Dentin Permeability of the Apical Third in Different Groups of Teeth
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Maxillary Lateral Incisor Agenesis and Its Relationship to Overall Tooth Size Jane Wright, DDS, MS,A Jose A
RESEARCH AND EDUCATION Maxillary lateral incisor agenesis and its relationship to overall tooth size Jane Wright, DDS, MS,a Jose A. Bosio, BDS, MS,b Jang-Ching Chou, DDS, MS,c and Shuying S. Jiang, MSd Prosthodontists, orthodontists, ABSTRACT and general dentists frequently fi Statement of problem. Agenesis of the maxillary lateral incisor has been linked to differences in encounter dif culties when the size of the remaining teeth. Thus, the mesiodistal space required for definitive esthetic resto- attempting to restore the oc- ration in patients with missing maxillary lateral incisors may be reduced. clusion if unilateral or bilateral Purpose. The purpose of this study was to determine whether a tooth size discrepancy exists in maxillary lateral incisors are orthodontic patients with agenesis of one or both maxillary lateral incisors. congenitally missing. Restora- tion of the missing lateral Material and methods. Forty sets of dental casts from orthodontic patients (19 men and 21 women; mean 15.9 years of age; all of European origin) were collected. All casts had agenesis of one incisor using an implant- or both maxillary lateral incisors. Teeth were measured with a digital caliper at their greatest supported crown, a partial mesiodistal width and then compared with those of a control group matched for ethnicity, age, and fi xed dental prosthesis, or sex. Four-factor ANOVA with repeated measures of 2 factors was used for statistical analysis (a=.05). mesial movement of the Results. Orthodontic patients with agenesis of one or both maxillary lateral incisors exhibited canine are treatment options. smaller than normal tooth size compared with the control group. -

Tooth Size Proportions Useful in Early Diagnosis
#63 Ortho-Tain, Inc. 1-800-541-6612 Tooth Size Proportions Useful In Early Diagnosis As the permanent incisors begin to erupt starting with the lower central, it becomes helpful to predict the sizes of the other upper and lower adult incisors to determine the required space necessary for straightness. Although there are variations in the mesio-distal widths of the teeth in any individual when proportions are used, the sizes of the unerupted permanent teeth can at least be fairly accurately pre-determined from the mesio-distal measurements obtained from the measurements of already erupted permanent teeth. As the mandibular permanent central breaks tissue, a mesio-distal measurement of the tooth is taken. The size of the lower adult lateral is obtained by adding 0.5 mm.. to the lower central size (see a). (a) Width of lower lateral = m-d width of lower central + 0.5 mm. The sizes of the upper incisors then become important as well. The upper permanent central is 3.25 mm.. wider than the lower central (see b). (b) Size of upper central = m-d width of lower central + 3.25 mm. The size of the upper lateral is 2.0 mm. smaller mesio-distally than the maxillary central (see c), and 1.25 mm. larger than the lower central (see d). (c) Size of upper lateral = m-d width of upper central - 2.0 mm. (d) Size of upper lateral = m-d width of lower central + 1.25 mm. The combined mesio-distal widths of the lower four adult incisors are four times the width of the mandibular central plus 1.0 mm. -

Dental Anatomy Lecture (8) د
Dental Anatomy Lecture (8) د. حسين احمد Permanent Maxillary Premolars The maxillary premolars are four in number: two in the right and two in the left. They are posterior to the canines and anterior to the molars. The maxillary premolars have shorter crowns and shorter roots than those of the maxillary canines. The maxillary first premolar is larger than the maxillary second premolar. Premolars are named so because they are anterior to molars in permanent dentition. They succeed the deciduous molars (there are no premolars in deciduous dentition). They are also called “bicuspid -having two cusps-“, but this name is not widely used because the mandibular first premolar has one functional cusp. The premolars are intermediate between molars and canines in: Form: The labial aspect of the canine and the buccal aspect of premolar are similar. Function: The canine is used to tear food while the premolars and molars are used to grind it. Position: The premolars are in the center of the dental arch. [Type a quote from the document or the summary of [Type a quote from the document or the summary of an interesting point. You can position the text box an interesting point. You can anywhere in the document. position the text box Use the Text Box Tools tab to anywhere in the document. change the formatting of the Use the Text Box Tools tab to Some characteristic features to all posterior teeth: 1. Greater relative facio-lingual measurement as compared with the mesio-distal measurement. 2. Broader contact areas. 3. Contact areas nearly at the same level. -

Maxillary Premolars
Maxillary Premolars Dr Preeti Sharma Reader Oral & Maxillofacial Pathology SDC Dr. Preeti Sharma, Subharti Dental College, SVSU Premolars are so named because they are anterior to molars in permanent dentition. They succeed the deciduous molars. Also called bicuspid teeth. They develop from the same number of lobes as anteriors i.e., four. The primary difference is the well-formed lingual cusp developed from the lingual lobe. The lingual lobe is represented by cingulum in anterior teeth. Dr. Preeti Sharma, Subharti Dental College, SVSU The buccal cusp of maxillary first premolar is long and sharp assisting the canine as a prehensile or tearing teeth. The second premolars have cusps less sharp and function as grinding teeth like molars. The crown and root of maxillary premolar are shorter than those of maxillary canines. The crowns are little longer and roots equal to those of molars. Dr. Preeti Sharma, Subharti Dental College, SVSU As the cusps develop buccally and lingually, the marginal ridges are a little part of the occlusal surface of the crown. Dr. Preeti Sharma, Subharti Dental College, SVSU Maxillary second premolar Dr. Preeti Sharma, Subharti Dental College, SVSU Maxillary First Premolar Dr Preeti Sharma Reader Oral Pathology SDC Dr. Preeti Sharma, Subharti Dental College, SVSU The maxillary first premolar has two cusps, buccal and lingual. The buccal cusp is about 1mm longer than the lingual cusp. The crown is angular and buccal line angles are more prominent. The crown is shorter than the canine by 1.5 to 2mm on an average. The premolar resembles a canine from buccal aspect. -

Study of Root Canal Anatomy in Human Permanent Teeth
Brazilian Dental Journal (2015) 26(5): 530-536 ISSN 0103-6440 http://dx.doi.org/10.1590/0103-6440201302448 1Department of Stomatologic Study of Root Canal Anatomy in Human Sciences, UFG - Federal University of Goiás, Goiânia, GO, Brazil Permanent Teeth in A Subpopulation 2Department of Radiology, School of Dentistry, UNIC - University of Brazil’s Center Region Using Cone- of Cuiabá, Cuiabá, MT, Brazil 3Department of Restorative Dentistry, School of Dentistry of Ribeirão Beam Computed Tomography - Part 1 Preto, USP - University of São Paulo, Ribeirão Preto, SP, Brazil Carlos Estrela1, Mike R. Bueno2, Gabriela S. Couto1, Luiz Eduardo G Rabelo1, Correspondence: Prof. Dr. Carlos 1 3 3 Estrela, Praça Universitária s/n, Setor Ana Helena G. Alencar , Ricardo Gariba Silva ,Jesus Djalma Pécora ,Manoel Universitário, 74605-220 Goiânia, 3 Damião Sousa-Neto GO, Brasil. Tel.: +55-62-3209-6254. e-mail: [email protected] The aim of this study was to evaluate the frequency of roots, root canals and apical foramina in human permanent teeth using cone beam computed tomography (CBCT). CBCT images of 1,400 teeth from database previously evaluated were used to determine the frequency of number of roots, root canals and apical foramina. All teeth were evaluated by preview of the planes sagittal, axial, and coronal. Navigation in axial slices of 0.1 mm/0.1 mm followed the coronal to apical direction, as well as the apical to coronal direction. Two examiners assessed all CBCT images. Statistical data were analyzed including frequency distribution and cross-tabulation. The highest frequency of four root canals and four apical foramina was found in maxillary first molars (76%, 33%, respectively), followed by maxillary second molars (41%, 25%, respectively). -

The All-On-Four Treatment Concept: Systematic Review
J Clin Exp Dent. 2017;9(3):e474-88. All-on-four: Systematic review Journal section: Prosthetic Dentistry doi:10.4317/jced.53613 Publication Types: Review http://dx.doi.org/10.4317/jced.53613 The all-on-four treatment concept: Systematic review David Soto-Peñaloza 1, Regino Zaragozí-Alonso 2, María Peñarrocha-Diago 3, Miguel Peñarrocha-Diago 4 1 Collaborating Lecturer, Master in Oral Surgery and Implant Dentistry, Department of Stomatology, Faculty of Medicine and Dentistry, University of Valencia, Spain Peruvian Army Officer, Stomatology Department, Luis Arias Schreiber-Central Military Hospital, Lima-Perú 2 Dentist, Department of Stomatology, Faculty of Medicine and Dentistry, University of Valencia, Spain 3 Assistant Professor of Oral Surgery, Stomatology Department, Faculty of Medicine and Dentistry, University of Valencia, Spain 4 Professor and Chairman of Oral Surgery, Stomatology Department, Faculty of Medicine and Dentistry, University of Valencia, Spain Correspondence: Unidad de Cirugía Bucal Facultat de Medicina i Odontologìa Universitat de València Gascó Oliag 1 46010 - Valencia, Spain [email protected] Soto-Peñaloza D, Zaragozí-Alonso R, Peñarrocha-Diago MA, Peñarro- cha-Diago M. The all-on-four treatment concept: Systematic review. J Clin Exp Dent. 2017;9(3):e474-88. http://www.medicinaoral.com/odo/volumenes/v9i3/jcedv9i3p474.pdf Received: 17/11/2016 Accepted: 16/12/2016 Article Number: 53613 http://www.medicinaoral.com/odo/indice.htm © Medicina Oral S. L. C.I.F. B 96689336 - eISSN: 1989-5488 eMail: [email protected] Indexed in: Pubmed Pubmed Central® (PMC) Scopus DOI® System Abstract Objectives: To systematically review the literature on the “all-on-four” treatment concept regarding its indications, surgical procedures, prosthetic protocols and technical and biological complications after at least three years in function. -

Sensitive Teeth Sensitive Teeth Can Be Treated
FOR THE DENTAL PATIENT ... TREATMENT Sensitive teeth Sensitive teeth can be treated. Depending on the cause, your dentist may suggest that you try Causes and treatment desensitizing toothpaste, which contains com- pounds that help block sensation traveling from the tooth surface to the nerve. Desensitizing f a taste of ice cream or a sip of coffee is toothpaste usually requires several applications sometimes painful or if brushing or flossing before the sensitivity is reduced. When choosing makes you wince occasionally, you may toothpaste or any other dental care products, look have a common problem called “sensitive for those that display the American Dental Asso- teeth.” Some of the causes include tooth ciation’s Seal of Acceptance—your assurance that Idecay, a cracked tooth, worn tooth enamel, worn products have met ADA criteria for safety and fillings and tooth roots that are exposed as a effectiveness. result of aggressive tooth brushing, gum recession If the desensitizing toothpaste does not ease and periodontal (gum) disease. your discomfort, your dentist may suggest in- office treatments. A fluoride gel or special desen- SYMPTOMS OF SENSITIVE TEETH sitizing agents may be applied to the sensitive A layer of enamel, the strongest substance in the areas of the affected teeth. When these measures body, protects the crowns of healthy teeth. A layer do not correct the problem, your dentist may rec- called cementum protects the tooth root under the ommend other treatments, such as a filling, a gum line. Underneath the enamel and the crown, an inlay or bonding to correct a flaw or cementum is dentin, a part of the tooth that is decay that results in sensitivity. -

Original Article Concurrent Measurements of Danger Zone Anatomy in Mandibular First Molars Using Micro-Computed Tomography: a Pilot Study
Int J Clin Exp Med 2018;11(8):7692-7700 www.ijcem.com /ISSN:1940-5901/IJCEM0067321 Original Article Concurrent measurements of danger zone anatomy in mandibular first molars using micro-computed tomography: a pilot study Jiawei Lu1, Lizong Liang1, Jie Ran1, Gao Wu1, Chenghao Li2, Jianping Ge2, Jianxiang Tao1 Departments of 1Prosthodontics, 2Endodontics, School and Hospital of Stomatology, Tongji University, Shanghai Engineering Research Center of Tooth Restoration and Regeneration, Shanghai 20072, China Received October 16, 2017; Accepted May 9, 2018; Epub August 15, 2018; Published August 30, 2018 Abstract: The aim of this study is to describe the anatomical characteristics of the ‘danger zone’ in human mandibu- lar first molars by measuring the thickness of the bending point (point α) and the thinnest point (point β) of each root in human mandibular first molars. Eighteen mandibular first molars were scanned by micro-computed tomography and reconstructed three-dimensionally by Mimics Research 17.0. To identify characteristics of the ‘danger zone’, the actual root curvature, the minimal dentin thickness of the bending slice and the thinnest slice were selected as parameters. Furthermore, to describe the relationship of point α and point β, the distance between them was also measured. The results showed that the actual canal curvatures in the mandibular first molars were 5-10 degrees larger than those measured in 2-D images including X-ray or CBCT. The thinnest thickness of roots in all canals was less than 1 mm except the two distal roots of three-rooted mandibular first molars. Moreover, as for some two-rooted mandibular first molars, their point α and point β were located in the same furcation surface of root, the result might be coincident in the mesiolingual side; whereas for three-rooted mandibular first molars, the distal two canals were found significantly thicker than the mesial two (p<0.05). -

Anatomical Analysis of the Resected Roots of Mandibular First Molars After Failed Non-Surgical Retreatment
Restor Dent Endod. 2018 May;43(2):e16 https://doi.org/10.5395/rde.2018.43.e16 pISSN 2234-7658·eISSN 2234-7666 Research Article Anatomical analysis of the resected roots of mandibular first molars after failed non-surgical retreatment Jiyoung Yoon ,1 Byeong-Hoon Cho ,2 Jihyun Bae ,1 Yonghoon Choi 1* 1Department of Conservative Dentistry, Section of Dentistry, Seoul National University Bundang Hospital, Seongnam, Korea 2Department of Conservative Dentistry, Seoul National University School of Dentistry and Dental Research Institute, Seoul, Korea Received: Nov 29, 2017 ABSTRACT Accepted: Jan 26, 2018 Objectives: Yoon J, Cho BH, Bae J, Choi Y Understanding the reason for an unsuccessful non-surgical endodontic treatment outcome, as well as the complex anatomy of the root canal system, is very *Correspondence to important. This study examined the cross-sectional root canal structure of mandibular first Yong-Hoon Choi, DDS, MSD, PhD molars confirmed to have failed non-surgical root canal treatment using digital images Associate Professor, Department of Conservative Dentistry, Section of Dentistry, obtained during intentional replantation surgery, as well as the causative factors of the failed Seoul National University Bundang Hospital, conventional endodontic treatments. 82 Gumi-ro 173-beon-gil, Bundang-gu, Materials and Methods: This study evaluated 115 mandibular first molars. Digital Seongnam 13620, Korea. photographic images of the resected surface were taken at the apical 3 mm level and E-mail: [email protected] examined. The discolored dentin area around the root canal was investigated by measuring Copyright © 2018. The Korean Academy of the total surface area, the treated areas as determined by the endodontic filling material, and Conservative Dentistry the discolored dentin area. -

Comparative Morphology of Incisor Enamel and Dentin in Humans and Fat Dormice (Glis Glis)
Coll. Antropol. 27 (2003) 1: 373–380 UDC 572.72:616.314.11 Original scientific paper Comparative Morphology of Incisor Enamel and Dentin in Humans and Fat Dormice (Glis glis) Dean Konjevi}1, Tomislav Keros2, Hrvoje Brki}3, Alen Slavica1, Zdravko Janicki1 and Josip Margaleti}4 1 Chair for Game Biology, Pathology and Breeding, Veterinary Faculty, University of Zagreb, Zagreb, Croatia 2 Croatian Veterinary Institute, Zagreb, Croatia 3 Department for Dental Anthropology, School of Dental Medicine, University of Zagreb, Zagreb, Croatia 4 Department of Forest Protection and Wildlife Management, Faculty of Forestry, University of Zagreb, Zagreb, Croatia ABSTRACT The structure of teeth in all living beings is genetically predetermined, although it can change under external physiological and pathological factors. The author’s hypoth- esis was to indicate evolutional shifts resulting from genetic, functional and other dif- ferences. A comparative study about certain characteristics of incisors in humans and myomorpha, the fat dormouse (Glis glis) being their representative as well, comprised measurements of enamel and dentin thickness in individual incisor segments, evalua- tion of external enamel index, and also assessment of histological structure of enamel and dentin. The study results involving dormice showed the enamel to be thicker in lower than in the upper teeth, quite contrary to enamel thickness in humans. In the up- per incisors in dormice the enamel is the thickest in the medial layer of the crown, and in the cervical portion of the crown in the lower incisors. The thickness of dentin in dor- mice is greater in the oral than in the vestibular side. These findings significantly differ from those reported in reference literature, but they are based on the function of teeth in dormice. -

Bonding to Enamel and Dentin
Chapter 16 Bonding to Enamel and Dentin INTRODUCTION • Evolution of Dentin Bonding Agents ADHESIVE DENTISTRY • Nanofilled Bonding Agents • Indications for Use of Adhesives HYBRID LAYER AND HYBRIDIZATION • Advantages of Bonding Techniques • Hybridization (Given by Nakabayachi in 1982) • Mechanism of Adhesion • Zones of Hybrid Layer • Factors Affecting Adhesion SMEAR LAYER ENAMEL BONDING • Structure • Steps for Enamel Bonding • Formation of Smear Layer • Mechanism of Etching • Components of Smear Layer DENTIN BONDING • Role of Smear Layer • Conditioning of Dentin • Role of Smear Layer in Dentin Bonding • Priming of Dentin • Classification of Modern Adhesives • Moist vs Dry Dentin GLASS IONOMER BASED ADHESIVE SYSTEM DENTIN BONDING AGENT • Steps • Mechanism of Bonding FAILURE OF DENTIN BONDING INTRODUCTION fluid present in dentinal tubules makes the bonding difficult. The adhesion to dentin requires decalcification The traditional “drill and fill” approach is fading now of the dentinal surface to expose a layer of interlacing because of numerous advancements taking place in collagen fibrils and the entrances of the dentinal tubules. restorative dentistry. For a restorative material, adhesion When resins are used, they form an intermediate layer is the primary requirement so that restorative materials with exposed spongy collagen network which can be then can be bonded to enamel or dentin and without the need bonded to the retentive inner surface of the restoration of extensive tooth preparation. The initial advancement by means of a resin similar to that of enamel bonding. was made in 1956, by a pedodontist, Buonocore, who The past decade has seen increased use of bonding developed acid etching of the enamel. He showed that agents in concurrence with traditional dental materials. -
Anatomical Landmarks in Order to Study an Individual Tooth Intelligently, We Must Be Able to Recognize All Landmarks of Importance by Name
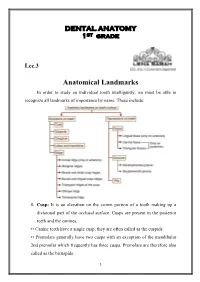
DENTAL ANATOMY 1ST grade Lec.3 Anatomical Landmarks In order to study an individual tooth intelligently, we must be able to recognize all landmarks of importance by name. These include: 1. Cusp: It is an elevation on the crown portion of a tooth making up a divisional part of the occlusal surface. Cusps are present in the posterior teeth and the canines. •• Canine teeth have a single cusp; they are often called as the cuspids. •• Premolars generally have two cusps with an exception of the mandibular 2nd premolar which frequently has three cusps. Premolars are therefore also called as the bicuspids. 1 •• Maxillary and mandibular 1st molars have five cusps, while other molars generally have four cusps. Each cusp is a gothic pyramid with four sides formed by four ridges that run down from the cusp tip: •• Mesial and distal cusp ridges (cusp slopes) •• Buccal/lingual cusp ridge •• Triangular ridge of the cusp. There are two cusp slopes on either side of the triangular ridge. In case of canines, there is a labial ridge analogous to the buccal ridge posterior teeth; there is a lingual ridge analogous to triangular ridge of posterior teeth. In the Table below the Number of cusps in different types of teeth: Tooth type Maxillary arch Mandibular arch Incisors 0 0 Canines 1 1 Premolars 2 2 in 1st premolar 3 or 2 in 2nd premolar Molars 1st molar 4 +1 accessory cusp 5 (cusp of Carabelli) 2nd molar 4 4 3rd molar 4 or 3 4 or 5 A cusp is named according to its location on the tooth.