“Mosaic Pattern'' Foreign Bodies in Computed Tomography of the Head
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
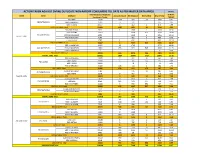
Action Taken Against Dvvnl Duplicate Non-Rapdrp Consumers Till Date As Per Master Data Apr20 in Nos
ACTION TAKEN AGAINST DVVNL DUPLICATE NON-RAPDRP CONSUMERS TILL DATE AS PER MASTER DATA APR20 IN NOS. Total Suspected Duplicate % W.R.T. ZONE Circle DivName Account Closed Bill Stopped Dismantled Grand Total Consumers Target TARGET EDD-BAH 17047 1116 289 28 1433 8.41 EDCFATEHABAD EDD-ETMADPUR 10405 75 232 307 2.95 EDD-III AGRA 23657 6 462 2 470 1.99 EDCFATEHABAD Total 51109 1197 983 30 2210 4.32 EDD-FIROZABAD 9032 1 1566 1 1568 17.36 EDD-JASRANA 14167 3408 826 4234 29.89 EDC-FIROZABAD EDD-SHIKOHABAD 6292 1449 6 1455 23.12 AGRA 1 ZONE EDD-SHIRSAGANJ 7149 482 3 485 6.78 S EDD-TUNDLA 4787 1 632 1 634 13.24 EDC-FIROZABAD Total 41427 2 7537 837 8376 20.22 EDD-II MAINPURI 16327 32 1745 1777 10.88 EDC-MAINPURI EDD-III MAINPURI 13681 433 629 546 1608 11.75 EUDD-1 MAINPURI 7 0 0.00 EDC-MAINPURI Total 30015 465 2374 546 3385 11.28 AGRA 1 ZONE Total 122551 1664 10894 1413 13971 11.40 EDD KHERAGARH 12877 7 322 32 361 2.80 EDD-I AGRA 27184 5 105 133 243 0.89 EDC-IAGRA EDD-II AGRA 24091 78 1 79 0.33 EDD-IV KIRAWALI 15183 146 114 4 264 1.74 EDC-IAGRA Total 79335 158 619 170 947 1.19 EDD-III MATHURA 7781 476 11 487 6.26 EDC-IIMATHURA EDD-MATH 5270 9 467 476 9.03 AGRA 2 ZONE EDC-IIMATHURA Total 13051 9 943 11 963 7.38 EDD GOVERDHAN 13014 7 613 2 622 4.78 EDCMATHURA EDD KOSI 8099 185 171 144 500 6.17 EDD-I MATHURA 10226 3 333 391 727 7.11 EDCMATHURA Total 31339 195 1117 537 1849 5.90 EUDD-II VRINDAVAN 1432 3 225 228 15.92 EUDCMATHURA EUDD-III MATHURA 453 2 4 6 1.32 EUDCMATHURA Total 1885 5 229 234 12.41 AGRA 2 ZONE Total 125610 367 2908 718 3993 3.18 EDD-I -

Drishti IAS Coaching in Delhi, Online IAS Test Series & Study Material
Drishti IAS Coaching in Delhi, Online IAS Test Series & Study Material drishtiias.com/printpdf/uttar-pradesh-gk-state-pcs-english Uttar Pradesh GK UTTAR PRADESH GK State Uttar Pradesh Capital Lucknow Formation 1 November, 1956 Area 2,40,928 sq. kms. District 75 Administrative Division 18 Population 19,98,12,341 1/20 State Symbol State State Emblem: Bird: A pall Sarus wavy, in Crane chief a (Grus bow–and– Antigone) arrow and in base two fishes 2/20 State State Animal: Tree: Barasingha Ashoka (Rucervus Duvaucelii) State State Flower: Sport: Palash Hockey Uttar Pradesh : General Introduction Reorganisation of State – 1 November, 1956 Name of State – North-West Province (From 1836) – North-West Agra and Oudh Province (From 1877) – United Provinces Agra and Oudh (From 1902) – United Provinces (From 1937) – Uttar Pradesh (From 24 January, 1950) State Capital – Agra (From 1836) – Prayagraj (From 1858) – Lucknow (partial) (From 1921) – Lucknow (completely) (From 1935) Partition of State – 9 November, 2000 [Uttaranchal (currently Uttarakhand) was formed by craving out 13 districts of Uttar Pradesh. Districts of Uttar Pradesh in the National Capital Region (NCR) – 8 (Meerut, Ghaziabad, Gautam Budh Nagar, Bulandshahr, Hapur, Baghpat, Muzaffarnagar, Shamli) Such Chief Ministers of Uttar Pradesh, who got the distinction of being the Prime Minister of India – Chaudhary Charan Singh and Vishwanath Pratap Singh Such Speaker of Uttar Pradesh Legislative Assembly, who also became Chief Minister – Shri Banarsidas and Shripati Mishra Speaker of the 17th Legislative -

ORIGINAL ARTICLE Pissn 0976 3325│Eissn 2229 6816 Open Access Article
ORIGINAL ARTICLE pISSN 0976 3325│eISSN 2229 6816 Open Access Article www.njcmindia.org ASSESSMENT OF MAGNITUDE AND THE CO-MORBIDITIES OF OVERWEIGHT AND OBESITY IN URBAN AND RURAL AREAS OF KANPUR Naresh Pal Singh1, Pankaj K Jain2, R P Sharma3, Suresh Chandra4, Seema Nigam4, Anamika Singh5 Financial Support: None declared Conflict of interest: None declared ABSTRACT Copy right: The Journal retains the copyrights of this article. However, reproduction of this article in the Background: Obesity is emerging as a global epidemic with part or total in any form is permis- growing threat to health in both developed and developing coun- sible with due acknowledgement of tries. It has become a major health concern for almost all the age the source. groups of the society. Objectives of the study is assess the preva- How to cite this article: lence and co-morbidities of overweight and obesity among per- Singh NP, Jain PK, Sharma RP, sons 15 years and above in urban and rural areas of Kanpur, UP. Chandra S, Nigam S, Singh A. As- Methods: For this cross-sectional study, multistage random sam- sessment of Magnitude and the Co- pling technique was used to select one colony in urban and one morbidities of Overweight and Obesity in Urban and Rural areas of village in rural area of Kanpur district. The desired sample size Kanpur. Natl J Community Med. was 2200. Detailed socio-demographic information was collected 2015; 6(1):1-5. on a pre-designed and pre-tested questionnaire. After anthropo- metric examination, Body Mass Index (BMI) was used to assess Author’s Affiliation: the overweight and obesity status. -

Head, Department of Neurosurgery
1 Full Bio-data in 106 Pages PROF. (DR.) RAJ KUMAR Head, Department of Neurosurgery Co-chairman, United Nation Affair (World Kabaddi Federation) Sanjay Gandhi Post Graduate Institute of Medical Sciences Raebareli Road, Lucknow Ex-In charge Apex Trauma Centre, SGPGIMS Ex-Vice Chancellor Uttar Pradesh University of Medical Sciences, Saifai, Etawah Ex-Director All India Institute of Medical Sciences Rishikesh, Uttarakhand, India 2021 2 DR. RAJ KUMAR B.Sc., M.B.B.S., M.S., M.Ch., Ph.D., M.R.C.S., F.R.C.S., F.A.M.S., F.N.S., M.A.M.S, M.N.A.Sc., F.A.S.E.T, D.Sc. Profile __________________________________________________________________________ Personal Details: OFFICIAL ADDRESS : HOD, Department of Neurosurgery Sanjay Gandhi Post Graduate Institute of Medical Sciences, Lucknow (UP)-226014, India Contact Numbers : 0522-249-4735,0522-249-4771 Email : [email protected] PERMANENT ADDRESS : A/82, Omaxe city, Saheed Path, Opposite Ramabai Chauki & Ambedkar University, Lucknow, Uttar Pradesh, India-226025 E-mail : [email protected], Website : www.profrajkumar.com PERSONAL INFORMATION Father’s Name : Late Sri Chhote Lal Date of Birth : 15th December, 1959 Place of Birth : Village- Paman, Kanpur (Dehat), UP, India Nationality : Indian Marital Status : Married 3 OBJECTIVES As Professor: 1. To achieve excellence in medical and super speciality of Neurosurgery. 2. To render quality medical training, medical research & quality patient care. 3. To enhance reputation of country by relevant research in medical field of Neurosciences. 4. To develop centers of excellence in medical field. 5. Social awareness in young doctors and bright minds for developing International standard of patient care and health care system. -

District Census Handbook, Etawah, Part XIII-B, Series-22, Uttar Pradesh
,CENSUS' 1981 ·;"Ttl XIII - ~ I ' . , ~/SERIES·22i 'lff,"~' MqVfifl .... S1~~ ~~ ~ UTTAR'· ·PRADESH, Pt1rt XIII· B . PRIMARY CENSUS J,SST,RACl Nr'll {GmT !!tan ~"~T ·DISTlUCT ~~~~l ETAWAH DISTRICT CENSUS . HANDBOOK ~~ ~ ~vf.r" ftr ~;~~~, Qtlft, 1. SR=QTq.fT i-il 2. ' srrlf!fi'{<i' v-vi 3. f~~ <fiT ~T;rf",o;r ix-x 4. ~~~<11uf ari'Cfi~ s. fGfCifT Gf'flTll'f<rT ~R=;Cfir <fir qf~:qlf xi-xiii 6. f~T smrf1{Cfi iif~Hm: ~~Flt iif;:r~~t1T 18-17 7• ar~w:qcr iifrfcr~ ~ f¥i SlNf1{Cf) \ifiM''''<i'r~T~ 18-2,; 8, ~f.qij ;;t'f-~ffftff ~ full" 'SfNf'f'li iif;WIl'fi'f'Tl(fT, 26-33 9. ~1{)Jr/.'I1TU7.f ~T'rl'1{Cfi \jj;:r~lIFfHn, (;:r~'3Tm ~ UllIT c:f'fT 'f11'if it i(ri ~ ~~) 3S-lSl 1. t!~T q~" (i) CT~"r(:f1{r;;f," (ii) llnrl <fiT qllfliiiif q:;ft 36-39 (Iii)' 'n~T1Jf ~r~fq<fi iifif'l'olTifrrn 44-73 (iv) • <T'l1;Tll srr~f;r~ iifif~UFtRf" (~trSfT ;:r~~q'ffi;cy;T)' 74-75 ( v) ~cTqT iI1T~cnf(1Cfir <fiT qf~f~ 77-82 (vi) <T~Utr ~Tt:rf1{Cfi iifil1T1Jfi(f'lr, (iifijef"..crtilR iI1T,\q'rf(:f'Pr) 84-85 (vii) iifq<l~CA'IJ'\ ;:r~Cfrf.;;fCfir 'fiT q-f~f~c 87-88 (viii) iI1Ti'rlt ~r~f'fCfi ;r.pJ'G'fifmT-: (~f~~ ;;1H ~"I') 98-91 (i:l) ~f~~ .;,,~ ~"I' 'fir q'f'\f~c 93 2. ~,1AJ CI'~~" (i) tT~«~ ;rA'Rr-t (n) llnrl <tr q~ifilf q:qT 96-99 (iii) llr;rT1Jf ~~fqCfi Gfif~I!T'lHr~ 194-129 (iv) if~Tlt ~l'{flfCfi ~iI1T1Jfi(Tm\ (~n:''f;rr "I~\q'rf~'fiT) 139-131· (v) 'll~~ if~ \.qTf~lflr 'fiT qf,~ 132-133 (vi) 'Wf'rtr ~T'ff~ ~JFtT'3r'\ (~T iI1T{ ~"I') (vii) ~~ iflJ'\ ~'Jt Cfir qf(f~c ii 3. -

List of Common Service Centres Established in Uttar Pradesh
LIST OF COMMON SERVICE CENTRES ESTABLISHED IN UTTAR PRADESH S.No. VLE Name Contact Number Village Block District SCA 1 Aram singh 9458468112 Fathehabad Fathehabad Agra Vayam Tech. 2 Shiv Shankar Sharma 9528570704 Pentikhera Fathehabad Agra Vayam Tech. 3 Rajesh Singh 9058541589 Bhikanpur (Sarangpur) Fatehabad Agra Vayam Tech. 4 Ravindra Kumar Sharma 9758227711 Jarari (Rasoolpur) Fatehabad Agra Vayam Tech. 5 Satendra 9759965038 Bijoli Bah Agra Vayam Tech. 6 Mahesh Kumar 9412414296 Bara Khurd Akrabad Aligarh Vayam Tech. 7 Mohit Kumar Sharma 9410692572 Pali Mukimpur Bijoli Aligarh Vayam Tech. 8 Rakesh Kumur 9917177296 Pilkhunu Bijoli Aligarh Vayam Tech. 9 Vijay Pal Singh 9410256553 Quarsi Lodha Aligarh Vayam Tech. 10 Prasann Kumar 9759979754 Jirauli Dhoomsingh Atruli Aligarh Vayam Tech. 11 Rajkumar 9758978036 Kaliyanpur Rani Atruli Aligarh Vayam Tech. 12 Ravisankar 8006529997 Nagar Atruli Aligarh Vayam Tech. 13 Ajitendra Vijay 9917273495 Mahamudpur Jamalpur Dhanipur Aligarh Vayam Tech. 14 Divya Sharma 7830346821 Bankner Khair Aligarh Vayam Tech. 15 Ajay Pal Singh 9012148987 Kandli Iglas Aligarh Vayam Tech. 16 Puneet Agrawal 8410104219 Chota Jawan Jawan Aligarh Vayam Tech. 17 Upendra Singh 9568154697 Nagla Lochan Bijoli Aligarh Vayam Tech. 18 VIKAS 9719632620 CHAK VEERUMPUR JEWAR G.B.Nagar Vayam Tech. 19 MUSARRAT ALI 9015072930 JARCHA DADRI G.B.Nagar Vayam Tech. 20 SATYA BHAN SINGH 9818498799 KHATANA DADRI G.B.Nagar Vayam Tech. 21 SATYVIR SINGH 8979997811 NAGLA NAINSUKH DADRI G.B.Nagar Vayam Tech. 22 VIKRAM SINGH 9015758386 AKILPUR JAGER DADRI G.B.Nagar Vayam Tech. 23 Pushpendra Kumar 9412845804 Mohmadpur Jadon Dankaur G.B.Nagar Vayam Tech. 24 Sandeep Tyagi 9810206799 Chhaprola Bisrakh G.B.Nagar Vayam Tech. -

Uttar Pradesh University of Medical Sciences, Saifai, Etawah
Uttar Pradesh University of Medical Sciences, Saifai, Etawah Faculty of Medicine/Dental (UG (MBBS) and PG (MD/MS/MDS) Academic Calendar (Terminal/University Examinations & Vacations) Year 2020 Sl Activity Tentative Dates Remarks PG (MD/MS/MDS) 1 Submission of Synopsis for JR-1 (admitted batch) Last date for submission 31.10.2020 2 Submission of Thesis for JR-3 (final year) 3 University Examination (MAIN) 13.04.2020 to 17.04.2020 Dates of practical exam will be finalized by HODs 4 University Examination (SUPP.) 05.10.2020 to 09.10.2020 Dates of practical exam will be finalized by HODs MBBS First Year (ANATOMY, PHYSIOLOGY, BIOCHEMISTRY) 1 1st Terminal for 1st Prof. ( 1st Semester) 27.01.2020 to 04.02.2020 - 2 2nd Terminal for 1st Prof (2nd Semester) 20.04.2020 to 28.04.2020 - 3 Pre University Exam for 1st Prof (2nd Semester) 05.08.2020 to 13.08.2020 - 4 FIRST RPOF EXAM 01.09.2020 to 08.09.2020 Dates of practical exam will be finalized by HODs 5 FIRST RPOF EXAM (SUPP.) 11.12.2020 to 18.12.2020 Dates of practical exam will be finalized by HODs MBBS Second Year (PATHOLOGY, MICROBIOLOGY, PHARMACOLOGY, FORENSIC MEDICINE) 1 1st Terminal for 2nd Prof (3rd and 4th semester) 19.08.2020 to 27.08.2020 Exam held in Morning Session 2 2nd Terminal for 2nd Prof (5th semester) 28.01.2020 to 06.02.2020 - 3 SECOND PROF EXAM 17.03.2020 to 26.03.2020 Dates of practical exam will be finalized by HODs 4 SECOND PROF EXAM (SUPP.) 11.09.2020 to 21.09.2020 Dates of practical exam will be finalized by HODs MBBS Third Year (COMMUNITY MEDICINE, E.N.T., OPHTHALMOLOGY) 1st Terminal for Final Prof. -

Automatic Weather Station Network of Uttar Pradesh
AUTOMATIC WEATHER STATION NETWORK OF UTTAR PRADESH S.No. District AWS Station Address 1. Agra Agra Dir I/C FMO, Hydrogen Factory, Agra 2. Aigarh Aligarh ADM, Finance, Aligarh. (Collectorate) 3. Etah Etah DM, Etah (Collectorate) 4. Etawah Etawah Baba Saheb Dr. B.R.A. College of Agriculture Engineering & Technology, Etawah. 5. Hathras Hathras DM, Hathras. (Collectorate) 6. Mainpuri Mainpuri Tehshildar Sadar, Mainpuri 7. Mathura Mathura DM, Mathura (Collectorate) 8. Allahabad Allahabad Dean, College of Forestry, Allahabad Agricultural Institute, Allahabad 9. Chitrakoot Karwi ADM (Relief) Sonepur,Karwi, Chitrakoot 10. Faizabad Faizabad DM, Firozabad ( Collectorate) 11. Fatehpur Fatehpur Officer In-Charge Nazarat, Fatehpur 12. Kaushambi Kokhraj Farm Suprientendent, Govt. Agri. Farm, Khokhraj, Kaushambi. 13. Meerut Meerut Chaudhry Charan Singh University campus, Meerut c/o M.O.Meerut 14. Bulandshahar Bulandshahar Marathwada Institute,Dhamerchola ,Bulandshahar 15. Lucknow Lucknow Director I/C, Met Centre, Lucknow 16. Aurraiya Aurraiya D.M. Aurraiya (Collectorate) 17. Bharaich Bahraich Officer In-charge, Crop Research Station, N.D. University of Agri & Tech, Baharaich. 18. Gonda Gonda ADM, Gonda 19. Kannauj Kannauj D.M. kannauj. (Collectorate) 20. Kanpur City Kanpur Dept. of Agronomy, Chandra Shekhar Azad University of Agriculture, Kanpur 21. Kanpur Dehat Akabarpur DM Kanpur Dehat, (Akabarpur) 22. Raebareili Fursatganj Senior ATC Officer , IGRUA, Fursatganj, Raebareli C/o M.O.Fursatganj 23. Sultanpur Sultanpur Krishi Vigyan Kendra, C/o Met. Office K.N.I.T.,Sultanpur C/O M.O.Sultanpur 24. Unnao Unnao Dy. Dir Agri. Unnao 25. Bareilly Bareilly DM, Barailly (Collectorate) 26. Badaun Badaun DM, Badaun (Collectorate) 27. Lakhimpur Kheri Palliakalan BDO, Vikash Khand Bhawan, Paliakalan, Lakhimpurkheri. -

23 2 2019 11 55 9 Noida 2
from Downloaded www.upsrtc.com From Downloaded www.upsrtc.com GENERAL Father's Obtain Total Date of A EX- ARDH- MRATAK RETIR O SR NO. Name Address Marks% RefNo. Caste NCC ITI Name Marks Marks Birth LEVEL ARMY SAINIK ASHRIT E LEVEL ARVIND RAMCHAN DEEN NAGARIYA TIMANPUR MAINPRUI NOIDA- 802 KUMAR DRA SINGH SHARIFPUR UP 205265 368 500 73.6 26.Mai.97 9534 General YES MATA VILL BIRNAI POST BAIRIBISA THANA VISWAS PRASAD GOPIGANJ DIST S R N BHADOHI PIN NOIDA- 803 UPADHYAY UPADHYAY 221303 368 500 73.6 20.Jun.97 9416 General YES ANKIT SUSHEEL VILLAGE NAGLA CHHATTU POST URESAR NOIDA- 804 KUMAR KUMAR THANA EKA DIST FIROZABAD UP 368 500 73.6 10.Jul.97 4582 General YES RAVINDRA PRATAP JASWANT VILL AND POST AKOHARI THANA NOIDA- 805 SINGH SINGH PARASPUR DISTT GONDA UP PIN 271504 368 500 73.6 20.Jul.97 10142 General YES Girraj Kamalesh Vill- Saray Raj Nagar Post- Jalesar Distt- NOIDA- 806 Kishor Chandra Etah 368 500 73.6 04.Aug.97 9844 General YES RAKESH VILLAGE AND POST SHAHPUR BANGAWA From PRANJAL KUMAR TEHSIL ALAPUR THANA ALAPUR DISTRICT NOIDA- 807 SINGH SINGH AMBEDKAR NAGAR PIN 224181 368 500 73.6 02.Dez.97 5952 General YES ROHAN YOGENDRA VILLAGE MAJURI KHAS POST NEWADA PS NOIDA- 808 SINGH SINGH GAGAHA GORAKHPUR 368 500 73.6 05.Jul.98 2405 General YES PINTOO V.PO DHIKANA BARAUT , BAGHPAT UTTAR NOIDA- 809 KUMAR RAMPAL PRADESH 250611 368 500 73.6 10.Jul.98 12573 General YES SANDEEP GULVIR VPO THORA TEH JEWAR DISTT G B NAGAR NOIDA- 810 SHARMA SHARMA 203155 368 500 73.6 25.Nov.98 11743 General YES LANKESH RAMPURA SIHUA MAMAN HIMATPUR NOIDA- 811 HIMANSHU -

Ground Water Year Book Uttar Pradesh (2014 - 2015)
GROUND WATER YEAR BOOK UTTAR PRADESH (2014 - 2015) Foreword Groundwater on account of its universal availability, dependability and low capital cost, is the major source of water to meet the requirement of various sector in India. However, with a rapid growth of population and all round development, there is incessant pressure on the ground water withdrawal resulting compulsive awakening in terms of both the quality and quantity. Ground water has an important role in meeting the water requirements of agriculture, industrial and domestic sectors in the state. About 78% percent of irrigation requirements in the Uttar Pradesh state are being met from ground water resources. If the present trend of the increasing demand remains incontrollable, the resource may be as strategic as are the minerals resources. Though in contrast to this, the resource of groundwater as a part of hydrologic cycle is replenishable. The indiscriminate exploitation of groundwater has led to depletion of storage is essential in order to avoid the adverse impact. This could be achieved only after careful monitoring of various inpiuts of hydrological system. Temporal variation in the Ground water system need to be studied for the scientific management of the resource. In view of this Central Ground Water Board, Northern Region, Lucknow has setup a network of 1241 Ground Water Monitoring Wells all over the state to maintain a regular database. The behavior of water level is monitored four times every year in May, August, November and January. To ascertain the hydrochemical behavior of ground water, samples are collected from representative wells once a year during the month of May and samples are analysed in the chemical laboratory of the office. -

Reported Districtwise L1/L1 Covid Care Center, L2, L3 Isolation Beds with Hospital Name No
Reported Districtwise L1/L1 Covid Care Center, L2, L3 Isolation Beds with Hospital Name No. of No. of No. of S.N. District L1 Hospital Name L1 Covid Care Centre Beds L2 Hospital Name L3 Hospital Name Beds Beds Beds Hindustan Engg Collage 450 RASA PUBLIC SCHOOL 75 Agra Public School 225 Neminath Homeopathic Medical 100 SNMC Medical 1 Agra CHC Baroli Ahir 30 College Chauhan hospital 20 375 College Mount Litera School, Shamshabad Road 100 Global Agra Convent School, Shamshabad Road 250 K.D. Medical College 620 2 Mathura CHC Vrindavan 30 IVS SANSKRITI UNVERSITY 160 Krishna Mohan Medical College & 520 Hospital F. H. Medical Collage Pandit Deen Dayal Upadhyay CHC Jasrana 30 100 620 3 Firozabad Govt. Ashram Padwati Vidyalaya CHC Deedamai 60 J.S. Hospital Shikohabad 100 ASMC 180 4 Mainpuri CHC Bhogon 30 Jawahar Navodayay Vidyalaya 250 DDU Joint Hospital 100 Bed Combined Hospital 100 100 5 Aligarh CHC Harduaganj 30 Jeevan Jyoti Hospital 100 Sai Ayurvedic Hospital 125 J. N Medical Collage 66 ZH PG College Agra Road 250 Dr. Shailendra Jain Hospital 6 Etah CHC Baghwala, 30 25 Jawahar Navodayay Vidyalaya 100 Sri ram Hospital Lord Krishna Public School, 100 7 Hathras 30 Mursan, Hathras 150 CHC Mursan J P Degree Collage 150 ITI Yakutganj, Sahawar 80 8 Kasganj DCH soron 30 V K Jain Collage of Management 80 Seth Jaipuriya School Mirla, 250 9 Azamgarh 30 GMC 420 100 Bed Combined Hospital 100 CHC-Kolhukhor Town Politechnic Collage 125 Gaurav Multispeciallity Hospital 10 Ballia CHC Basantpur 30 50 Sacred Heart School, Ballia 125 Bapu Ayurvedic Medical College 100 11 Mau 30 CHC PARDAHA No. -

PDF of Trial CTRI Website URL
PDF of Trial CTRI Website URL - http://ctri.nic.in Clinical Trial Details (PDF Generation Date :- Fri, 24 Sep 2021 18:47:14 GMT) CTRI Number CTRI/2020/06/025998 [Registered on: 20/06/2020] - Trial Registered Prospectively Last Modified On 18/06/2020 Post Graduate Thesis No Type of Trial Interventional Type of Study Drug Ayurveda Study Design Randomized, Parallel Group, Placebo Controlled Trial Public Title of Study Efficacy of An Ayurvedic Preparation Raj Nirwan Bati (RNB) on symptomatic COVID-19 Patients Scientific Title of To Determine the Efficacy of An Ayurvedic Preparation Raj Nirwan Bati (RNB) on symptomatic Study COVID-19 Patients: A Double-Blind Randomized Controlled Trial Secondary IDs if Any Secondary ID Identifier NIL NIL Details of Principal Details of Principal Investigator Investigator or overall Name Dr Raj Kumar Trial Coordinator (multi-center study) Designation Vice Chancellor Affiliation Uttar Pradesh University of Medical Sciences Address Uttar Pradesh University of Medical Sciences, Saifai, Etawah Etawah UTTAR PRADESH 206130 India Phone 9450610933 Fax 05688276509 Email [email protected] Details Contact Details Contact Person (Scientific Query) Person (Scientific Name Dr Naresh Pal Singh Query) Designation Professor (Junior Grade) Affiliation Uttar Pradesh University of Medical Sciences Address Department of Community Medicine, Uttar Pradesh University of Medical Sciences, Saifai, Etawah Etawah UTTAR PRADESH 206130 India Phone 09458641119 Fax 05688276509 Email [email protected] Details Contact Details Contact