O422 Geretti 012.Pdf
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Croi 2021 Program Committee
General Information CONTENTS WELCOME . 2 General Information General Information OVERVIEW . 2 CONTINUING MEDICAL EDUCATION . 3 CONFERENCE SUPPORT . 4 VIRTUAL PLATFORM . 5 ON-DEMAND CONTENT AND WEBCASTS . 5 CONFERENCE SCHEDULE AT A GLANCE . 6 PRECONFERENCE SESSIONS . 9 LIVE PLENARY, ORAL, AND INTERACTIVE SESSIONS, AND ON-DEMAND SYMPOSIA BY DAY . 11 SCIENCE SPOTLIGHTS™ . 47 SCIENCE SPOTLIGHT™ SESSIONS BY CATEGORY . 109 CROI FOUNDATION . 112 IAS–USA . 112 CROI 2021 PROGRAM COMMITTEE . 113 Scientific Program Committee . 113 Community Liaison Subcommittee . 113 Former Members . 113 EXTERNAL REVIEWERS . .114 SCHOLARSHIP AWARDEES . 114 AFFILIATED OR PROXIMATE ACTIVITIES . 114 EMBARGO POLICIES AND SOCIAL MEDIA . 115 CONFERENCE ETIQUETTE . 115 ABSTRACT PROCESS Scientific Categories . 116 Abstract Content . 117 Presenter Responsibilities . 117 Abstract Review Process . 117 Statistics for Abstracts . 117 Abstracts Related to SARS-CoV-2 and Special Study Populations . 117. INDEX OF SPECIAL STUDY POPULATIONS . 118 INDEX OF PRESENTING AUTHORS . .122 . Version 9 .0 | Last Update on March 8, 2021 Printed in the United States of America . © Copyright 2021 CROI Foundation/IAS–USA . All rights reserved . ISBN #978-1-7320053-4-1 vCROI 2021 1 General Information WELCOME TO vCROI 2021 Welcome to vCROI 2021! The COVID-19 pandemic has changed the world for all of us in so many ways . Over the past year, we have had to put some of our HIV research on hold, learned to do our research in different ways using different tools, to communicate with each other in virtual formats, and to apply the many lessons in HIV research, care, and community advocacy to addressing the COVID-19 pandemic . Scientists and community stakeholders who have long been engaged in the endeavor to end the epidemic of HIV have pivoted to support and inform the unprecedented progress made in battle against SARS-CoV-2 . -

Current Perspectives in HIV Post-Exposure Prophylaxis
HIV/AIDS–Research and Palliative Care Dovepress open access to scientific and medical research Open Access Full Text Article REVIEW Current perspectives in HIV post-exposure prophylaxis Binta Sultan1,2 Abstract: The incidence of human immunodeficiency virus (HIV) infection continues to rise Paul Benn1 among core groups and efforts to reduce the numbers of new infections are being redoubled. Laura Waters1 Post-exposure prophylaxis (PEP) is the use of short-term antiretroviral therapy (ART) to reduce the risk of acquisition of HIV infection following exposure. Current guidelines recommend a 1Department of Genitourinary Medicine, Mortimer Market Centre, 28-day course of ART within 36–72 hours of exposure to HIV. As long as individuals continue Central and North West London to be exposed to HIV there will be a role for PEP in the foreseeable future. Nonoccupational NHS Foundation Trust, London, UK; PEP, the vast majority of which is for sexual exposure (PEPSE), has a significant role to play in 2Centre for Sexual Health and HIV Research, University College London, HIV prevention efforts. Awareness of PEP and its availability for both clinicians and those who London, UK are eligible to receive it are crucial to ensure that PEP is used to its full potential in any HIV For personal use only. prevention strategy. In this review, we provide current evidence for the use of PEPSE, assessment of the risk of HIV transmission, indications for PEP, drug regimens, and management of patients started on PEP. We summarize national and international guidelines for the use of PEPSE. We explore the place of PEP within the wider strategy of reducing HIV incidence rates in the era of treatment as prevention and pre-exposure prophylaxis. -

A Phase IV, Double-Blind, Multicentre, Randomized, Placebo-Controlled
A phase IV, double-blind, multicentre, randomized, placebo-controlled, pilot study to assess the feasibility of switching individuals receiving efavirenz with continuing central nervous system adverse events to etravirine Laura Watersa, Martin Fisherb, Alan Winstonc, Chris Higgsa, Wendy Hadleyb, Lucy Garveyc, Sundhiya Mandaliaa, Nicky Perryb, Nicola Mackiec and Mark Nelsona Background: Two nucleoside reverse transcriptase inhibitors (NRTIs) and efavirenz (EFV) is a recommended initial regimen for HIV-1. Most EFV-related central nervous system (CNS) toxicity resolves early though symptoms may persist; we studied switching to etravirine (ETR) in these individuals. Methods: A randomized, double-blind trial in patients with viral suppression but ongoing CNS adverse events after more than 12 weeks EFV. Patients received 2NRTI/EFV/ETR-placebo (delayed switch) or 2NRTI/ETR/EFV-placebo (immediate switch) for 12 weeks followed by 12-week open-label phase (2NRTI/ETR). Primary end-point was percentage with G2-4 CNS adverse events at 12 weeks. Results: Thirty-eight men; 20/18 were randomized to immediate switch/delayed switch; median CD4 was 444/498 cells/ml, respectively. Baseline CNS adverse events were similar. Nineteen immediate switch patients completed follow-up (one lost to follow-up) and 13 on delayed switch (two lost to follow-up, two withdrawn consent, one adverse event). Immediate switch G2-4 CNS adverse event: 90% at baseline, 60% at week 12 (P ¼ 0.041). Delayed switch G2-4 CNS adverse event: 88.9% at baseline, 81.3% at week 12 (P ¼ ns). Combined (both arms) percentage decline in G2-4 CNS adverse event after 12 weeks of ETR was significant for overall adverse events, insomnia, abnormal dreams and nervousness (P ¼ 0.009, 0.016, 0.001, and 0.046, respectively). -

Consensus Statement on the Role of Health Systems in Advancing the Long-Term Well-Being of People Living with HIV ✉ Jeffrey V
PERSPECTIVE https://doi.org/10.1038/s41467-021-24673-w OPEN Consensus statement on the role of health systems in advancing the long-term well-being of people living with HIV ✉ Jeffrey V. Lazarus 1 , Kelly Safreed-Harmon1, Adeeba Kamarulzaman2,3, Jane Anderson4, Ricardo Baptista Leite5, Georg Behrens 6, Linda-Gail Bekker7, Sanjay Bhagani 8, Darren Brown 9, Graham Brown 10, Susan Buchbinder11, Carlos Caceres 12, Pedro E. Cahn13, Patrizia Carrieri 14, Georgina Caswell15, Graham S. Cooke 16, Antonella d’Arminio Monforte 17, Nikos Dedes18, 1234567890():,; Julia del Amo19, Richard Elliott 20, Wafaa M. El-Sadr21, María José Fuster-Ruiz de Apodaca 22,23, Giovanni Guaraldi 24, Tim Hallett 16, Richard Harding 25, Margaret Hellard 26, Shabbar Jaffar27, Meaghan Kall28, Marina Klein 29, Sharon R. Lewin 30,31,32, Ken Mayer33, Jose A. Pérez-Molina 34, Doreen Moraa35, Denise Naniche 1, Denis Nash36, Teymur Noori 37, Anton Pozniak 9,38, Reena Rajasuriar2, Peter Reiss39, Nesrine Rizk 40, Jürgen Rockstroh41, Diana Romero 36, Caroline Sabin 42, David Serwadda43 & Laura Waters 44 Health systems have improved their abilities to identify, diagnose, treat and, increasingly, achieve viral suppression among people living with HIV (PLHIV). Despite these advances, a higher burden of multimorbidity and poorer health-related quality of life are reported by many PLHIV in comparison to people without HIV. Stigma and discrimination further exacerbate these poor outcomes. A global multidisciplinary group of HIV experts developed a consensus statement identifying key issues that health systems must address in order to move beyond the HIV field’s longtime emphasis on viral suppression to instead deliver integrated, person- centered healthcare for PLHIV throughout their lives. -
UK Guideline for the Use of HIV Post-Exposure Prophylaxis 2021
UK Guideline for the use of HIV Post-Exposure Prophylaxis 2021 Guideline writing group Consultant Occupational Physician Kaveh Asanati Honorary Clinical Senior Lecturer, National Heart & Lung Institute, Imperial College London Consultant Physician Royal Free Hospital, London Sanjay Bhagani Senior Lecturer, Institute for Global Health, University College London Consultant Physician Chelsea and Westminster Hospital, London Marta Boffito Reader, Imperial College London Specialist Registrar, Brighton and Sussex University Hospital, Brighton Fiona Cresswell (Chair) Clinical PhD Fellow, London School of Hygiene and Tropical Medicine Valerie Delpech Consultant Epidemiologist, Public Health England Specialist Registrar, Hospital for Tropical Diseases, University College London Hospitals NHS Jayne Ellis Foundation Trust, London, UK Consultant HIV Medicine and Clinical Trials, Guy’s and St Thomas’ Hospital Julie Fox Honorary Reader Kings College London Linda Furness Sexual Health Adviser, Cardiff Royal Infirmary British HIV Association Guideline Committee Nadi Gupta Consultant HIV and Sexual Health, Rotherham NHS Foundation Trust British Association of Sexual Health and HIV Clinical Effectiveness Group Margaret Kingston Consultant Physician, Manchester Royal Infirmary. Honorary Chair Manchester University Consultant Occupational Physician Massoud Mansouri Deputy Course Director in Occupational Health, School of Medicine, Cardiff University Amanda Samarawickrama Consultant HIV and Sexual Health, Sexual Health South West London Kat Smithson National -

(BHIVA) & the British Association for Sexual Health & HIV (BASHH) 19
5th Joint Conference of the British HIV Association (BHIVA) & The British Association for Sexual Health & HIV (BASHH) 19 – 21 April 2021 - DIGITAL CONFERENCE PROGRAMME Monday 19th April - HIV Day 08:30 – 08:40 Welcome & Introduction by the Chair of BHIVA & Chair of BASHH Dr Laura Waters, Mortimer Market Centre, London Dr John McSorley, London North West Healthcare NHS Trust 08:40 – 09:40 Weight considerations for people with HIV Chair: Dr Laura Waters 08:40 – 09:10 ART & weight gain; myth or reality? Dr Anton Pozniak Chelsea & Westminster Hospital NHS Foundation Trust 09:10 – 09:25 Weight considerations for people with HIV - practical tips Maria Halley, Imperial College Healthcare NHS Trust Q&A 09:25 – 09:40 All speakers Clinical Conundrums – interactive cases 09:40 – 10:40 Chair: Dr Tristan Barber DOACs Rory Grier-Gavin, Imperial College Healthcare NHS Trust, London ART & the kidney (AKI, CKD, dialysis, pre-Tx) Clinical considerations: Professor Jeremy Levy, Imperial College London Pharmacological considerations: Justine Barnes, Birmingham Heartlands Hospital Q&A All Speakers 10:40 – 11:00 Break 11:00 – 12:00 Oral Research Presentations Session 1 Chairs: Dr Jonathan Underwood & Dr Sarah Cavilla 11:00 – 11:10 Sustained 97% HIV testing rate in the Emergency Department: the new gold standard Linda Cheyenne Vaccari 11:10 – 11:20 Safety and immunogenicity of V114, a 15-valent pneumococcal conjugate vaccine (PCV), in adults infected with human immunodeficiency virus (HIV): A phase 3 trial Laura Spowart 11:20 – 11:30 Mito-Flow: a novel assay for T-cell mitochondrial dysfunction in ageing and HIV Matthew Hunt 11:30 – 11:40 The prevalence and clustering of menopausal symptoms in women living with HIV Hajra Okhai 11:40 – 11:50 Long-term follow-up after a switch to Bictegravir, Emtricitabine, Tenofovir alafenamide (B/F/TAF) from a boosted protease inhibitor-based regimen F. -

Conference Report
CONFERENCE REPORT 11-12 December 2020 1 EXECUTIVE SUMMARY ........................................................................ 5 SCIENTIFIC PROGRAMME ..............................................................10 CONTENTS YING ORGANISING COMMITTEE AND FACULTY .......12 THE GLOBAL SPREAD OF ATTENDEES .................................14 EVALUATION REPORT .........................................................................16 THE EVALUATION METHODOLOGY.......................................17 KEY STATISTICS ........................................................................................17 RESULTS .........................................................................................................18 ACKNOWLEDGEMENTS .................................................................30 2 3 There are over 2.5 million people with HIV living in the European region1. Over the last three decades, tremendous advances have been made. While overall treatment opportunities have greatly evolved and those diagnosed early have the same life span as non-HIV infected people, PrEP and early test and treatment strategies are not equally available Europe-wide, resulting in a still impressive 140,000 new cases each year2. Of these, a significant number are diagnosed in a late stage. Meanwhile, key experts who have been there from the beginning of the epidemic start to retire and young doctors who have less access to expertise and reduced experience with complex patients are dealing with changing models of care and increasing mobile populations -

Scientific Programme Wednesday, 06 November 2019 Industry Sponsored
17th European AIDS Conference November 6-9, 2019 Basel, Switzerland Scientific Programme Wednesday, 06 November 2019 Industry sponsored session 08:00 - 12:00 Boston 1-3 Industry sponsored session (For more details, please visit the <a href="https://eacs-conference2019.com/index.php?article_id=166" target="_blank">conference website</a>) Page 1 / 174 17th European AIDS Conference November 6-9, 2019 Basel, Switzerland Scientific Programme Pre-conference workshop/course 09:30 - 16:00 Singapore EACS pre-educational course Convener: EACS Access to the webcasted session: <a href="http://resourcelibrary.eacs.cyim.com?mediaId=77962" target="_blank">Introduction</a> <a href="http://resourcelibrary.eacs.cyim.com?mediaId=77963" target="_blank">Zzzzzzz: Sleep issues beyond efavirenz: Clinical case</a> <a href="http://resourcelibrary.eacs.cyim.com?mediaId=77965" target="_blank">Zzzzzzz: Sleep issues beyond efavirenz: Overview</a> <a href="http://resourcelibrary.eacs.cyim.com?mediaId=77966" target="_blank">Zzzzzzz: Sleep issues beyond efavirenz: Questions</a> <a href="http://resourcelibrary.eacs.cyim.com?mediaId=77969" target="_blank">Non-AIDS respiratory issues: Clinical case</a> <a href="http://resourcelibrary.eacs.cyim.com?mediaId=77974" target="_blank">Non-AIDS respiratory issues: Overview</a> <a href="http://resourcelibrary.eacs.cyim.com?mediaId=77975" target="_blank">Non-AIDS respiratory issues: Questions</a> <a href="http://resourcelibrary.eacs.cyim.com?mediaId=77986" target="_blank">Dermatology in the modern era of HIV: Clinical case</a> <a -
UK Guideline for the Use of HIV Post-Exposure Prophylaxis 2021
UK Guideline for the use of HIV Post-Exposure Prophylaxis 2021 Guideline writing group Consultant Occupational Physician Kaveh Asanati Honorary Clinical Senior Lecturer, National Heart & Lung Institute, Imperial College London Consultant Physician Royal Free Hospital, London Sanjay Bhagani Senior Lecturer, Institute for Global Health, University College London Consultant Physician Chelsea and Westminster Hospital, London Marta Boffito Reader, Imperial College London Specialist Registrar, Brighton and Sussex University Hospital, Brighton Fiona Cresswell (Chair) Clinical PhD Fellow, London School of Hygiene and Tropical Medicine Valerie Delpech Consultant Epidemiologist, Public Health England Specialist Registrar, Hospital for Tropical Diseases, University College London Hospitals NHS Jayne Ellis Foundation Trust, London, UK Consultant HIV Medicine and Clinical Trials, Guy’s and St Thomas’ Hospital Julie Fox Honorary Reader Kings College London Linda Furness Sexual Health Adviser, Cardiff Royal Infirmary British HIV Association Guideline Committee Nadi Gupta Consultant HIV and Sexual Health, Rotherham NHS Foundation Trust British Association of Sexual Health and HIV Clinical Effectiveness Group Margaret Kingston Consultant Physician, Manchester Royal Infirmary. Honorary Chair Manchester University Consultant Occupational Physician Massoud Mansouri Deputy Course Director in Occupational Health, School of Medicine, Cardiff University Amanda Samarawickrama Consultant HIV and Sexual Health, Sexual Health South West London Kat Smithson National -

HIV Therapy:Layout 1 1/7/08 09:29 Page 11
HIV therapy:Layout 1 1/7/08 09:29 Page 11 Therapeutics HIV THERAPY past, present and future Since the identification of HIV in 1983 and licensing of zidovudine (AZT), the first antiretroviral agent, in 1986 we now have more than 20 agents available for HIV treatment from five drug classes. A patient starting therapy for the first time today can start on one pill once a day, a huge improvement to the complex regimens that characterised earlier stages in the history of HIV treatment. In addition, the past year has seen newly licensed drugs from both existing and new drug classes which have shifted the treatment paradigm for highly experienced individuals with high levels of drug resistance. However, the majority of HIV-infected subjects worldwide do not have access to the multitude of drugs we enjoy in the developed world; last year alone more than two million adults and children died of AIDS-related causes. This article will review recent advances in HIV treatment and discuss future challenges that the research community, pharmaceutical industry, healthcare providers and HIV- infected patients will need to address as time goes on. IV is a retrovirus meaning it is an RNA, increases. Drugs that block CXCR4 are in early By Dr Laura Waters rather than DNA, virus but has a unique stages of clinical development but maraviroc, a H enzyme (reverse transcriptase) enabling CCR5 blocker, was licensed at the end of last year the transcription, in host cells, of viral RNA into for treatment-experienced patients. This is the first DNA. HIV replication results in progressive ARV that acts on a host cell, rather than a viral, immune decline; the resultant abnormalities are target precipitating concerns regarding the long- manifold but most clearly manifested as a reduc- term safety. -

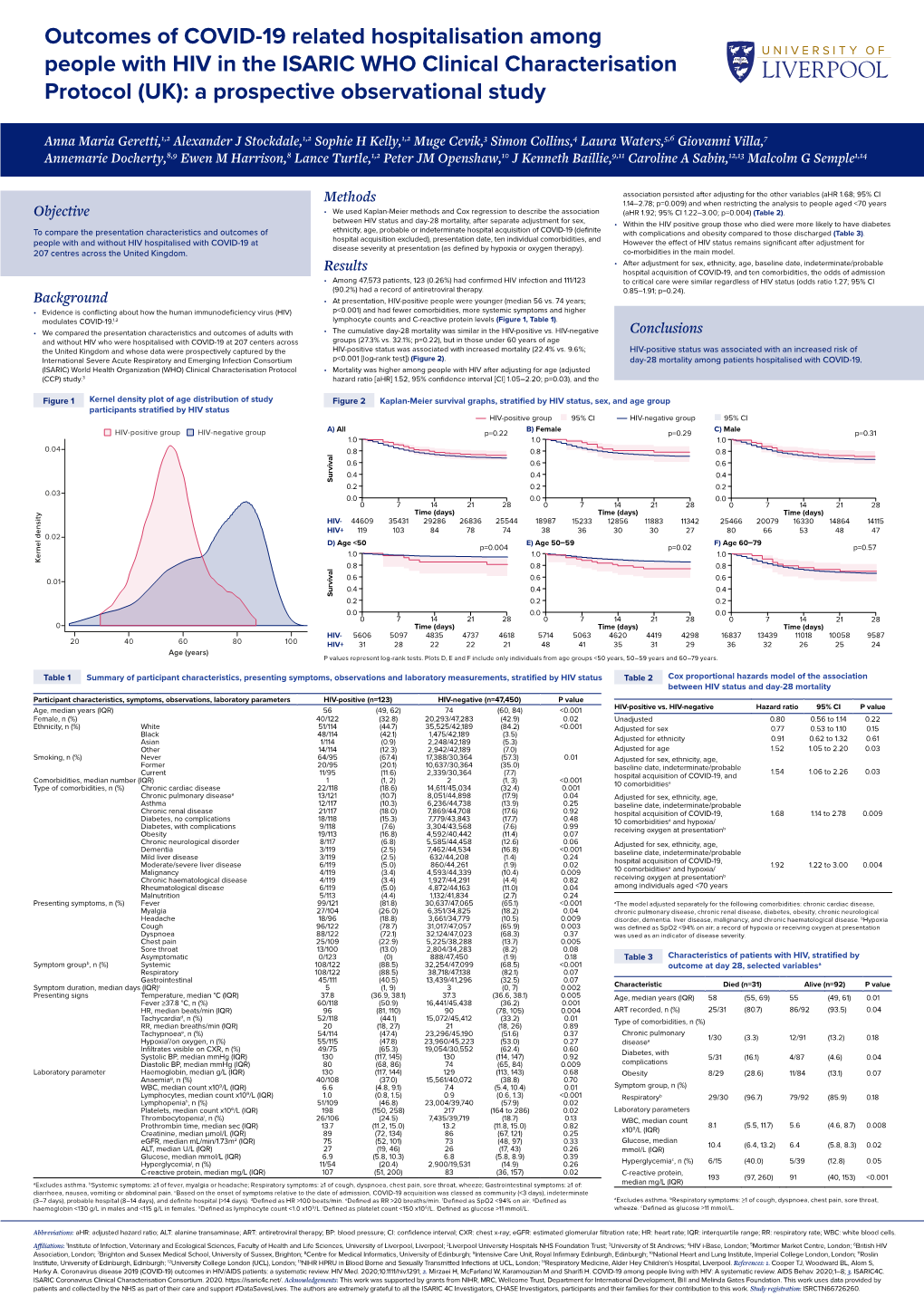
Pneumocystis Pneumonia, a COVID-19 Mimic, Reminds Us of the Importance of HIV Testing in COVID-19
ACUTE MEDICAL CARE Clinical Medicine 2020 Vol 20, No 6: 590–2 Pneumocystis pneumonia, a COVID-19 mimic, reminds us of the importance of HIV testing in COVID-19 Authors: Sophie Kelly,A Laura Waters,B Muge Cevik,C Simon Collins,D Joe Lewis,E Meng-San Wu,F Tom J BlanchardG and Anna M GerettiH While clinical environments are highly focused on COVID-19, days later, he presented again with significant hypoxia, worsening reports of missed or delayed treatment for conditions that bilateral upper lobe airspace shadowing on chest X-ray (Fig 1b), imitate COVID-19, such as pneumonia caused by the fungus anaemia (haemoglobin at 87 g/dL), lymphopenia (0.14 cells/mm3) Pneumocystis jirovecii, are emerging. Given the uncertain and raised C-reactive protein (212 mg/L); at this time oral thrush spectrum of COVID-19 presentations and variable sensitivity was noted. ABSTRACT of laboratory tests for SARS-CoV-2, there is a risk that, without a high index of suspicion, alternative aetiologies may be Diagnosis overlooked while pursuing a diagnosis of COVID-19. The British HIV Association has been calling for the inclusion of HIV On first presentation to the emergency department, perhaps testing in all patients admitted to hospital with suspected due to the relative frequency of COVID-19 during the peak of COVID-19. In this article we reflect on the importance of the pandemic and the consequent biases in clinical reasoning, including HIV testing to prevent avoidable morbidity and COVID-19 was considered the most likely diagnosis. On second mortality in our patients. -

BASHH PEPSE Guidelines
1 2 3 UK Guideline for the use of HIV Post-Exposure Prophylaxis 4 Following Sexual and Occupational Exposures 2020 5 6 Guideline writing group: Kaveh Asanati Consultant Occupational Physician Honorary Clinical Senior Lecturer, National Heart and Lung Institute, Imperial College London Sanjay Bhagani Consultant Physician Royal Free Hospital, London Senior Lecturer Marta Boffito Consultant Physician Chelsea and Westminster Hospital, London Reader, Imperial College London Fiona Cresswell Specialist Registrar, Brighton and Sussex University Hospital, Brighton (Chair) Clinical PhD Fellow, London School of Hygiene and Tropical Medicine Valerie Delpech Consultant Epidemiologist, Public Health England Jayne Ellis Specialist Registrar, Hospital for Tropical Diseases, University College London Hospitals NHS Foundation Trust, London, UK Julie Fox Consultant HIV Medicine and Clinical Trials, Guy’s and St Thomas’ Hospital Honorary Reader Kings College London Linda Furniss Sexual Health Adviser, Cardiff Nadi Gupta British HIV Association Guideline Committee Consultant HIV and Sexual Health, Rotherham NHS Foundation Trust Massoud Mansouri Consultant Occupational Physician Deputy Course Director in Occupational Health, School of Medicine, Cardiff University. Amanda Samarawickrama Consultant HIV and Sexual Health, Sexual Health South West London Kat Smithson National AIDS Trust Alex Sparrowhawk Terrence Higgins Trust Keith Radcliffe Chair BASHH Clinical Effectiveness Group, Consultant HIV and Sexual Health Whittall Street Clinic, Birmingham Paul Rafferty