VARIATIONS in SUBSCAPULAR ARTERY: a STUDY Pushpalatha M1, Chitra N2
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Variation of the Origin of the Lateral Thoracic Artery. Case Report
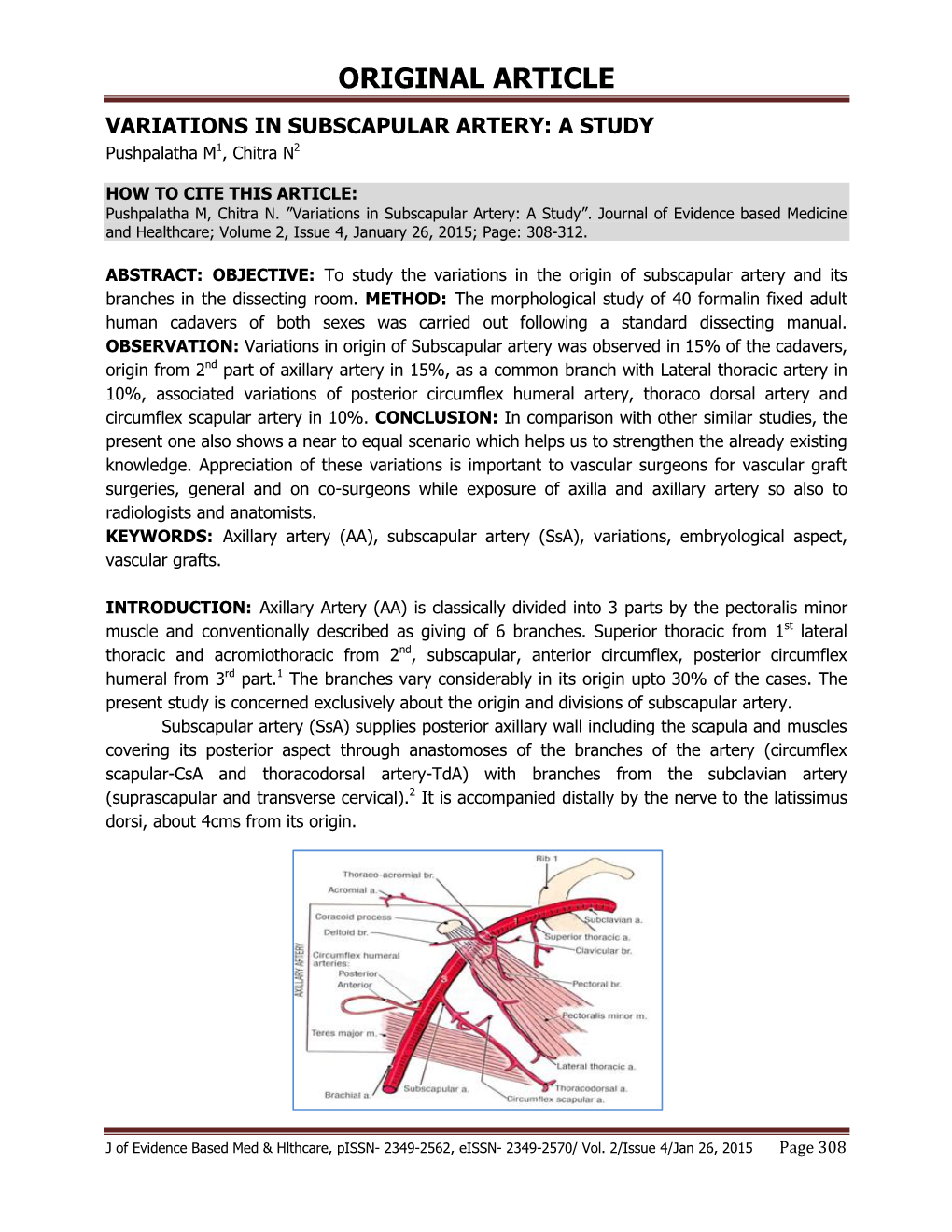
Revista Română de Anatomie funcţională şi clinică, macro- şi microscopică şi de Antropologie Vol. XVII – Nr. 4 – 2018 CLINICAL ANATOMY VARiation OF THE ORIGin OF THE LatERAL THORacic ARTERY. CASE REPORT Tamás-Csaba Sipos2, Lóránd Dénes1*, Klara Brînzaniuc1, Annamária Szántó1, Zoltán Pávai1, Zsuzsánna Pap1 University of Medicine, Pharmacy, Sciences and Technology of Tîrgu-Mureş 1. Department of Anatomy and Embryology 2. Student, GM 6th year VARIATION OF THE ORIGIN OF THE LATERAL THORACIC ARTERY. Case RePORT (Abstract): Introduction: Anatomical variations of the origin of axillary artery branches are quite common. The most frequent variations are common trunks or emergence from a different segment than the classical description. Material and method: A formalin fixed male human cadaver has been dissected during teaching classes for medical students at the Anatomy and Embryology De- partment of UMFST Târgu Mureş. We observed a pattern of origins of the axillary artery branch- es different from the classical description. Results: The second part of the axillary artery provides the superior thoracic artery and the thoraco-acromial artery from its anterior surface, while the subscapular artery separates from its posterior surface. The lateral thoracic artery is a branch of the subscapular artery. The anterior and posterior circumflex humeral arteries come from the third part of the axillary artery, which corresponds to the classical description. Conclusions: Published studies report multiple variations regarding the origin of the axillary artery branches. Most com- monly, the lateral thoracic artery originates from the subscapular artery, which is the case in our study as well. Key-words: LATERAL THORACIC ARTERY, vaRIATION, SUBSCAPULAR ARTERY INTRODUCTION provides six branches, which are grouped ac- Arterial supply to the thoraco-scapulo-hu- cording to its parts: the first part gives off the meral area is provided by the branches of the superior thoracic artery, the second part pro- axillary artery. -

A High Origin Subscapular Trunk and Its Clinical Implications
ogy iol : Cu ys r h re P n t & R Anatomy & Physiology: Current y e s m e o a t Ariyo, Anat Physiol 2018, 8:2 r a c n h A Research DOI: 10.4172/2161-0940.1000296 ISSN: 2161-0940 Case Report Open Access A High Origin Subscapular Trunk and its Clinical Implications Olutayo Ariyo* Department of Pathology Anatomy and Cell Biology, SKMC, Thomas Jeffesron University, Philadelpphia, PA United States *Corresponding author: Olutayo Ariyo, Department of Pathology Anatomy and Cell Biology, SKMC, Thomas Jeffesron University, Philadelpphia, PA United States, Tel: 610-638-9278; E-mail: [email protected] Received date: May 07, 2018; Accepted date: May 24, 2018; Published date: May 28, 2018 Copyright: © 2018 Ariyo O. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Abstract Important variations in the arrangement of branches of the axillary artery revolve around the origin of the subscapular artery. The case of a "high origin" subscapular artery as a common trunk to lateral thoracic, common circumflex humeral trunk in the left upper limb of a 72 year-old female cadaver, is discussed. This variant trunk originated posterior to the pectoralis minor muscle about 2-3 cm posteroinferior to that of the thoracoaromial artery. Trunk formations in the axillary artery with four or more branches sharing a common stem of origin are infrequent compared with those with fewer numbers. In certain surgical orthopedic procedures, surgeons sometimes administer a ligature in the 3rd part of the artery, relying on a suprascapular/dorsal scapular-circumflex scapular colateral pathway to dump blood into the artery distal to the ligature. -

Arterial Supply to the Rotator Cuff Muscles
Int. J. Morphol., 32(1):136-140, 2014. Arterial Supply to the Rotator Cuff Muscles Suministro Arterial de los Músculos del Manguito Rotador N. Naidoo*; L. Lazarus*; B. Z. De Gama*; N. O. Ajayi* & K. S. Satyapal* NAIDOO, N.; LAZARUS, L.; DE GAMA, B. Z.; AJAYI, N. O. & SATYAPAL, K. S. Arterial supply to the rotator cuff muscles.Int. J. Morphol., 32(1):136-140, 2014. SUMMARY: The arterial supply to the rotator cuff muscles is generally provided by the subscapular, circumflex scapular, posterior circumflex humeral and suprascapular arteries. This study involved the bilateral dissection of the scapulohumeral region of 31 adult and 19 fetal cadaveric specimens. The subscapularis muscle was supplied by the subscapular, suprascapular and circumflex scapular arteries. The supraspinatus and infraspinatus muscles were supplied by the suprascapular artery. The infraspinatus and teres minor muscles were found to be supplied by the circumflex scapular artery. In addition to the branches of these parent arteries, the rotator cuff muscles were found to be supplied by the dorsal scapular, lateral thoracic, thoracodorsal and posterior circumflex humeral arteries. The variations in the arterial supply to the rotator cuff muscles recorded in this study are unique and were not described in the literature reviewed. Due to the increased frequency of operative procedures in the scapulohumeral region, the knowledge of variations in the arterial supply to the rotator cuff muscles may be of practical importance to surgeons and radiologists. KEY WORDS: Arterial supply; Variations; Rotator cuff muscles; Parent arteries. INTRODUCTION (Abrassart et al.). In addition, the muscular parts of infraspinatus and teres minor muscles were supplied by the circumflex scapular artery while the tendinous parts of these The rotator cuff is a musculotendionous cuff formed muscles received branches from the posterior circumflex by the fusion of the tendons of four muscles – viz. -

Arteries of The
This document was created by Alex Yartsev ([email protected]); if I have used your data or images and forgot to reference you, please email me. Arteries of the Arm st The AXILLARY ARTERY begins at the border of the 1 rib as a continuation of the subclavian artery Subclavian artery The FIRST PART stretches between the 1st rib and the medial border of pectoralis minor. First rib It has only one branch – the superior thoracic artery Superior thoracic artery The SECOND PART lies under the pectoralis Thoracoacromial artery minor; it has 2 branches: Which pierces the - The Thoracoacromial artery costocoracoid membrane - The Lateral Thoracic artery deep to the clavicular head The THIRD PART stretches from the lateral border of pectoralis major of pectoralis minor to the inferior border of Teres Major; it has 3 branches: Pectoralis major - The Anterior circumflex humeral artery - The Posteror circumflex humeral artery Pectoralis minor - The Subscapular artery Axillary nerve Posterior circumflex humeral artery Lateral Thoracic artery Travels through the quadrangular space together Which follows the lateral with the axillary nerve. It’s the larger of the two. border of pectoralis minor onto the chest wall Anterior circumflex humeral artery Passes laterally deep to the coracobrachialis and Circumflex scapular artery the biceps brachii Teres Major Passes dorsally between subscapularis and teres major to supply the dorsum of the scapula Profunda Brachii- deep artery of the arm Thoracodorsal artery Passes through the lateral triangular space (with Goes to the inferior angle of the scapula, the radial nerve) into the posterior compartment Triceps brachii supplies mainly the latissimus dorsi of the arm. -

Superficial Brachial Artery: a Possible Cause for Idiopathic Median Nerve Entrapment Neuropathy P
CORE Metadata, citation and similar papers at core.ac.uk Provided by Via Medica Journals Folia Morphol. Vol. 76, No. 3, pp. 527–531 DOI: 10.5603/FM.a2017.0013 C A S E R E P O R T Copyright © 2017 Via Medica ISSN 0015–5659 www.fm.viamedica.pl Superficial brachial artery: a possible cause for idiopathic median nerve entrapment neuropathy P. Nkomozepi, N. Xhakaza, E. Swanepoel Department of Human Anatomy and Physiology, Faculty of Health Sciences, University of Johannesburg, Johannesburg, Gauteng, South Africa [Received: 29 November 2016; Accepted: 4 January 2017] Nerve entrapment syndromes occur because of anatomic constraints at specific locations in both upper and lower limbs. Anatomical locations prone to nerve entrapment syndromes include sites where a nerve courses through fibro-osseous or fibromuscular tunnels or penetrates a muscle. The median nerve (MN) can be entrapped by the ligament of Struthers; thickened biceps aponeurosis; between the superficial and deep heads of the pronator teres muscle and by a thickened proximal edge of flexor digitorum superficialis muscle. A few cases of MN neu- ropathies encountered are reported to be idiopathic. The superficial branchial artery (SBA) is defined as the artery running superficial to MN or its roots. This divergence from normal anatomy may be the possible explanation for idiopathic MN entrapment neuropathy. This study presents three cases with unilateral presence of the SBA encountered during routine undergraduate dissection at the University of Johannesburg. Case 1 — SBA divided into radial and ulnar arteries. Brachial artery (BA) terminated as deep brachial artery. Case 2 — SBA continued as radial artery (RA). -

Variations in the Axillary Artery Branching Pattern Anatomy Section
DOI: 10.7860/JCDR/2020/44533.13887 Case Report Variations in the Axillary Artery Branching Pattern Anatomy Section DEEPSHIKHA SINGH1, MINAKSHI MALHOTRA2, SNEH AGARWAL3 ABSTRACT Variations in axillary artery branching pattern can lead to iatrogenic injuries during invasive procedures. Knowledge of the same is critical to prevent such events. Multiple bilateral variations were observed in the branching pattern of axillary artery. These variations were noted in a female cadaver, during routine undergraduate dissection in September 2019 in Lady Hardinge Medical College, New Delhi. On the left side, an anomalous branch running with the medial pectoral nerve was found. A common stem arising from the 2nd part of left axillary artery divided to give the lateral thoracic artery, the subscapular artery and an alar artery. Another alar branch arose from the left subscapular artery before it bifurcated into thoraco-dorsal and circumflex scapular arteries. The right axillary artery gave an aberrant branch proximal to the lateral thoracic artery. A common trunk arising from the 2nd part of right axillary branched out to give the posterior circumflex humeral artery, the subscapular artery and an alar artery. The brachial artery divided 13.5 cm proximal to the intercondylar line of humerus on the left and 14.4 cm on the right side. On both sides, the ulnar artery arose proximally and the radial and common inter-osseous arteries continued as a common trunk and divided distally. This case study reports multiple bilateral axillary artery anomalies and complements to the existing knowledge of vascular anomalies. Comprehensive knowledge of these variations is essential from anatomical, radiological and surgical point of view. -

THORACODORSAL ARTERY SCAPULAR TIP (TDAST) FLAP for HEAD and NECK RECONSTRUCTION Douglas Chepeha
OPEN ACCESS ATLAS OF OTOLARYNGOLOGY, HEAD & NECK OPERATIVE SURGERY THORACODORSAL ARTERY SCAPULAR TIP (TDAST) FLAP FOR HEAD AND NECK RECONSTRUCTION Douglas Chepeha The thoracodorsal artery scapular tip flap is Benefits of TDAST the osseous (bone) component of the latissi- mus dorsi flap. The thoracodorsal artery • Long vascular pedicle 1,2 supplies the scapular tip and the latissimus • Triangular 3-dimensional shape 2 dorsi muscle (with overlying skin). There- • Bone paddle easily shaped without fore, the scapular tip can be harvested as an osteotomy to reconstruct the infrastruc- independent osseous paddle or with the ture of the maxilla 3 latissimus dorsi muscle or with the latissi- • Bone is surrounded by attached muscle mus dorsi muscle and overlying skin or in that can be used to help close defects of some combination with the serratus muscle. maxillary and mandibular alveolus bone There are many possible combinations of • Can be harvested as a chimeric flap with skin, muscle and bone paddles that make a variety of skin and muscle paddle this arterial donor system valuable for head options 3-5 and neck reconstruction. In addition, the • Independently mobile skin paddle 2,3 thoracodorsal arterial system can be com- • Thoracodorsal artery and vein are large bined with the circumflex scapular arterial vessels and most commonly connect to system (both arteries arise from the sub- larger subscapular vessels scapular system or are directly adjacent to one another) to further increase the skin and Caveats of TDAST bone paddle options. Although it would not always be ideal, this donor site could be • Overall harvest is manageable but one used to reconstruct all defects in the head must exercise caution with the identifi- and neck. -
Unilateral Double Axillary and Double Brachial Arteries. Embryological Basis and Clinical Implications
Int. J. Morphol., Case report 24(3):463-468, 2006. Unilateral Double Axillary and Double Brachial Arteries. Embryological Basis and Clinical Implications Arterias Axilar y Braquial Dobles Unilaterales. Bases Embriológicas e Implicaciones Clínicas Jayakumari, S.; Gayatri Rath & Jyoti Arora JAYAKUMARI, S.; RATH, G. & ARORA, J. Unilateral double axillary and double brachial arteries. Embryological basis and clinical implications. Int. J. Morphol., 24(3):463-468, 2006. SUMMARY: This report presents double axillary and double brachial arteries on the right side of an adult male cadaver. In this case, the right axillary artery bifurcated into axillary artery I and axillary artery II posterior to the pectoralis minor muscle. Both the axillary arteries with their branches traversed upto lower border of teres major muscle and continued further as seperate entities into the cubital fossa as brachial artery I and brachial artery II respectively. The axillary artery I which continued as brachial artery I was super- ficial and tortuous in its course, while the axillary artery II was slender and deeply situated. The thoraco-acromial, lateral thoracic and subscapular arteries took origin from axillary artery I. The superior thoracic artery was seen arising from the thoraco-acromial artery. The anterior and posterior circumflex humeral arteries arose from axillary artery II.The profunda brachii artery was given off by the brachial artery II, while at the level of intercondylar line, the ulnar artery was given off by brachial artery I. In the cubital fossa, the brachial artery it divided into radial and common interosseous artery, while the brachial artery II ended by anastomosis with brachial artery I. -
Arteries of the Upper Limb (Shoulder, Arms & Hands) the Blood Supply to the Upper Limb (Shoulder, Arm and Hand) Starts As the Subclavian Arteries in the Shoulders
Arteries of the Upper Limb (Shoulder, Arms & Hands) The blood supply to the upper limb (shoulder, arm and hand) starts as the subclavian arteries in the shoulders. As each artery passes into the axilla (armpit) it becomes the: > axillary artery supplies blood, through several small branches, to the axilla, chest wall, shoulder joint, scapula, and regional muscles. Axillary artery branches include: – supreme thoracic artery supplies blood to the upper chest. – thoracoacromial trunk supplies blood to the deltoid and pectoral region. – lateral thoracic artery supplies blood to the lateral thorax (chest wall). – subscapular artery supplies blood to the muscles of the scapula and latissimus dorsi. – anterior humeral circumflex and posterior humeral circumflex artery supply blood to the head of the humerus, deltoid and teres minor muscle. > As the axillary artery emerges from the axilla into the arm it is now called the brachial artery. > brachial artery runs down medial humerus to supply blood to anterior flexor muscles. > deep brachial artery branches off to supply blood to the triceps. At the elbow, small branches anastomose around the elbow joint. Below the elbow, the brachial artery splits into the radial and ulnar arteries. > radial artery supplies blood to the lateral muscles of the forearm, wrist, thumb and later half of the index finger. It creates the wrist pulse. > ulnar artery supplies blood to the medial forearm, and fingers 3-5 and the medial half of the index finger. > The ulnar artery gives off the common interosseus artery which supplies blood to the to the deep flexors and extensors. > In the palm, the radial and ulnar arteries anatomose to form the palmar arches. -
The Pectoral Branch Arising from the Subscapular Artery: Case Report of a Rare Variation
Forensic Medicine and Anatomy Research, 2016, 4, 41-45 http://www.scirp.org/journal/fmar ISSN Online: 2327-4107 ISSN Print: 2327-4115 The Pectoral Branch Arising from the Subscapular Artery: Case Report of a Rare Variation Jae-Hee Park, Jae-Ho Lee, In-Jang Choi Department of Anatomy, School of Medicine, Keimyung University, Daegu, Republic of Korea How to cite this paper: Park, J.-H., Lee, Abstract J.-H. and Choi, I.-J. (2016) The Pectoral Branch Arising from the Subscapular Ar- Variations in the upper limbs are common and are the main causes for iatro- tery: Case Report of a Rare Variation. Fo- genic injury during invasive procedures. A rare division of the axillary artery rensic Medicine and Anatomy Research, 4, was found on the left side of a Korean cadaver during an educational dissec- 41-45. tion. The subscapular artery originated from the second part of the axillary http://dx.doi.org/10.4236/fmar.2016.44008 artery. And then it gave off an aberrant branch to the pectoralis major muscle, Received: December 19, 2016 as pectoral branch. The author describes this previously unreported case and Accepted: January 6, 2017 discusses its prevalence and the clinical implications. Published: January 9, 2017 Keywords Copyright © 2016 by authors and Scientific Research Publishing Inc. Axillary Artery, Subscapular Artery, Thoracoacromial Artery, Variation This work is licensed under the Creative Commons Attribution International License (CC BY 4.0). http://creativecommons.org/licenses/by/4.0/ 1. Introduction Open Access The axillary artery, the continuation of the subclavian artery, begins at the lateral border of the first rib, and after passing the lower margin of the teres major muscle, it becomes the brachial artery. -

Multiple Arterial Anomalies in Upper Limb
Kathmandu University Medical Journal (2009), Vol. 7, No. 3, Issue 27, 293-297 Case Note Multiple arterial anomalies in upper limb Baral P1, Vijayabhaskar P2, Roy S1, Kumar S2, Ghimire S3, Shrestha U3 1Lecturer, 2Assistant Professor, Department of Anatomy, Manipal College of Medical Sciences, Pokhara, Nepal, 3Post-graduate students, Department of Anatomy, B.P. Koirala Institute of Health Sciences, Dharan, Nepal. Abstract An isolated neurovascular variation is common but multiple vascular anomalies on same upper limb is a very rare case. We observed an unusual variations in right upper limb during routine dissection of a Nepali cadaver . The variations were observed in Axilla, Forearm and Palm. In axilla, fi rst part of axillary artery did not give any branch, the second part of axillary artery gave off only two branches - (a) thoracoacromial artery and (b) a large common trunk which later gave off lateral thoracic, thoracodorsal, subscapular, posterior circumfl ex scapular and then continued as posterior circumfl ex humeral artery. The third part of axillary artery gave off only anterior circumfl ex humeral artery. In forearm, the ulnar artery runs downward superfi cial to fl exor muscles. Here, radial artery gave off common interosseous artery. In palm radial artery did not give any contribution to superfi cial palmar arch which is solely formed by the continuation of ulnar artery. This type of anomalies are very rare and is not reported in Nepalese cadaver at all. These anomalies are described in detail and their clinical relevance is highlighted. Key words : Axillary artery, Brachial artery, Radial artery, Ulnar artery, Palmar arch, Variations he arterial system of upper limb begins with the orthopaedic surgeons, plastic surgeons, radiologists and Taxillary artery, a continuation of subclavian artery anatomists. -

Redalyc.Anomalous Origin of the Deep Brachial Artery (Profunda Brachii
Jornal Vascular Brasileiro ISSN: 1677-5449 [email protected] Sociedade Brasileira de Angiologia e de Cirurgia Vascular Brasil Cisne de Paula, Rafael; Erthal, Rafael; Mota Pacheco Fernandes, Rodrigo; Babinski, Marcio Antônio; Silva, Julio Guilherme; Araujo Chagas, Carlos Alberto Anomalous origin of the deep brachial artery (profunda brachii) observed in bilateral arms: case report Jornal Vascular Brasileiro, vol. 12, núm. 1, enero-marzo, 2013, pp. 53-56 Sociedade Brasileira de Angiologia e de Cirurgia Vascular São Paulo, Brasil Available in: http://www.redalyc.org/articulo.oa?id=245025771011 How to cite Complete issue Scientific Information System More information about this article Network of Scientific Journals from Latin America, the Caribbean, Spain and Portugal Journal's homepage in redalyc.org Non-profit academic project, developed under the open access initiative C A S E REPORT Anomalous origin of the deep brachial artery (profunda brachii) observed in bilateral arms: case report Origem anômala da artéria braquial profunda (profunda brachii) observada em braços bilaterais: relato de caso Rafael Cisne de Paula1, Rafael Erthal2, Rodrigo Mota Pacheco Fernandes2, Marcio Antônio Babinski2, Julio Guilherme Silva3, Carlos Alberto Araujo Chagas4 Abstract During an ordinary dissection, a cadaver showed a bilateral anomalous origin of the deep brachial artery, where this vessel appeared like a branching of the subscapular artery with common trunk, which included the posterior circumflex humeral artery. The course and distribution of the deep brachial artery in the back compartment were relatively consistent with previous reports. Arterial variations can be damaged through iatrogenic means if not properly documented. The knowledge of this case is very important in clinical medicine and in surgeries in this compartment to prevent any injury.