAL INTELLIGENCE ABENCY CONFIDENTIAL SOURCESMETHODSEXEMPTION3B2B LIMITED OFFICIAL USE VIENNA 02784 NAZI WAR CRIMESOISCLOSUREACT DATE 2001 2007 E.O. 12356: N/A TEXT TAGS: PREL, PGOV, AU, US SUBJECT: AMBASSADOR VISITS SALZBURG AND TIROL 1. SUMMARY: AMBASSADOR GRUNWALDS FIRST OFFICIAL VISIT OUTSIDE THE CAPITAL CITY INCLUDED A ROUND OF DISCUSSIONS WITH OFFICIALS IN SALZBURG AND TIROL PROVINCES, AS WELL AS AN OPPORTUNITY TO MEET MANY OTHER PROMINENT LOCAL RESIDENTS DURING TWO LARGE SOCIAL OCCASIONS IN SALZBURG AND INNSBRUCK. THESE LATTER EVENTS WERE WELL ATTENDED AND PROVIDED A TACIT BUT RATHER CLEAR INDICATION THAT MANY AUSTRIANS SEEM PREPARED TO ACCEPT A FRESH START IN AUSTRIAN-AMERICAN RELATIONS AFTER THE STRAINS CREATED BY U.S. MEASURES AGAINST PRESIDENT KURT WALDHEIM AND THEIR AFTERMATH. 2. MOST NOTABLE OF THE OFFICIAL DISCUSSIONS WAS THAT WITH SALZBURG GOVERNOR WILFRIED HASLAUER. THOUGH CLOSE TO WALDHEIM AND CONSISTENTLY ONE OF HIS MOST VOCAL SUPPORTERS, HASLAUER CAUTIOUSLY VENTURED THE NAZI WAR CRIMES DISCLOSURE AC- PERSONAL SPECULATION THAT AFTER SEVERAL MONTHS, ONCE 2000 THE CURRENT FUROR OVER THE HISTORIANS REPORT FINDINGS HAD SUBSIDED, WALDHEIM MAY AFTER ALL DECIDE TO RELINQUISH CIA HAS NO OBJECTION TO OECLASSINCATION AND/OR RELEASE OF CIA INPORMATKY IN THOI PONMPAT FOUO CONFIDENTIAL Page 1 CONFIDENTIAL FOUO HIS POST IN ORDER TO OVERCOME THE GREAT DIVISION THAT THE PRESIDENTIAL ISSUE HAS CREATED WITHIN THE AUSTRIAN PEOPLE. -

Summary of AG-011 United Nations Executive Office of the Secretary-General (EOSG) (1946-Present)
Summary of AG-011 United Nations Executive Office of the Secretary-General (EOSG) (1946-present) Title United Nations Executive Office of the Secretary-General (EOSG) (1946-present) Active Dates 1919-2014 Administrative History The Executive Office of the Secretary-General (EOSG) was established initially in 1946 to assist the Secretary-General with relations with members and organs of the United Nations, and with specialized agencies and non-governmental organizations, as well as to assist with policy and coordination of the Secretariat. It was established shortly after the first Secretary-General of the United Nations took office following appointment by the General Assembly on 1 February 1946. The Executive Office of the Secretary-General "assists the Secretary-General in the performance of those functions which he does not delegate to the departments and for which he retains personal responsibility. These functions include consultation with governments and the heads of the specialized agencies and the supervision of special projects" (YUN, 1947-1948) It also aids in policy creation and implementation, coordinates the activities of the departments, publications and correspondence, and advises on UN protocol. The following Secretariat bodies reported to the Secretary-General from the beginning: the Department of Security Council Affairs, the Department of Economic Affairs, the Department of Social Affairs, the Department of Trusteeship and Information from Non-Self-Governing Territories, the Department of Public Information, the Department of Legal Affairs, the Department of Conference and General Services, and the Department of Administrative and Financial Services. From 1946 through the 1950s the EOSG was responsible for protocol and liaison with diplomatic representatives, as well as for relationships with non-governmental organizations, communications with member state representatives and related, and for the coordination and support of General Assembly activities. -

Modern Newspaper Management and Press Laws
MODERN NEWSPAPER MANAGEMENT AND PRESS LAWS Syllabus Newspaper – Overview, Definitions, History, Gazettes and bulletins, Industrial Revolution Categories – Daily, Weekly and other, Geographical scope and distribution, Local or regional, National Subject matter – Technology: Print, Online, Formats Newspaper production process. News gathering - Pre press, Press: Lithographic stage, Impression stage, Post press Media & Press Laws Press, Law, Society & Democracy Constitutional Safeguards To Freedom Of Press Meaning Of Freedom Basis Of Democracy Role Of Journalism Role Of Journalism In Society The Power Of Press Press Commissions & Their Recommendations Press & Registration Of Books Act Press Council Working Journalist Act Law Of Libel & Defamation Official Secret Act Parliamentary Privileges Right To Information Copyright Act Social Responsibility Of Press & Freedom Of Expression MODERN NEWSPAPER MANAGEMENT AND PRESS LAWS Tutorial A newspaper is a periodical publication containing written information about current events. Newspapers can cover wide variety of fields such as politics, business, sport and art and often include materials such as opinion columns, weather forecasts, reviews of local services, obituaries, birth notices, crosswords, editorial cartoons, comic strips, and advice columns. Most newspapers are businesses, and they pay their expenses with a mixture of subscription revenue, newsstand sales, and advertising revenue. The journalism organizations that publish newspapers are themselves often metonymically called newspapers. Newspapers have traditionally been published in print (usually on cheap, low- grade paper called newsprint). However, today most newspapers are also published on websites as online newspapers, and some have even abandoned their print versions entirely. Newspapers developed in the 17th century, as information sheets for businessmen. By the early 19th century, many cities in Europe, as well as North and South America, published newspapers. -

Em Mch 155 Em Reg Sct Wrk
REPORT ON THE REGIONAL SCIENTIFIC WORKING GROUP ON BREASTFEEDING NICOSIA, CYPRUS 26 - 30 January 1981 The views expressed in this Report do not necessarily reflect the official policy of the World Health Organization TABLE OF CONTENTS 1.1 RECENT ADVANCES IN KNOWLEDGE CONCERNING BREASTFEEDING 5 1.2 RECENT DEVELOPMENTS IN PROGRAMMES TO PROMOTE AND PROTECT 8 BREASTFEEDING 2. MVLEW OY THE !3MASTYEEULNG SITUATLON IN 'lXE REGION 13 3. PROPOS.ALS FOK KLSEARCH CONCERNING THC PREVA1.ESCL AN11 nI'HATTON l)r '!RI:A$II:FI:I)TUC ANn ASSOI'TATFn FACTORS 4. PROMOTIONAL AND EDUCATIONAL ACTIVITIES FOR THE PUBLIC ON 22 BREASTFEEDING 5. THE TRAINING OF HEALTH WORKERS CONCERNING BREASTFEEDING 25 6. THE PROPOSED CODE OF MARKETTNG OF BREAST-MT1.K SITRSTTT1TTF.S 28 7. THE ROLE OF WOMEN'S ORGANIZATIONS IN THE SUPPORT OF BREASTFEEDING 29 8. MATERNITY OR "LACTATION" LFAVE 9. LEARNING MATERIALS ON BREASTFEEDING RECOMMENDATIONS 40 ANNEXES I. OPENING ADDRESS OF H.E. THE MINISTER OF HEALTH, MR G. TOMBAZOS !i. MESSAGE FROM DR A.H. TABA, DIRECTOR WHO EASTERN MEDITERRANEAN REGION 111. TiiE TEXTS OF WORLD HEALTH ASSEMBLY RESOLUTIONS 27.43 of 1974, 31.17 "1 1978 arid 33.32 "1 1980 1V DRAFT INTERNATIONAI. CODE OF MARKETING OF BREAST-MILK SUBSTITUTES AS SUBMITTED TC: Ti!i: WHO EXECUTIVE BOARD IN JANUARY 1981; IN ITS RECOMMENMTION FORM. (WHO DOCUMENT EB 67/20 PAGES 14 THROUGH 21) V. LIST OF PARTICIPANTS Ever since infant formulas manufactured industrially became available on a large scale early this century as substitutes for breast-milk, it is probably true that most doctors have nevertheless believed that breastfeeding was the method of feeding more likely to result in an infant's hsalthv growth.