I Guide in Conducting an Implementation Review of the Community Health Service Record System
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Province, City, Municipality Total and Barangay Population AURORA
2010 Census of Population and Housing Aurora Total Population by Province, City, Municipality and Barangay: as of May 1, 2010 Province, City, Municipality Total and Barangay Population AURORA 201,233 BALER (Capital) 36,010 Barangay I (Pob.) 717 Barangay II (Pob.) 374 Barangay III (Pob.) 434 Barangay IV (Pob.) 389 Barangay V (Pob.) 1,662 Buhangin 5,057 Calabuanan 3,221 Obligacion 1,135 Pingit 4,989 Reserva 4,064 Sabang 4,829 Suclayin 5,923 Zabali 3,216 CASIGURAN 23,865 Barangay 1 (Pob.) 799 Barangay 2 (Pob.) 665 Barangay 3 (Pob.) 257 Barangay 4 (Pob.) 302 Barangay 5 (Pob.) 432 Barangay 6 (Pob.) 310 Barangay 7 (Pob.) 278 Barangay 8 (Pob.) 601 Calabgan 496 Calangcuasan 1,099 Calantas 1,799 Culat 630 Dibet 971 Esperanza 458 Lual 1,482 Marikit 609 Tabas 1,007 Tinib 765 National Statistics Office 1 2010 Census of Population and Housing Aurora Total Population by Province, City, Municipality and Barangay: as of May 1, 2010 Province, City, Municipality Total and Barangay Population Bianuan 3,440 Cozo 1,618 Dibacong 2,374 Ditinagyan 587 Esteves 1,786 San Ildefonso 1,100 DILASAG 15,683 Diagyan 2,537 Dicabasan 677 Dilaguidi 1,015 Dimaseset 1,408 Diniog 2,331 Lawang 379 Maligaya (Pob.) 1,801 Manggitahan 1,760 Masagana (Pob.) 1,822 Ura 712 Esperanza 1,241 DINALUNGAN 10,988 Abuleg 1,190 Zone I (Pob.) 1,866 Zone II (Pob.) 1,653 Nipoo (Bulo) 896 Dibaraybay 1,283 Ditawini 686 Mapalad 812 Paleg 971 Simbahan 1,631 DINGALAN 23,554 Aplaya 1,619 Butas Na Bato 813 Cabog (Matawe) 3,090 Caragsacan 2,729 National Statistics Office 2 2010 Census of Population and -

Spatial Variation in Groundwater Quality and Potential Extent of Contamination in Santa Ignacia, Tarlac, Philippines
Spatial variation in groundwater quality and potential extent of contamination in Santa Ignacia, Tarlac, Philippines Jessamine Gail M. Inson1,*, Christian E. Supsup1, and Mary Jane C. Flores1 1 Biology Department, De La Salle University, 2401 Taft Avenue, Manila, Philippines *Corresponding Author: [email protected] Abstract: The municipality of Santa Ignacia in the Province of Tarlac is highly dependent on groundwater; thus, its quality is significant to the community. This study presents the first assessment of groundwater quality and spatial variation of possible groundwater contamination in Santa Ignacia. A total of 274 groundwater samples were collected from 21 sampling sites in the municipality. Five groundwater quality parameters were measured, namely: pH, conductivity, nitrate, nitrite, and iron. Geographical coordinates of sampled wells and measurements of measured groundwater quality parameters were transformed and analyzed using Geographic Information System software, QGIS. Spatial variations of measured groundwater quality parameters were mapped using the Inverse Distance Weighted (IDW) interpolation technique. Constructed spatial variation maps revealed that groundwater quality parameters varied in the study area. All measured parameters, except nitrite content, were within the acceptable limits set by the DENR and WHO for groundwater quality. The nitrite content of groundwater in Padapada has exceeded the permissible limit which may cause long-term public health problems; hence, further evaluation and monitoring of groundwater quality in this area is highly recommended. The identification of the possible source of nitrite in Padapada is necessary to lessen the contamination risk; hence, protecting the groundwater sources in the municipality. Key Words: groundwater; groundwater quality; groundwater contamination; spatial variation; Geographic Information System 1. -

2015Suspension 2008Registere
LIST OF SEC REGISTERED CORPORATIONS FY 2008 WHICH FAILED TO SUBMIT FS AND GIS FOR PERIOD 2009 TO 2013 Date SEC Number Company Name Registered 1 CN200808877 "CASTLESPRING ELDERLY & SENIOR CITIZEN ASSOCIATION (CESCA)," INC. 06/11/2008 2 CS200719335 "GO" GENERICS SUPERDRUG INC. 01/30/2008 3 CS200802980 "JUST US" INDUSTRIAL & CONSTRUCTION SERVICES INC. 02/28/2008 4 CN200812088 "KABAGANG" NI DOC LOUIE CHUA INC. 08/05/2008 5 CN200803880 #1-PROBINSYANG MAUNLAD SANDIGAN NG BAYAN (#1-PRO-MASA NG 03/12/2008 6 CN200831927 (CEAG) CARCAR EMERGENCY ASSISTANCE GROUP RESCUE UNIT, INC. 12/10/2008 CN200830435 (D'EXTRA TOURS) DO EXCEL XENOS TEAM RIDERS ASSOCIATION AND TRACK 11/11/2008 7 OVER UNITED ROADS OR SEAS INC. 8 CN200804630 (MAZBDA) MARAGONDONZAPOTE BUS DRIVERS ASSN. INC. 03/28/2008 9 CN200813013 *CASTULE URBAN POOR ASSOCIATION INC. 08/28/2008 10 CS200830445 1 MORE ENTERTAINMENT INC. 11/12/2008 11 CN200811216 1 TULONG AT AGAPAY SA KABATAAN INC. 07/17/2008 12 CN200815933 1004 SHALOM METHODIST CHURCH, INC. 10/10/2008 13 CS200804199 1129 GOLDEN BRIDGE INTL INC. 03/19/2008 14 CS200809641 12-STAR REALTY DEVELOPMENT CORP. 06/24/2008 15 CS200828395 138 YE SEN FA INC. 07/07/2008 16 CN200801915 13TH CLUB OF ANTIPOLO INC. 02/11/2008 17 CS200818390 1415 GROUP, INC. 11/25/2008 18 CN200805092 15 LUCKY STARS OFW ASSOCIATION INC. 04/04/2008 19 CS200807505 153 METALS & MINING CORP. 05/19/2008 20 CS200828236 168 CREDIT CORPORATION 06/05/2008 21 CS200812630 168 MEGASAVE TRADING CORP. 08/14/2008 22 CS200819056 168 TAXI CORP. -

Pampanga River Basin: Flood of August 2004 (Southwest Monsoon As Enhanced by Typhoon Marce)
PRB Flood: SW Monsoon due to T.Marce – Aug2004 Pampanga River Basin: Flood of August 2004 (Southwest Monsoon as enhanced by Typhoon Marce) Summary Typhoon Marce (August 20-24, 2004) became the first destructive tropical cyclone to affect the Pampanga River Basin for the year 2004. Widespread rains for more than 3 days spawned by the intensified southwest monsoon as enhanced by Typhoon Marce inundated extensive areas of the western and central sections of Luzon, including Metro Manila. As a result, 64 persons died, more than 2.1 million people affected, and an estimated damage cost of P 2.3 Billion in both agriculture and infrastructure were incurred. An investigative survey team of the Pampanga River Flood Forecasting and Warning Center (PRFFWC) composed of Messrs. Armando P. Taruc (Senior Weather. Specialist), Hilton T. Hernando (Weather Facilities Specialist II) and Pablito Villablanca (Weather Observer III), was dispatched to the Pampanga River Basin to take on the following tasks: 1. Conduct a post-flood survey from September 7 to 12, 2004, to assess and make scientific evaluation of the flooding in the area; 2. Coordinate with other concerned agencies (LGU’s and NGO’s) and entities on the conduct of the study in connection with the flooding event; and 3. To recommend measures focusing on the non-structural means to minimize and mitigate flood losses in both life and property. This disastrous flood is considered the major flood of 2004. A record high of river stage for Pampanga River at Arayat station and, likewise, a record water level for the Candaba Swamp area were attained during this event. -
NDRRMC Update Sitrep No 10 Re Effects of TY QUIEL 8 Oct 2011 6 AM
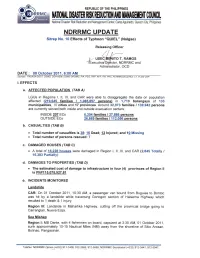
Region II: One (1) service motor banca and one (1) cargo/passenger vessel moored at San Vicente Fish Port, Sta. Ana, Cagayan bound for Maconacon and Divilacan, Isabela. Three (3) service motor banca and one (1) cargo/passenger motor banca moored at Veteranz Wharf Aparri, Cagayan bound to Camiguin Island, Calayan, Cagayan with 20 passenger stranded. Vehicular Accident Region I: Nick Basto, 6 years old from Brgy. San Julian Centra, Agoo, La Union suffered a cerebral concussion when he was hit by a tricycle while crossing the street from the evacuation center to buy food. He was brought to La Union Medical Center. Storm Surge Region I: Storm surge occurred in Barangays Tabuculan, Pasungol, and Bucalag of Santa, Ilocos Sur on 01 October 2011. Flooding Region III: Flashflood occurred in Brgys. Bamban and Daldayap, San Clemente, Tarlac due to the overflowing of the Batacan River; Brgy. San Isidro, Paniqui, Tarlac; Brgys. Pob. Sur Baybayaoas, Ptiombayug, Pedro L. Quines and Mamonit in Mayantoc, Tarlac (due to breached portion of Baybayaoas Dike); and Brgys .Pindangan 2 nd , Pao 1, 2, 3 and Surgi in Camiling, all in Tarlac. Fifty (50) passengers on board 3 buses were stranded along Romulo Highway in Camiling, Tarlac due to 5ft. flooding. They were rescued by joint efforts from PNP Camiling 3 rd Mechanized IB, 32nd Mechanized Company, Operatives of Camiling, Sta. Ignacia LGU, and PDRRMC. f) STATUS OF DAMS (as of 6:00 AM, 07 October 2011 ) The following dams opened their respective gates as the water levels have reached their spilling levels: Ambuklao (1 Gate / 0.5 m); Binga (2 Gates / 1.3 m); Magat (1 Gate / 2 m); and San Roque (1 Gate / 0.5 m). -

Balanga City, Bataan Orion, Bataan
CLES 1 Vercons Balanga City, Bataan 2 Owengen Orion, Bataan 3 Life Bank Foundation Inc. Balanga City, Bataan 4 Jay-del Construction Limay, Bataan 5 Bataan Commercial Enterprice Orani, Bataan 6 ABESCO Balanga City, Bataan 7 Gabby's Marketing Balanga City, Bataan 8 Crown Royale Balanga City, Bataan 9 Color Me Crazy Balanga City, Bataan 10 Ocampos Balanga City, Bataan 11 Sunset Cove Morong, Bataan 12 Seapine Mariveles, Bataan 13 Liberty Value Loan Pilar, Bataan 14 Studio 23 Hair and Body Salon Balanga City, Bataan 15 Lockheed Security Agency Limay, Bataan 16 Prime Power Agency Limay, Bataan 17 Plaza Hotel Balanga City, Bataan 18 J.E Manalo Limay, Bataan 19 Terp Asia Balanga City, Bataan 20 Hotel Brizo Morong, Bataan 21 Phi-Phi Hotel and Beach Resort Morong, Bataan 22 Balgon Hardware Mariveles, Bataan 23 Mariveles Bag Makers Mariveles, Bataan 24 Card MBA Inc. Balanga City, Bataan 25 Goldridge Construction Balanga City, Bataan 26 ICMC Balanga City, Bataan 27 DIDP Mariveles, Bataan 28 FS Phil corp. Limay, Bataan 29 Fundline Finance Corp. Balanga City, Bataan 30 Racal Motor Sales Balanga City, Bataan 31 Cindy's Balanga City, Bataan 32 Bluelight Security Agency Mariveles, Bataan 33 JPN Coiltech Mariveles, Bataan 34 Biggy and Bernie Mariveles, Bataan 35 Herma Shipyard Mariveles, Bataan CLES 36 Phil Am Mariveles, Bataan 37 Kisa Inc. Pilar, Bataan 38 Lingap Kapwa MPCA Balanga, Bataan 39 King's Garden Balanga, Bataan 40 Terp Asia Balanga, Bataan 41 Koree Plastic Corporation Mariveles, Bataan 42 Caro Incorporation Pilar, Bataan 43 Organic Fairment Abucay, Bataan 44 Samasaka Bagac, Bataan 45 UNTV Balanga, Bataan 46 Bataan White Corals Morong, Bataan 47 AMPC Abucay, Bataan 48 JBSS Quezon City 49 Security Bank Balanga, Bataan 50 Puregold Orani, Bataan 51 Puregold Balanga, Bataan 52 St. -

DIRECTORY of MINES & QUARRIES, Regional Office No
DIRECTORY OF MINES & QUARRIES, Regional Office No. III Duration of Permit Type of Location Region Mineral Province Municipality/City Commodity Permit Holder Operator Managing Official/Position Mailing Address Permit Number Effectivity of Expiration Permit (Barangay, Permit of Municipality, Stat Permit Area (hectares) Province) us Limay, Bagac & Mariveles, under III Metallic Bataan Limay, Bagac & Mariveles Gold/Silver/Copper Balanga Bataan Minerals Corp. Benguet Corporation Oscar T. Tranate, President 369 Adelfa St., San Jose, Balanga, Bataan MPSA 154-2000-III 3/31/2000 3/30/2025 1,410.24 exploratio Bataan n Aglao, San Marcelino, under III Metallic Zambales San Marcelino Gold/Silver/Copper Luis D. Dizon Lumiere Mining, Inc. Luis D. Dizon, Chairman of the Board 263 Ibuna Street, San Juan, MM MPSA 227-2006-III 1/17/2006 1/16/2031 160.00 exploratio Zambales n Guinabon, Santa Cruz, under III Metallic Zambales Santa Cruz Nickel Ramon G. Perlas Ramon G. Perlas Ramon G. Perlas, Permit Holder 17 Sison Street, Phase 6, BF Homes, Parañaque City MPSA 315-2010-III 2/10/2010 2/09/2035 286.25 exploratio Zambales n Zambales Diversified Metals 3/F DMCI Homes Corporate Center 1321 Apolinario Street, Lucapon, Santa Cruz, suspended III Metallic Zambales Santa Cruz Nickel DMCI Mining Corporation Cesar F. Simbulan, Jr., President MPSA 181-2004-III 5/22/2004 5/21/2029 3,765.39 operations Corporation Bangkal, Makati City Zambales under Guisguis, Santa Cruz, III Metallic Zambales Santa Cruz Nickel San Juanico Resources Corporation San Juanico Resources Corporation Cesario P. Magsaysay, President 29/F RCBC Tower I, Ayala Avenue, Makati City MPSA 265-2008-III 7/28/2008 7/27/2033 3,432.08 exploratio Zambales n 6/F MAPFRE Insular Corporate Centre, Ayala-Alabang Village, Guisguis, Santa Cruz, suspended III Metallic Zambales Santa Cruz Nickel Filipinas Mining Corporation LnL Archipelago Minerals, Inc. -

Summary Report
SUMMARY REPORT RESULT OF THE MGB GEOHAZARD ASSESSMENT COVERING THE EIGHTEEN (18) MUNICIPALITIES/CITY IN THE PROVINCE OF TARLAC In line with the Presidential Directive and NDCC resolutions following the February 17 Southern Leyte landslide incident, and the need to fast track the geohazard mapping program along the eastern seaboard of the Philippines, geologists from the Mines and Geosciences Bureau-Regional Office III (MGB-R3) conducted a geohazard assessment of the barangays in the municipalities/city n the province of Tarlac. Each barangay was classified according to their susceptibility to landslide and/or flooding. For landslide susceptibility, the rating parameters are as follows: High • Presence of active and/ or recent landslides • Presence of numerous and large tension cracks along slope adjacent to the community and that would directly affect the community • Areas with drainages that are prone to landslides damming • Steep/Unstable slopes consisting of loose materials Moderate • Areas with indicative and/or old landslides • Presence of small tension cracks along slope and are located away from the community • Moderate slopes 1 Low • Low to gently sloping • No presence of tension cracks Each barangay was rated into low, moderate or high for flooding susceptibility with the rating parameters as follows: Low • 0 – 0.5 meter depth of floodwaters Moderate • 0.51 – 1 meter depth of floodwaters High • > 1 meter depth of floodwaters With regards to landslide susceptibility, the barangays assessed include areas that are located on and/or near slopes and riverbanks and have the potential for landslide occurrence. The rating of each barangay presented herein particularly refers to the barangay proper since majority of the population is located there. -

(STEP) - FY 2017 List of Graduates As of October 30, 2017
Technical Education and Skills Development Authority Special Training for Employment Program (STEP) - FY 2017 List of Graduates As of October 30, 2017 Date Started Date Finished Region Province Name of TVIs Course/Qualification Title Delivery Mode Name Address (dd-mm-yy) (dd-mm-yy) POBLACION NORTH, SOLANO, NUEVA ELECTRICAL INSTALLATION AND Institution-Based ALCAYDE, LORENZO II ALDERSGATE COLLEGE LONE DISTRICT, NUEVA 8/8/17 10/6/17 VISCAYA MAINTENANCE NC II (Traditional) FERNANDEZ VISCAYA NUEVA ELECTRICAL INSTALLATION AND Institution-Based BACOTO, CYRON JOHN BAGAHABAG, SOLANO, LONE II ALDERSGATE COLLEGE 8/8/17 10/6/17 VISCAYA MAINTENANCE NC II (Traditional) TAMIDLES DISTRICT, NUEVA VISCAYA NUEVA ELECTRICAL INSTALLATION AND Institution-Based SAN JUAN, SOLANO, LONE II ALDERSGATE COLLEGE BALLON, RONALD ADRIANO 8/8/17 10/6/17 VISCAYA MAINTENANCE NC II (Traditional) DISTRICT, NUEVA VISCAYA NUEVA ELECTRICAL INSTALLATION AND Institution-Based BASCON, KLYDE HANZ STA. LUCIA, BAGABAG, LONE II ALDERSGATE COLLEGE 8/8/17 10/6/17 VISCAYA MAINTENANCE NC II (Traditional) GADIANO DISTRICT, NUEVA VISCAYA NUEVA ELECTRICAL INSTALLATION AND Institution-Based QUEZON, SOLANO, LONE II ALDERSGATE COLLEGE BUENAFE, DARYLL MUECA 8/8/17 10/6/17 VISCAYA MAINTENANCE NC II (Traditional) DISTRICT, NUEVA VISCAYA NUEVA ELECTRICAL INSTALLATION AND Institution-Based CALDERON , RANCES MASOC, BAYOMBONG, LONE II ALDERSGATE COLLEGE 8/8/17 10/6/17 VISCAYA MAINTENANCE NC II (Traditional) GIANCARLO LAD-AO DISTRICT, NUEVA VISCAYA NUEVA ELECTRICAL INSTALLATION AND Institution-Based -
NDRRMC Update SND Sitrep No 12 Re TY QUIEL 10 Oct 2011
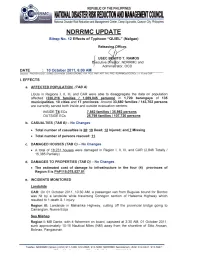
Region II: One (1) service motor banca and one (1) cargo/passenger vessel, both bound bound for Maconacon and Divilacan, Isabela, moored at San Vicente Fish Port, Sta. Ana, Cagayan Three (3) service motor bancas and one (1) cargo/passenger motor banca with a total of 20 passengers bound to Camiguin Island were left stranded as they moored at Veteranz Wharf Aparri, Cagayan Region III: Missing Fishermen on board F/Bs Princess Angela and Queen Lorena 2: • Four (4) out of eight (8) fishermen believed to be from F/b Princess Angela were rescued: one (1) was pronounced dead on arrival at the hospital, two (2) died while afloat in the middle of the sea while the remaining two (2) allegedly went out of their minds and untied themselves from the floating containers and have been missing since then; SAR operations are ongoing • Four (4) out of 9 fishermen from F/b Queen Lorena 2 were rescued on 05 October while SAR Operations is still ongoing for the missing The reported missing F/banca Brando Ice with 14 fishermen on board returned home safely on 05 October 2011. Said banca took shelter at the vicinity of Cabra Island, Mindoro during the height of the typhoon Vehicular Accident Region I: Nick Basto, 6 years old from Brgy. San Julian Central, Agoo, La Union suffered a cerebral concussion after being hit by a tricycle while crossing the street from the evacuation center to buy food. He was brought to La Union Medical Center for medical attention Storm Surge Region I: A storm surge occurred in Barangays Tabuculan, Pasungol, and Bucalag of Santa, Ilocos Sur on 01 October 2011. -

ORDINANCE No. 2011-008-Local Revenue Code
Page 1 of 72 pages, Local Revenue Code Republic of the Philippines MUNICIPALITY OF PANIQUI Province of Tarlac OFFICE OF THE SANGGUNIANG BAYAN EXCERPTS FROM THE MINUTES OF THE REGULAR SESSION OF THE SANGGUNIANG BAYAN OF PANIQUI, TARLAC HELD ON NOVEMBER 15, 2011 AT THE SB SESSION HALL. PRESENT: Hon. Genevieve S. Linsao – Vice Mayor-Presiding Officer Hon. Jayrold Z. Roxas, member Hon. Christian Alfred F. Cuchapin, member Hon. Evelyn S. David, member Hon. Rosauro V. Tayag, member – Majority Floor Leader Hon. Godofredo G. Tangonan, Jr., - Minority Floor Leader Hon. Dante P. Belarmino, member Hon. Gerardo N. Tiangsing, member Hon. William M. Ibay, Sr., member Hon. Gerardo R. Chanchico, ABC – Ex-Officio Member Hon. Jovien Ian U. Lagmay-SK – Ex-Officio Member ABSENT: None RESOLUTION NO. 130–2011 On motion of Councilor Dante P. Belarmino, unanimously seconded, RESOLVED, to approve and adopt, as it hereby approves and adopts, ordinance updating and supplementing the provisions of the LOCAL REVENUE CODE of the Municipality of Paniqui, Tarlac. RESOLVED FURTHER, that this resolution be enacted into an ordinance to wit; ORDINANCE NO. 2011-08 AN ORDINANCE UPDATING AND SUPPLEMENTING THE PROVISIONS OF THE LOCAL REVENUE CODE OF THE MUNICIPALITY OF PANIQUI, TARLAC. Be it ordained by the Sangguniang Bayan of Paniqui, Province of Tarlac, in session assembled, that: CHAPTER I. GENERAL PROVISIONS Article A. Short Title and Scope Section 1A.01 Short Title. This ordinance shall be known as the Local Revenue Code of 2011 of the Municipality of Paniqui, Tarlac. Section 1A.02 Scope and Application. This Code shall govern the levy, assessment and collection of taxes, fees, charges and other impositions within the territorial jurisdiction of the municipality. -
A APPLICATION with MOTION for PROVISIONAL AUTHORITY
Republic of the Philippines ENERGY REGULATORY COMMISSION Pacific Center Building San Miguel Avenue, Pasig City IN THE MATTER OF THE APPLICATION FOR APPROVAL OF ADDITIONAL CAPITAL ENERGY REGULATORY COMMiSSION EXPENDITURE PROJECTS FOR YEARS 20I7AND 2018, __ Time: WITH APPLICATION FOR R By: AUTHORITY TO SECURE LOAN FROM THE NATIONAL ELECTRIFICATION ADMINISTRATION AND PRAYER FOR PROVISIONAL AUTHORITY tO 17- 104 ERC CASE NOT RC TARLAC IELECTRIC COOPERATIVE, INC. (TARELCO I), :fl S iL r Applicant. U' x---------------------x w vi. a APPLICATION with MOTION FOR PROVISIONAL AUTHORITY Applicant, TARLAC IELECTRIC COOPERATIVE, INC. (TARELCO I for brevity), through counsel, unto this Honorable Commission, respectfully alleges, that: THE APPLICANT 1. TARELCO I is anon-stock, non-profit electric cooperative, duly organized and existing under and by virtue of the laws of the Republic of the Philippines, with principal offices at Amacalan, Gerona, Tarlac; liPage 2. It is engaged in the distribution electric light and power in the municipalities of Anao, Camiling, Gerona, Mayantoc, Paniqui, Pura, Moncada, Ramos, San Clemente, San Jose, San Manuel, Sta. Ignacia, and Victoria, in the Province of Tarlac; Barangays Batang Batang, Bora, Laoang, San Juan De Mata and Sto. Domingo of Tarlac City, Province of Tarlac; the municipalities of Cuyapo and Nampicuan, Province of Nueva Ecija; Barangays Maybubon, Agcano, Bagong Barrio, Bulakid, Caingin Tabing flog, San Agustin, Yuson, Lamorito and San Miguel of the municipality of Guimba, Province of Nueva Ecija, and Barangay Villa Rosa, municipality of Licab, Ii kewise in the Province of Nueva Ecija. LEGAL BASES FOR THE APPLICATION 3. Pursuant to Republic Act No. 9136, ERC Resolution 26, Series of 2009 and other laws and rules, and in line with its mandate to provide safe, quality, efficient and reliable electric service to its consumers, TARELCO I seeks approval, confirmation and authority from this HonorableCommission to implement its proposed additional Capital Expenditure (CAPEX) Projects for Years 2017 to 2018.