The Use and Effectiveness of Powered Air Purifying Respirators in Health Care: Workshop Summary
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Proposed Industrial Powered, Air-Purifying Respirator (PAPR) Standard Draft: November 4, 2005
D R A F T F O R D I S C U S S I O N Concept: Proposed Industrial Powered, Air-Purifying Respirator (PAPR) Standard Draft: November 4, 2005 84.300 Scope 84.301 Definitions 84.302 Description 84.303 Required components 84.304 General construction 84.305 Breathing tubes 84.306 Body harnesses 84.307 Head harness 84.308 Respiratory inlet coverings 84.309 Eyepieces of respiratory inlet coverings 84.310 Inhalation and exhalation valves 84.311 Exhalation valve leakage 84.312 Breathing resistance 84.313 Air pressure determination for maintaining positive pressure 84.314 Air flow determination for testing cartridges, canisters, and/or filters at a constant flow and for machine breathing gas testing 84.315 PAPR100 and PAPR95 particulate filter efficiency level determination 84.316 Chemical cartridge/canister gas/vapor removing effectiveness 84.317 Laboratory Respiratory Protection Level (LRPL) 84.318 Field of view 84.319 Low temperature fogging 84.320 Noise levels 84.321 Breathing gas: Carbon dioxide (CO2) machine test 84.322 Breathing gas: Oxygen (O2) and Carbon dioxide (CO2) human subject-generated 84.323 Low pressure indicator 84.324 Full and low battery power indicator 84.325 Battery life 84.326 End-of-Service-Life (ESLI) criteria 84.327 Service time limitations 84.328 Shelf life limitations 84.329 Intrinsic safety, optional 84.330 Hydration device (drink tube), optional 84.331 Additional container requirements specific to PAPRs 84.332 Additional labeling requirements specific to PAPRs D R A F T F O R D I S C U S S I O N 1 D R A F T F O R D I S C U S S I O N 84.300 Scope: Powered, air-purifying Respirators (PAPRs) shall be approved under this subpart The purpose of Subpart P is to establish procedures and minimum requirements for issuing approvals and extensions of approval specifically to PAPRs. -

Powered Air Purifying Respirator (PAPR) Standard Subpart P
Proposed Concept: Powered Air-Purifying Respirator (PAPR) Standard Subpart P December 21, 2007 1. Scope 2. Definitions 3. Descriptions 4. Base Requirements – All PAPR shall meet the following base requirements: 4.1 Non-respiratory 4.1.1 Required components 4.1.2 General construction 4.1.3 Breathing tubes 4.1.4 Body harnesses 4.1.5 Head harness 4.1.6 Respiratory inlet coverings 4.1.7 Eyepieces/lens of respiratory inlet coverings 4.1.8 Noise levels 4.1.9 Low pressure indicator 4.1.10 Power 4.1.11 Battery life 4.1.12 End of Service Life (ESLI) criteria 4.1.13 Shelf life limitations 4.1.14 Failure Mode and Effects Analysis (FMEA) 4.2 Respiratory 4.2.1 Inhalation and exhalation valves 4.2.2 Exhalation valve leakage 4.2.3 Breathing resistance 4.2.4 Air flow determination 4.2.5 Breathing gas: Carbon dioxide (CO2) machine tests 4.2.6 Service time limitations 4.2.7 Chemical cartridge/canister gas/vapor removal effectiveness 4.2.8 PAPR P95 and PAPR P100 particulate filter efficiency level determination 4.2.9 Breathing gas concentrations determination: Oxygen (O2) and Carbon dioxide (CO2) human subject generated 4.2.10 Laboratory Respirator Protection Level (LRPL) Draft For Discussion Only 5. Enhanced Chemical, Biological, Radiological, Nuclear (CBRN) Requirements - Performance requirements beyond base requirements that may be desired by applicant for approval 5.1 CBRN requirements 5.2 Lower Level Chemical, Biological, Radiological, Nuclear (LCBRN) requirements 6. Additional Enhanced Requirements 6.1 Flammability and Heat Resistance 6.2 Silent Operation 6.3 Operational Temperature Range 6.4 Hydration device (drink tube) 6.5 Intrinsic Safety 2 Draft For Discussion Only 1. -

Chin-Type Gas Masks Full-Facepiece Air-Purifying Respirator
Chin-Type Gas Masks Full-Facepiece Air-Purifying Respirator The MSA Chin-Type Gas Mask is a full-facepiece air-purifying respirator with a single canister, designed for respiratory protection against specific gases or a group of gases as indicated by canister identification. Because every life has a purpose... Chin-Type Gas Masks The lightweight, round plastic canister attaches directly to the facepiece, yet permits downward head movement. Chin-Type Gas Masks can be used for many applications including paper mills, chemical plants, agri-business, fumigation and HazMat situations. Choices include a silicone or rubber facepiece in three sizes and four styles, optional carrying/storage case and wall hanger. A belt-mounted option is also available. MSA NIOSH-approved canisters with particulate filters have a five-year shelf life. Round plastic chin canisters are ovidedpr for one of four hazard groups: • Phosphine/ammonia/chlorine/P100 • Organic vapor/P100 • Hydrogen fluoride/chlorine/P100 • Formaldehyde/acid gas/chlorine dioxide/hydrogen sulfide/P100 Gas masks are designed solely to remove specific contaminants from air. Their use is restricted to entry into, or work within, tmospheresa that are within canister limitations. They are not intended for oxygen-deficient atmospheres (less than 19.5% 2O ). Gas masks may be used for escape only from atmospheres in which the contaminant concentration does not exceed the gas mask maximum use concentration. Chin-Type Gas Masks have the following maximum use limitations: Routine use: 50 times the Permissible Exposure Level (PEL) - Do not exceed the Immediately Dangerous to Life or Health (IDLH) concentration. Escape use: contaminant concentrations up to gas mask maximum use concentrations, providing there is sufficient oxygen to support life. -

War Gases .Pdf
yh&% .*i From the collection of the m Prejinger h v Jjibrary San Francisco, California 2007 THE WAR GASES WAR GASES Their Identification and Decontamination BY MORRIS B. JACOBS, Ph.D. Food, Drug and Insecticide Admin. U. S. Dept. of Agr. 1927 Chemist Department of Health, City of New York, 1928. Formerly, Lt. U. S. Chemical Warfare Service Reserve INTERSCIENCE PUBLISHERS, INC. NEW YORK, N. Y.-1942 Copyright, 1942, by INTERSCIENCE PUBLISHERS, INC. 215 Fourth Avenue, New York, N. Y. Printed in U. S. A. by WAVERLY PRESS, BALTIMORE, MD. PREFACE Relatively little has been written in the United States of America on the subject of passive defense, or as we would put it, civilian defense against poison gas. One of the very first steps in defense of this nature is a system for the detection, the sampling and the identification of the chemical war- fare agents, and the decontamination of areas and materials polluted by them. It is the aim of this book to present these subjects so that the informa- tion given will be useful to the gas identification officer, the war gas chemist, the decontamination officer, and the health officer. While this book was written primarily for the aforementioned officers, Chapters I, II, III, part of IV and VII should prove of value to the air raid warden and, in general, to all persons dealing with the above mentioned phases of gas defense. It is written so that it can be used for the training of gas identifi- cation officers, as a manual by chemists and decontamination officers, and as a source of information on the analytical chemistry of the war gases. -

Standard for Gas Mask
JICOSH Home | Standard for Gas Mask http://www.jniosh.go.jp/icpro/jicosh-old/english/law/GasMask/index.html Standard for Gas Mask (Ministry of Labour Notification No. 68 of September 26, 1990) Latest Amendments: Ministry of Health, Labour and Welfare Notification No.299 of September 18, 2001 Japanese The Standard for Gas Mask has been enacted as follows conforming to and in order to enforce the Industrial Safety and Health Law (Law No. 57 of 1972). Contents Article 1 Scope of application Article 2 Type of gas mask Article 3 Materials Article 4 Test on strength Article 5,6 Structure Article 7 Performance tests Article 8 Labeling and others Article 9 Exceptions of this Standard Supplementary Provisions (Scope of application) Article 1 The standard issued in the Ministry of Health, Labour and Welfare Notification is applied to the gas masks which are categorized into those described in the left column of the following Table, according to the kinds of hazardous materials (including particulates which coexist with these gaseous materials) described in the right column of the same Table, among the gas masks to be used at the places where gases, vapors and particulates mixed with these gases or vapors may harm the human body by inspiring them. However, this standard is not applied to those gas masks used in places where oxygen concentration is below 18% or the concentrations of gases or vapors exceeds 2% ( in case the gas is ammonia, the concentration exceeds 3%). Category Hazardous materials Gas masks for halogens Halogen gases or vapors Gas masks for organic compounds Organic compound vapors Gas masks for carbon monoxide Carbon monoxide Gas masks for ammonia Ammonia Gas masks for sulfur dioxide Sulfur dioxide (Type of gas mask) Article 2 Gas masks shall be categorized into the types described in the left column of the following Table, according to the form and the scope of application described in the right column of the same Table. -

Gas Masks for Law Enforcement 5555-166
Gas Masks for Law Enforcement [ Respiratory Protection for Homeland Security ] G A S M A S K S F O R MSA’s Gas Masks: from Military Warfare to Civil Unrest to CBRN Threats MSA has been making Gas about wearing an exceptionally As one SWAT officer recently Masks since World War I. designed gas mask. “An enemy stated,“Equipment needs to be can drop blood or blister agents light, dependable, and foolproof. [ Military Warfare ] on an airfield, so you never The MSA [Advantage® 1000] Over 7 million MSA Gas Masks, know WHEN you’re going to mask is.” including the M17, M23, and need that protection. The design Another agreed,“If you need to M40 Series, have protected US and shape of the lens and this use force in hostage situations, military forces throughout the mask are very important in you have to see exactly what past century. MSA designed and enabling you to aim and fire you are doing while wearing developed the MCU-2/P gas your weapon. You’re not worry- your mask. The range of visibili- mask for the US military (USAF ing about comfort; you want to ty and optics are great.” in Desert Storm). Our be sure you can SEE.” Millennium™ Gas Mask is a [ CBRN Threats ] [ Civil Unrest ] clone of this USAF-Navy mask All threats to US homeland that’s now available to Law However, law enforcement offi- security—home-grown or Enforcement users. cers, especially SWAT teams, imported—signify potential A USAF Major who served in probably “know MSA” because destruction of people, places, Egypt and Somalia is adamant they’ve worn our dependable, and ways of life we hold dear. -
RCT-APR-STP-0037Pdf Icon
National Institute for Occupational Safety and Health National Personal Protective Technology Laboratory P.O. Box 18070 Pittsburgh, PA 15236 Procedure No. RCT-APR-STP-0037 Revision: 1.1 Date: 28 June 2005 DETERMINATION OF α-CHLOROACETOPHENONE (CN) SERVICE LIFE TEST, AIR-PURIFYING RESPIRATORS STANDARD TESTING PROCEDURE (STP) Uncontrolled Copy 1. PURPOSE This test establishes the procedure for ensuring that the level of protection provided by the α-Chloroacetophenone (CN) service life requirements on gas mask and air-purifying respirators submitted for Approval, Extension of Approval, or examined during Certified Product Audits, Uncontrolledmeet the minimum certification standards set forth in 42Copy CFR Part 84, Subpart G, Section 84.63(a)(c)(d) and Subpart I, Section 84.110; Volume 60, Number 110, June 8, 1995. 2. GENERAL This STP describes the Determination of α-Chloroacetophenone (CN) Service Life Test, Air- UncontrolledPurifying Respirators test in sufficient detail that a person Copy knowledgeable in the appropriate technical field can select equipment with the necessary resolution, conduct the test, and determine whether or not the product passes the test. 3. EQUIPMENT/MATERIAL 3.1.Uncontrolled The list of necessary test equipment and materials follows: Copy 3.1.1. Miller Nelson Research Model 401 Flow-Temperature-Humidity Control System or equivalent. 3.1.2. UV Spectrophotometer, Spectronic Model 601 or equivalent. Uncontrolled Copy 3.1.3. Supelco Tenax- GC sample tubes custom made to the following specifications: 10cm long, 10 mm outside diameter, 8 mm inside diameter. Front section contains 70 mg. 35/60 mesh Tenax-GC; back section contains 35 mg. 35/60 Tenax-GC. -

Advantage® 1000 CBA-RCA and Millennium® Gas Masks
Advantage® 1000 CBA-RCA and Millennium® Gas Masks [ Designed for use by law enforcement and emergency personnel ] Advantage® 1000 CBA-RCA Millennium Chemical-Biological Gas Mask (Chemical/Biological Agent-Riot Control • Has flexible, one piece polyurethane lens with wide Agent) Gas Mask field of vision, bonded to a durable super-soft Hycar • Has flexible, one piece polyurethane lens with wide rubber facepiece. field of vision, bonded to a durable super-soft Hycar • Is NIOSH approved for protection against CN and rubber facepiece. CS tear gas. • Is NIOSH approved for protection against CN and • Is effective against, but does not have approval for CS tear gas. OC tear gas. • Is effective against, but does not have approval for • Is effective against biological agents and chemical OC tear gas. warfare agents. • Is effective against biological agents and chemical • Has dual-canister mount to allow weapon firing warfare agents. from either shoulder. • Has dual-canister mount to allow weapon firing • Has drinking tube to allow fluid ingestion in from either shoulder. contaminated atmospheres. Advantage® 1000 CBA-RCA Gas Mask The Advantage 1000 CBA-RCA Gas Masks are also effective The Advantage 1000 CBA-RCA Gas Masks from MSA are against biological agents, along with the following specifically designed for use by law enforcement and chemical warfare (CW) agents: GA, GB (Sarin), GD, VX, emergency response personnel. The facepiece features a Mustard, and Lewisite.Testing conducted by MSA and single low profile canister.The gas mask is NIOSH independent laboratories assures that the gas mask and approved (No.TC-14G-0235) for protection against canister meet the requirements for effectiveness against chloroacetphenone (CN), chlorobenzylidene (CS), P100 CW agents using the test protocol recommended by the particulate efficiency level and particulates. -
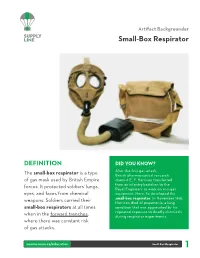
Small-Box Respirator
Artifact Backgrounder Small-Box Respirator DEFINITION DID YOU KNOW? Aer the first gas attack, The small-box respirator is a type British pharmaceutical research of gas mask used by British Empire chemist E. F. Harrison transferred from an infantry battalion to the forces. It protected soldiers’ lungs, Royal Engineers to work on anti-gas eyes, and faces from chemical equipment. Here, he developed the small-box respirator. In November 1918, weapons. Soldiers carried their Harrison died of pneumonia, a lung small-box respirators at all times condition that was aggravated by his repeated exposure to deadly chemicals when in the forward trenches, during respirator experiments. where there was constant risk of gas attacks. warmuseum.ca/education Small-Box Respirator HISTORICAL CONTEXT Gas warfare as we know it began in April 1915, at By the end of the war, some 124,000 tons of the Second Battle of Ypres, in Belgium. Looking chemical weapons were released by all sides. to break the stalemate of trench warfare, the In 1918, approximately 30 per cent of the artillery German Army released large volumes of deadly shells fired by Canadian artillery were packed chlorine gas. The wind carried the chlorine with gas. Although gas was a common element clouds across the positions of French, British and in most operations during the second half Canadian troops, none of whom were outfitted of the war, its impact was increasingly limited with anti-gas equipment. From 1915 onwards, by protective masks, such as the small-box both sides used deadly gases as wartime respirator. Gas made the battlefield even more weapons. -

Respirator Fact Sheet
If I wear a Gas Mask correctly, am I completely use by workers to protect against workplace hazards. safe? Respirators certified by NIOSH will say "NIOSH The filter cartridges protect against only certain Approved" and may have a certification number. inhaled airborne substances. Some dangerous chemi- However, NIOSH only certifies respirators against TM cals are absorbed through the skin. Properly selected specific hazards. Just because a respirator is certified and worn gas masks and escape respirators must be does not mean it will protect against ALL hazards. combined with protective clothing to completely pre- NIOSH-certified respirators are supplied with vent injury from these chemicals. Approval Labels that identify the hazards that the res- pirator is approved to protect against. If you are buy- Respirator Fact Sheet ing a respirator, you should check the Approval Label What you should know in deciding whether to buy escape hoods, gas masks, or other respirators for Will a Gas Mask protect me if there is not to be sure that it has been certified against the hazards preparedness at home and work enough oxygen in the air? you want protection against. Gas Masks do not provide oxygen. If used in an envi- ronment with low oxygen levels, such as a fire, you are The questions you should ask about any respira- in danger of suffocation. tor you are considering purchasing: Some employers and consumers are considering purchasing escape hoods or other respirators What protection (which chemicals and particles, and to protect themselves against potential terrorist threats, including biological and chemical sub- Will a Gas Mask protect me if there is a fire? at what levels) does the escape hood provide? It's important to read the manufacturer's information stances. -
Fm ' -P—Í3 Yj Reference C H FM 3-8 N DEPARTMENT 0F the ARMY FIELD MANUAL
408.3 A1 fM ' -p—Í3 yJ Reference C h FM 3-8 N DEPARTMENT 0F THE ARMY FIELD MANUAL CHEMIC REFERENCE RAN0B00K •tes OF*i HEADQUARTERS, DEPARTMENT OÍ\THE ARMY # A P R I L 1 9 6 3 An FM 3-8 FIELD MANUAL HEADQUARTERS, DEPARTMENT OF THE ARMY No. 3-8 WASHINGTON 25, D.C., 7 May 1963 CHEMICAL CORPS REFERENCE HANDBOOK CHAPTER 1. INTRODUCTION... 1.1-1.4 3 2. ORGANIZATION Section I. General 2.1-2.5 5 II. Characteristics of chemical units 2.6, 2.7 6 III. Major mission equipment 2.8, 2.9 12 IV. Characteristics of composite service organization teams. _ 2.10 19 CHAPTER 3. OPERATIONS Section I. Troop planning 3.1-3.4 21 II. Troop movements 3.5-3.11 22 III. Chemical training 3.12-3.15 43 IV. Characteristics of chemical agents, chemical-filled munitions, and chemical equipment 3.16-3.21 44 V. Chemical landmines • 3.22,3.23 87 VI. Flame fuel 3.24 88 CHAPTER 4. CHEMICAL SUPPLY AND MAINTENANCE Section I. Introductory information 4.1-4.8 89 II. Requirements.. 4.9-4.22 91 III. Class V basic load for chemical units 4.23-4.25 108 IV. Protection and identification equipment 4.26-4.31 109 V. Class III smoke agents. 4.32 115 VI. Water supply ' 4.33,4.34 115 VII. Storage and handling of supplies 4.35-4.41 117 VIII. Maintenance 4.42-4.49 118 CHAPTER 5. CHEMICAL SERVICE Section I. Decontamination 5.1-5.6 123 II. -

Millennium® Gas Mask
Millennium® Gas Mask The MSA Millennium Gas Mask Answers the Call The MSA Millennium CBRN Gas Mask meets or exceeds all performance requirements of the NIOSH CBRN Standard by effectively removing harmful gases, vapors and particulates so that the user can confidently breathe safely. The Millennium CBRN canister contains chemical sorbents and a P100 filter to attract, retain, and neutralize contaminants. The Millennium CBRN design is based on a highly successful military gas mask. The wearer enjoys a wide field of view and great flexibility, making it possible to safely perform any tasks required, including firing weapons if needed. The wearer can communicate easily while wearing the Millennium CBRN Gas Mask, too. The mask is lightweight and provides a tight seal on the face. A nose cup is also incorporated for reduced fogging of the facepiece. The material is impermeable to chemical agents such as mustard (HD), providing maximum assurance to the wearer. Riot Control Canisters are also available which protect against common riot control agents such as CN/CS and OC. The Millennium is also approved with a P100 filter for particulate/aerosol protection. CBRN ENCOMPASSES CHEMICAL, BIOLOGICAL, RADIOLOGICAL AND NUCLEAR AGENTS – AIRBORNE HAZARDS WHICH COULD BE USED AS WEAPONS IN A TERRORIST ATTACK. Canister Test Challenge and Test Breakthrough Concentrations* (NIOSH) CBRN STANDARD FOR FULL-FACEPIECE GAS MASKS Concentration (ppm) Test Breakthrough • Chemical, biological, radiological and nuclear agents Ammonia 2500 12.5 ppm • Mask penetration and