Bacterial Vaginosis Balanitis (Change on the Helmet of the Penis)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Reference Sheet 1
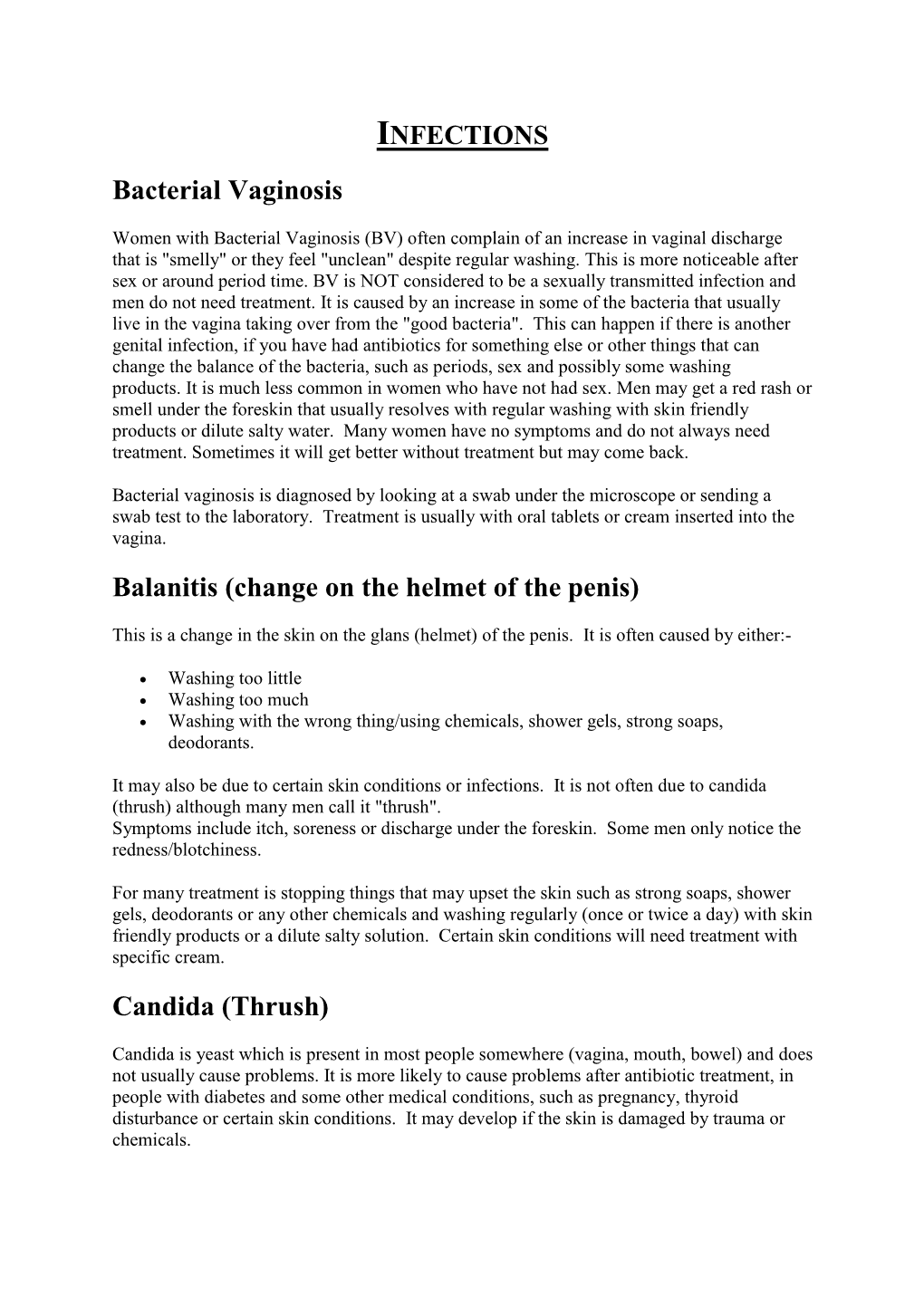
MALE SEXUAL SYSTEM 8 7 8 OJ 7 .£l"00\.....• ;:; ::>0\~ <Il '"~IQ)I"->. ~cru::>s ~ 6 5 bladder penis prostate gland 4 scrotum seminal vesicle testicle urethra vas deferens FEMALE SEXUAL SYSTEM 2 1 8 " \ 5 ... - ... j 4 labia \ ""\ bladderFallopian"k. "'"f"";".'''¥'&.tube\'WIT / I cervixt r r' \ \ clitorisurethrauterus 7 \ ~~ ;~f4f~ ~:iJ 3 ovaryvagina / ~ 2 / \ \\"- 9 6 adapted from F.L.A.S.H. Reproductive System Reference Sheet 3: GLOSSARY Anus – The opening in the buttocks from which bowel movements come when a person goes to the bathroom. It is part of the digestive system; it gets rid of body wastes. Buttocks – The medical word for a person’s “bottom” or “rear end.” Cervix – The opening of the uterus into the vagina. Circumcision – An operation to remove the foreskin from the penis. Cowper’s Glands – Glands on either side of the urethra that make a discharge which lines the urethra when a man gets an erection, making it less acid-like to protect the sperm. Clitoris – The part of the female genitals that’s full of nerves and becomes erect. It has a glans and a shaft like the penis, but only its glans is on the out side of the body, and it’s much smaller. Discharge – Liquid. Urine and semen are kinds of discharge, but the word is usually used to describe either the normal wetness of the vagina or the abnormal wetness that may come from an infection in the penis or vagina. Duct – Tube, the fallopian tubes may be called oviducts, because they are the path for an ovum. -

The Male Reproductive System
Management of Men’s Reproductive 3 Health Problems Men’s Reproductive Health Curriculum Management of Men’s Reproductive 3 Health Problems © 2003 EngenderHealth. All rights reserved. 440 Ninth Avenue New York, NY 10001 U.S.A. Telephone: 212-561-8000 Fax: 212-561-8067 e-mail: [email protected] www.engenderhealth.org This publication was made possible, in part, through support provided by the Office of Population, U.S. Agency for International Development (USAID), under the terms of cooperative agreement HRN-A-00-98-00042-00. The opinions expressed herein are those of the publisher and do not necessarily reflect the views of USAID. Cover design: Virginia Taddoni ISBN 1-885063-45-8 Printed in the United States of America. Printed on recycled paper. Library of Congress Cataloging-in-Publication Data Men’s reproductive health curriculum : management of men’s reproductive health problems. p. ; cm. Companion v. to: Introduction to men’s reproductive health services, and: Counseling and communicating with men. Includes bibliographical references. ISBN 1-885063-45-8 1. Andrology. 2. Human reproduction. 3. Generative organs, Male--Diseases--Treatment. I. EngenderHealth (Firm) II. Counseling and communicating with men. III. Title: Introduction to men’s reproductive health services. [DNLM: 1. Genital Diseases, Male. 2. Physical Examination--methods. 3. Reproductive Health Services. WJ 700 M5483 2003] QP253.M465 2003 616.6’5--dc22 2003063056 Contents Acknowledgments v Introduction vii 1 Disorders of the Male Reproductive System 1.1 The Male -

Introduction Remove the Udder Removing the Pizzle (Penis)
fig . removing the udder, cut outwards through the skin fig 2. removing the pizzle Introduction This guide describes the carcass dressing procedures either side of the pizzle joining the cuts around the that are ideally carried out in a deer larder, after back of the scrotum. Continue the single central cut the gralloch has been performed in the field. The through the skin almost to the anus, taking care not Gralloch guide should be considered essential to damage the haunches. Pull the pizzle free where it companion reading. Both are linked to the Carcass runs over the pelvis, cutting the blood vessels. Use Inspection, Carcass Transport, Basic Hygiene, and the knife to free the pizzle where it turns forward Larder guides. inside the “V” of the pelvis. Leave outside the carcass (draped down the back if the carcass is suspended). Remove the udder It will be removed with the aitch bone, bladder, Fig 1. This is best done in the larder but a large udder remainder of the rectum and anus, later. can prevent access to the rear end and may have to be removed in the field before opening the stomach. Split the aitch bone Pinch the skin just in front of the udder and pulling Figs 3. and 4. Note that some venison processors on it all the time, cut around the udder, removing it would prefer that the aitch bone remains intact, whole, with the skin. Do not take the cut any further check before cutting. While causing the least possible rearwards until back in the larder. -

Infertility Diagnosis and Treatment
UnitedHealthcare® Oxford Clinical Policy Infertility Diagnosis and Treatment Policy Number: INFERTILITY 008.12 T2 Effective Date: July 1, 2021 Instructions for Use Table of Contents Page Related Policies Coverage Rationale ....................................................................... 1 • Follicle Stimulating Hormone (FSH) Gonadotropins Documentation Requirements ...................................................... 2 • Human Menopausal Gonadotropins (hMG) Definitions ...................................................................................... 3 • Preimplantation Genetic Testing Prior Authorization Requirements ................................................ 3 Applicable Codes .......................................................................... 3 Related Optum Clinical Guideline Description of Services ................................................................. 3 • Fertility Solutions Medical Necessity Clinical Benefit Considerations .................................................................. 7 Guideline: Infertility Clinical Evidence ........................................................................... 8 U.S. Food and Drug Administration ........................................... 14 References ................................................................................... 15 Policy History/Revision Information ........................................... 18 Instructions for Use ..................................................................... 18 Coverage Rationale See Benefit Considerations -

Scalp Eczema Factsheet the Scalp Is an Area of the Body That Can Be Affected by Several Types of Eczema
12 Scalp eczema factsheet The scalp is an area of the body that can be affected by several types of eczema. The scalp may be dry, itchy and scaly in a chronic phase and inflamed (red), weepy and painful in an acute (eczema flare) phase. Aside from eczema, there are a number of reasons why the scalp can become dry and itchy (e.g. psoriasis, fungal infection, ringworm, head lice etc.), so it is wise to get a firm diagnosis if there is uncertainty. Types of eczema • Hair clips and headgear – especially those containing that affect the scalp rubber or nickel. Seborrhoeic eczema (dermatitis) is one of the most See the NES booklet on Contact Dermatitis for more common types of eczema seen on the scalp and hairline. details. It can affect babies (cradle cap), children and adults. The Irritant contact dermatitis is a type of eczema that skin appears red and scaly and there is often dandruff as occurs when the skin’s surface is irritated by a substance well, which can vary in severity. There may also be a rash that causes the skin to become dry, red and itchy. on other parts of the face, such as around the eyebrows, For example, shampoos, mousses, hair gels, hair spray, eyelids and sides of the nose. Seborrhoeic eczema can perm solution and fragrance can all cause irritant contact become infected. See the NES factsheets on Adult dermatitis. See the NES booklet on Contact Dermatitis for Seborrhoeic Dermatitis and Infantile Seborrhoeic more details. Dermatitis and Cradle Cap for more details. -

GERONTOLOGICAL NURSE PRACTITIONER Review and Resource M Anual
13 Male Reproductive System Disorders Vaunette Fay, PhD, RN, FNP-BC, GNP-BC GERIATRIC APPRoACH Normal Changes of Aging Male Reproductive System • Decreased testosterone level leads to increased estrogen-to-androgen ratio • Testicular atrophy • Decreased sperm motility; fertility reduced but extant • Increased incidence of gynecomastia Sexual function • Slowed arousal—increased time to achieve erection • Erection less firm, shorter lasting • Delayed ejaculation and decreased forcefulness at ejaculation • Longer interval to achieving subsequent erection Prostate • By fourth decade of life, stromal fibrous elements and glandular tissue hypertrophy, stimulated by dihydrotestosterone (DHT, the active androgen within the prostate); hyperplastic nodules enlarge in size, ultimately leading to urethral obstruction 398 GERONTOLOGICAL NURSE PRACTITIONER Review and Resource M anual Clinical Implications History • Many men are overly sensitive about complaints of the male genitourinary system; men are often not inclined to initiate discussion, seek help; important to take active role in screening with an approach that is open, trustworthy, and nonjudgmental • Sexual function remains important to many men, even at ages over 80 • Lack of an available partner, poor health, erectile dysfunction, medication adverse effects, and lack of desire are the main reasons men do not continue to have sex • Acute and chronic alcohol use can lead to impotence in men • Nocturia is reported in 66% of patients over 65 – Due to impaired ability to concentrate urine, reduced -

Assessment of Lower Urinary Tract Symptoms in Younger Men
MEN’S HEALTH ASSESSMENT OF LOWER URINARY TRACT SYMPTOMS IN YOUNGER MEN Lower urinary tract symptoms (LUTS) are common in the ageing male and represent a significant burden on both the patient and the healthcare system worldwide. 1,2 Accordingly, the majority of clinical trials and guidelines focus on the older patient, despite the fact that men below these ages will also present with many of the same symptoms. In this review, the authors explore the challenges of assessing and managing men below 50 years with LUTS. Dr Odunayo The aetiology of LUTS is multifactorial with causes How common are LUTS Kalejaiye attributed to dysfunction of the bladder and its in younger men? Urology SpR outlet – including the prostate, urethra and sphincter; The EPIC study, 3 a population-based survey which the neurological innervation of the lower urinary recruited men aged over 18 years, found that the Professor tract, and medical co-morbidities.1,2 It is important prevalence of LUTS increased with age, from 51.3% Raj Persad to consider all these aspects when assessing patients. in men aged 18-39 years to 62% in those aged 40-59 While in older men, benign prostatic enlargement years. This is compared with a prevalence of 80.7% Consultant is the commonest cause of male LUTS, in younger in men aged 60 years or older. Storage symptoms Urologist; men this is unusual, and other diagnoses should be were commonest in men 39 years or younger, with a Honorary considered more likely. prevalence of 37.5%, compared with a prevalence of Professor of 19.9% for voiding symptoms in this age group. -

Pelvic Inflammatory Disease (PID) Brown Health Services Patient Education Series
Pelvic Inflammatory Disease (PID) Brown Health Services Patient Education Series the uterine lining to treat abnormal What is PID? bleeding) PID (pelvic inflammatory disease) is ● PID risk from insertion of an IUD inflammation caused by infections ascending (intrauterine device) – occurs in the first 3 weeks post insertion from the vagina or cervix to the upper genital ● Abortion tract. This includes the lining of the uterus, the ovaries, the fallopian tubes, the uterine wall Why is it important to treat PID? and the uterine ligaments that hold these ● structures in place. PID is the most common serious infection of women aged 16 to 25 years What causes it? of age ● Untreated pelvic infections may cause Most cases of PID are caused by sexually adhesions in the fallopian tubes, which transmitted infections (STIs). The disease can be may lead to infertility caused by many different organisms or ● 1 in 4 women with acute PID develop combinations of organisms, but is frequently future problems such as ectopic caused by gonorrhea and chlamydia. Although pregnancy or chronic pelvic pain from Bacterial Vaginosis (BV) is associated with PID, adhesions whether the incidence of PID can be reduced by What are the symptoms? identifying and treating people with vaginas with BV is unclear. If you notice abnormal ● Painful intercourse could be the first discharge and a fishy vaginal odor (signs of BV) sign of infection ● you should be evaluated at Health Services. Pain and tenderness involving the lower abdomen, cervix, uterus and ovaries PID may also occur following procedures that ● Fever and chills create an open wound where infectious ● Nausea and/or diarrhea organisms can more easily enter, such as: ● Abnormal vaginal bleeding or discharge ● Biopsy from the lining of the uterus Early treatment can usually prevent these ● D & C (dilation and curettage – a problems. -

Vaginitis and Abnormal Vaginal Bleeding
UCSF Family Medicine Board Review 2013 Vaginitis and Abnormal • There are no relevant financial relationships with any commercial Vaginal Bleeding interests to disclose Michael Policar, MD, MPH Professor of Ob, Gyn, and Repro Sciences UCSF School of Medicine [email protected] Vulvovaginal Symptoms: CDC 2010: Trichomoniasis Differential Diagnosis Screening and Testing Category Condition • Screening indications – Infections Vaginal trichomoniasis (VT) HIV positive women: annually – Bacterial vaginosis (BV) Consider if “at risk”: new/multiple sex partners, history of STI, inconsistent condom use, sex work, IDU Vulvovaginal candidiasis (VVC) • Newer assays Skin Conditions Fungal vulvitis (candida, tinea) – Rapid antigen test: sensitivity, specificity vs. wet mount Contact dermatitis (irritant, allergic) – Aptima TMA T. vaginalis Analyte Specific Reagent (ASR) Vulvar dermatoses (LS, LP, LSC) • Other testing situations – Vulvar intraepithelial neoplasia (VIN) Suspect trich but NaCl slide neg culture or newer assays – Psychogenic Physiologic, psychogenic Pap with trich confirm if low risk • Consider retesting 3 months after treatment Trichomoniasis: Laboratory Tests CDC 2010: Vaginal Trichomoniasis Treatment Test Sensitivity Specificity Cost Comment Aptima TMA +4 (98%) +3 (98%) $$$ NAAT (like GC/Ct) • Recommended regimen Culture +3 (83%) +4 (100%) $$$ Not in most labs – Metronidazole 2 grams PO single dose Point of care – Tinidazole 2 grams PO single dose •Affirm VP III +3 +4 $$$ DNA probe • Alternative regimen (preferred for HIV infected -

The Human Foreskin the Foreskin Is Not an Optional Extra for a Man’S Body, Or an Accident
The Human Foreskin The foreskin is not an optional extra for a man’s body, or an accident. It is an integral, functioning, important component of a man’s penis. An eye does not function properly without an eyelid – and nor does a penis without its foreskin. Among other things, the foreskin provides: Protection The foreskin fully covers the glans (head) of the flaccid penis, thereby protecting it from damage and harsh rubbing against abrasive agents (underwear, etc.) and maintaining its sensitivity Sexual Sensitivity The foreskin provides direct sexual pleasure in its own right, as it contains the highest concentration of nerve endings on the penis Lubrication The foreskin, with its unique mucous membrane, permanently lubricates the glans, thus improving sensitivity and aiding smoother intercourse Skin-Gliding During Erection The foreskin facilitates the gliding movement of the skin of the penis up and down the penile shaft and over the glans during erection and sexual activity Varied Sexual Sensation The foreskin facilitates direct stimulation of the glans during sexual activity by its interactive contact with the sensitive glans Immunological Defense The foreskin helps clean and protect the glans via the secretion of anti-bacterial agents What circumcision takes away The foreskin is at the heart of male sexuality. Circumcision almost always results in a diminution of sexual sensitivity; largely because removing the foreskin cuts away the most nerve-rich part of the penis (up to 80% of the penis’s nerve endings reside in the foreskin) [1]. The following anatomy is amputated with circumcision: The Taylor “ridged band” (sometimes called the “frenar band”), the primary erogenous zone of the male body. -

A Clinical Case of Fournier's Gangrene: Imaging Ultrasound
J Ultrasound (2014) 17:303–306 DOI 10.1007/s40477-014-0106-5 CASE REPORT A clinical case of Fournier’s gangrene: imaging ultrasound Marco Di Serafino • Chiara Gullotto • Chiara Gregorini • Claudia Nocentini Received: 24 February 2014 / Accepted: 17 March 2014 / Published online: 1 July 2014 Ó Societa` Italiana di Ultrasonologia in Medicina e Biologia (SIUMB) 2014 Abstract Fournier’s gangrene is a rapidly progressing Introduction necrotizing fasciitis involving the perineal, perianal, or genital regions and constitutes a true surgical emergency Fournier’s gangrene is an acute, rapidly progressive, and with a potentially high mortality rate. Although the diagnosis potentially fatal, infective necrotizing fasciitis affecting the of Fournier’s gangrene is often made clinically, emergency external genitalia, perineal or perianal regions, which ultrasonography and computed tomography lead to an early commonly affects men, but can also occur in women and diagnosis with accurate assessment of disease extent. The children [1]. Although originally thought to be an idio- Authors report their experience in ultrasound diagnosis of pathic process, Fournier’s gangrene has been shown to one case of Fournier’s gangrene of testis illustrating the main have a predilection for patients with state diabetes mellitus sonographic signs and imaging diagnostic protocol. as well as long-term alcohol misuse. However, it can also affect patients with non-obvious immune compromise. Keywords Fournier’s gangrene Á Sonography Comorbid systemic disorders are being identified more and more in patients with Fournier’s gangrene. Diabetes mel- Riassunto La gangrena di Fournier e` una fascite necro- litus is reported to be present in 20–70 % of patients with tizzante a rapida progressione che coinvolge il perineo, le Fournier’s Gangrene [2] and chronic alcoholism in regioni perianale e genitali e costituisce una vera emer- 25–50 % patients [3]. -

The Ear, Nose, and Throat Exam Jeffrey Texiera, MD and Joshua Jabaut, MD CPT, MC, USA LT, MC, USN
The Ear, Nose, and Throat Exam Jeffrey Texiera, MD and Joshua Jabaut, MD CPT, MC, USA LT, MC, USN Midatlantic Regional Occupational and Environmental Medicine Conference Sept. 23, 2017 Disclosures ●We have no funding or financial interest in any product featured in this presentation. The items included are for demonstration purposes only. ●We have no conflicts of interest to disclose. Overview ● Overview of clinically oriented anatomy - presented in the format of the exam ● The approach ● The examination ● Variants of normal anatomy ● ENT emergencies ● Summary/highlights ● Questions Anatomy ● The head and neck exam consists of some of the most comprehensive and complicated anatomy in the human body. ● The ear, nose, and throat comprise a portion of that exam and a focused clinical encounter for an acute ENT complaint may require only this portion of the exam. Ears www.Medscape.com www.taqplayer.info Ear – Vestibular organ www.humanantomylibrary.com Nose/Sinus Anatomy Inferior Middle Turbinate Turbinate Septum Dorsum Sidewalls Ala Floor Tip www.ENT4Students.blogspot.com Columella Vestibule www.beautyepic.com Oral cavity and oropharynx (throat) www.apsubiology.org Neck www.rdhmag.com The Ear, Nose, and Throat exam Perform in a standardized systematic way that works for you Do it the same way every time, this mitigates risk of missing a portion of the exam Practice the exam to increase comfort with performance and familiarize self with variants of normal Describe what you are doing to the patient, describe what you see in your documentation Use your PPE as appropriate A question to keep in mind… ●T/F: The otoscope is the optimal tool for examining the tympanic membrane.