2021 Summary of Benefits
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Senior Resource Guide
SENIOR RESOURCE GUIDE Non-Profit and Public Agencies Serving NORTH ALAMEDA COUNTY Alameda ● Albany ● Berkeley ● Emeryville ● Oakland ● Piedmont Senior Information & Assistance Program – Alameda County Area Agency on Aging 6955 Foothill Blvd, Suite 143 (1st Floor), Oakland, CA 94605; 1-800-510-2020 / 510-577-3530; http://seniorinfo.acgov.org Office Hours : 8:30am – 4pm Monday – Friday ADULT DAY CARE/RESPITE (useful website: www.daybreakcenters.org): Alzheimer's Services of the East Bay - ASEB, Berkeley, www.aseb.org .................................................................................................................................... 510-644-8292 Bay Area Community Services - BACS, Oakland, http://bayareacs.org ................................................................................................................................... 510-601-1074 Centers for Elders Independence - CEI, (PACE - Program of All-inclusive Care for the Elderly); www.cei.elders.org ..................................................... 844-319-1150 DayBreak Adult Care Centers, (personalized referrals & community education); http://daybreakcenters.org ................................................................ 510-834-8314 Hong Fook Adult Day Health Care, Oakland, (14th Street site); www.fambridges.org ........................................................................................................ 510-839-9673 Hong Fook Adult Day Health Care, Oakland, (Harrison Street site); www.fambridges.org ................................................................................................ -

Senior Resource Guide for Central County
Senior Resource Guide for Central County Nonprofit and Public Agencies Serving Castro Valley ● Hayward ● San Leandro ● San Lorenzo Alameda County Area Agency on Aging 6955 Foothill Boulevard, 3 rd Floor, Oakland CA 94605, 1-800-510-2020 / 510-577-3530 http://alamedasocialservices.org (Revised 10/2010) ADULT DAY CARE/RESPITE (useful web site: www.adsnac.org ) Adult Day Services Network of Alameda County (personalized referrals & community education) ... 510-883-0874 Alzheimer’s Services of the East Bay Adult Day Health Care, Hayward.............................. 510-888-1411 Bay Area Community Services Adult Day Care (serves Hayward) , Fremont............................ 510-656-7742 Center for Elders Independence (PACE—A Program of All-inclusive Care for the Elderly) . 510-433-1150 LifeLong Medical Care Adult Day Health Care, East Oakland............................................. 510-563-4390 St. Peter’s Community Adult Day Care, San Leandro ......................................................... 510-562-4037 ALCOHOLISM & DRUG ABUSE PREVENTION PROGRAMS Alameda County Health Care ACCESS (referrals to substance abuse services in Alameda County) .. 1-800-491-9099 Alcoholics Anonymous Central Office, Oakland .................................................................. 510-839-8900 CommPre, a program of Horizon Services, Inc. (Prevention strategies to reduce alcohol and medication misuse among older adults) .......................... 510-885-8743 ALZHEIMER’S SERVICES Alzheimer’s Association Helpline ....................................................................................... -

Director of Marketing and Communications at Visit Stockton Stockton, California (Northern California/Central Valley)
Director of Marketing and Communications at Visit Stockton Stockton, California (Northern California/Central Valley) Visit Stockton.org [email protected] About Stockton, CA: Stockton is the county seat for San Joaquin County. The City of Stockton continues to be one of California’s fastest growing communities. Stockton is currently the 13th largest city in California with a dynamic, multi-ethnic and multi-cultural population of about 310,000. It is situated along the San Joaquin Delta waterway which connects to the San Francisco Bay and the Sacramento and San Joaquin Rivers. Stockton is located 60 miles east of the San Francisco Bay Area, 83 miles east of San Francisco, and 45 miles south of Sacramento, the capital of California. Stockton has an airport offering service to Phoenix and Las Vegas (on Allegiant Airlines). Visitors may also fly into Sacramento, Oakland or San Francisco. In the mid-2000’s Stockton underwent a tremendous economic expansion and continues to aggressively revitalize its downtown. Projects in the downtown area along the waterfront include an indoor arena, baseball stadium and waterfront hotel. The Bob Hope (Fox) California Theatre, listed on the National List of Historic hosts live performances regularly. The arena is home to the Stockton Kings (NBA G-League) basketball team, the Stockton Heat (AHL) Hockey team, as well as year-round family and cultural events and concerts. Adjacent to the Stockton Arena is the Stockton Ballpark, home of the Stockton Ports Single A Baseball Team (Oakland A’s affiliate). Stockton offers an excellent quality of life for its residents. The City has a number of beautiful residential communities along waterways, with single-family homes costing about one-third the price of homes in the Bay Area. -

2019 Northern California Kaiser Foundation Health Plan Provider
2. Key Contacts 2.1 Northern California Region Key Contacts Department Area of Interest Contact Information KP MSCC Membership Information (888) 576-6789 (Member cost General enrollment questions share and eligibility verification) Eligibility and benefit verification Weekdays : 8a-5p Pacific Co-pay, deductible and co-insurance information Members presenting without KP identification IVR System available number 24 hours / 7 days a week Verifying Member’s PCP assignment Member grievance and appeals Payment status on submitted claims Medical Services Contracting Contract Network Development and Provider (844) 343-9370 Network Management (510) 987-4138 (fax) • Updates to Provider demographics, such as Tax ID, address, and ownership changes P.O. Box 23380 • Practitioner additions/terminations to/from Oakland, CA 94623-2338 your group • Provider education and training • Contract interpretation • Form requests Quality & Operations Support Practitioner Credentialing (510) 625-5608 Medical Services Contracting Facility/Organizational Provider Credentialing (844) 343-9370 Medical Staff Office Kaiser Foundation Hospital Privileges Facility Listing – Section 2.4 Outside Medical Services Authorizations, Referrals by Service • Authorizations, referrals & billing questions for referred services Referral Coordinators - • Coordination of Benefits Facility Listing - Section 2.4 • Third Party Liability • Workers’ Compensation National Claims Emergency Medical Claims (non-Medicare) (800) 390-3510 Administration Billing questions for emergency (non-referred) -

SANTA CLARA Kaiser Foundation Hospital – Northern California Region
SANTA CLARA Kaiser Foundation Hospital – Northern California Region 2019 COMMUNITY BENEFIT YEAR-END REPORT AND 2017-2019 COMMUNITY BENEFIT PLAN Submitted to the Office of Statewide Health Planning and Development in compliance with Senate Bill 697, California Health and Safety Code Section 127350. 2019 Community Benefit Year-End Report Kaiser Foundation Hospital-Santa Clara Northern California Region Kaiser Foundation Hospital (KFH)-Santa Clara Table of Contents I. Introduction and Background A. About Kaiser Permanente B. About Kaiser Permanente Community Health C. Purpose of the Report II. Overview of Community Benefit Programs Provided A. California Kaiser Foundation Hospitals Community Benefit Financial Contribution – Tables A and B B. Medical Care Services for Vulnerable Populations C. Other Benefits for Vulnerable Populations D. Benefits for the Broader Community E. Health Research, Education, and Training Programs III. KFH-Santa Clara Community Served A. Kaiser Permanente’s Definition of Community Served B. Map and Description of Community Served C. Demographic Profile of Community Served IV. KFH-Santa Clara Community Health Needs Addressed in 2017-2019 A. Health Needs Addressed and Strategies to Address Those Needs B. Health Needs Not Addressed and Rationale V. 2019 Year-End Results for KFH-Santa Clara C. 2019 Community Benefit Programs Financial Resources Provided by KFH-Santa Clara – Table C D. 2019 Examples of KFH-Santa Clara Grants and Programs Addressing Selected Health Needs VI. Community Health Needs KFH-Santa Clara Will Address In 2020-2022 1 2019 Community Benefit Year-End Report Kaiser Foundation Hospital-Santa Clara Northern California Region I. Introduction and Background A. About Kaiser Permanente Founded in 1942 to serve employees of Kaiser Industries and opened to the public in 1945, Kaiser Permanente is recognized as one of America’s leading health care providers and nonprofit health plans. -
FINAL OAK-SFO Noise Proposals-3-13-17
OAKLAND AIRPORT-COMMUNITY NOISE MANAGEMENT FORUM An Advisory Body to the Executive Director of the Port of Oakland March 24, 2017 Co-Chairs Benny Lee, Mr. Dennis Roberts, Regional Administrator Elected- Federal Aviation Administration representative Western-Pacific Region City of San Leandro P.O. Box 92007 Walt Jacobs, Los Angeles, CA 90009 Citizen- representative RE: Recommendations to Adjust/Revise Metroplex Procedures Affecting East City of Alameda Bay Communities Members Dear Administrator Roberts: City of Alameda Long standing issues with, and changes to the San Francisco Bay Area airspace as a City of Berkeley result of implementation of the Northern California Metroplex in November 2014 have City of Hayward resulted in significant increases in noise complaints from affected communities in the East Bay region of the San Francisco Bay Area, primarily Alameda and Contra Costa City of Oakland Counties. The Oakland Airport-Community Noise Management Forum (Forum) serves as an advisory body on community noise concerns to the Executive Director of the Port City of San Leandro of Oakland and includes one elected official and one community member each from six City of Union City neighboring cities, as well as Alameda County. The Forum represents a combined regional population of almost 2 million people. County of Alameda Community issues and concerns over the implementation of certain NextGen air traffic Port of Oakland management procedures were brought to the attention of your immediate predecessor, Forum Facilitator former FAA Regional Administrator Mr. Glen A. Martin. In response to consultations with, and at the behest of Mr. Martin, the Forum accepted the role as the link to the Michael R. -

Three-Dimensional Geologic Modeling of the Santa Rosa Plain, California
Three-dimensional geologic modeling of the Santa Rosa Plain, California Donald S. Sweetkind* U.S. Geological Survey, Denver Federal Center, Mail Stop 973, Denver, Colorado 80225, USA Emily M. Taylor U.S. Geological Survey, Denver Federal Center, Mail Stop 980, Denver, Colorado 80225, USA Craig A. McCabe ESRI, 380 New York Street, Redlands, California 92373, USA Victoria E. Langenheim U.S. Geological Survey, Mail Stop 989, 345 Middlefi eld Road, Menlo Park, California 94025, USA Robert J. McLaughlin U.S. Geological Survey, Mail Stop 973, 345 Middlefi eld Road, Menlo Park, California 94025, USA ABSTRACT lence of the clay-rich Petaluma Formation Formation (Fig. 1). Although the outcrop dis- and its heterogeneous nature. Isopach maps tribution of each of these formations has been New three-dimensional (3D) lithologic and of the Glen Ellen Formation and the 3D mapped (e.g., Blake et al., 2002; Wagner et stratigraphic models of the Santa Rosa Plain stratigraphic model show the infl uence of the al., 2006; Graymer et al., 2007), the degree of (California, USA) delineate the thickness, Trenton Ridge, a concealed basement ridge subsurface interfi ngering and overlapping age extent, and distribution of subsurface geo- that bisects the plain, on sedimentation; the relations of the Miocene and Pliocene marine logic units and allow integration of diverse thickest deposits of the Glen Ellen Formation and nonmarine units have only recently been data sets to produce a lithologic, strati- are confi ned to north of the Trenton Ridge. recognized and have important signifi cance for graphic, and structural architecture for the the hydrogeologic system. -

Visit Tri-Valley REGIONAL TOURISM ASSET ASSESSMENT
Visit Tri-Valley REGIONAL TOURISM ASSET ASSESSMENT Prepared for: Visit Tri-Valley 5075 Hopyard Rd, Suite 240 Pleasanton, CA 94588 Solutions for your competitive world. Visit Tri-Valley Table of Contents Executive Summary 3 Part 1: Understanding Tourism Assets 7 Part 2: Existing Regional Assets 13 Part 3: Pipeline Projects 21 Part 4: Tri-Valley Tourism Asset Gaps 23 Part 5: Developing a Tourism Asset Strategy 44 Part 6: Summary Comments 45 Appendix 46 Appendix 1: Completed interviews 47 Appendix 2: Sources 48 Appendix 3: Project Overview 49 Appendix 4: Scope of Work 50 2 | P a g e Visit Tri-Valley Executive Summary The following report was developed in an effort to improve Tri-Valley’s long term competitive position in the Northern California tourism market> the report sought to identify current tourism related destination assets as more importantly potential tourism asset gaps. The report also seeks to define a tourism strategy that can improve the competitive position of Tri Valley over the long term. The report identifies several key challenges including the lack of perception the region has as a destination and that it is seen by some to be a series of communities. Additionally, the areas have significant differences between them. For example, Livermore, with its downtown area and wineries, is a very different experience to San Ramon, which generates a significant level of corporate travel. Moving forward Tri-Valley needs to consider three specific steps with regard to its assets. 1. Continue to build its brand assets in order to create value for all of the areas within the region. -
1.7.3 Project Environmental Impact Report
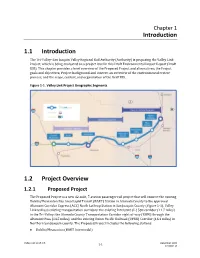
Chapter 1 Introduction 1.1 Introduction The Tri-Valley–San Joaquin Valley Regional Rail Authority (Authority) is proposing the Valley Link Project, which is being evaluated on a project level in this Draft Environmental Impact Report (Draft EIR). This chapter provides a brief overview of the Proposed Project and alternatives; the Project goals and objectives; Project background and context; an overview of the environmental review process; and the scope, content, and organization of the Draft EIR. Figure 1-1. Valley Link Project Geographic Segments 1.2 Project Overview 1.2.1 Proposed Project The Proposed Project is a new 42-mile, 7-station passenger rail project that will connect the existing Dublin/Pleasanton Bay Area Rapid Transit (BART) Station in Alameda County to the approved Altamont Corridor Express (ACE) North Lathrop Station in San Joaquin County (Figure 1-1). Valley Link will use existing transportation corridors: the existing Interstate (I-) 580 corridor (11.7 miles) in the Tri-Valley; the Alameda County Transportation Corridor right-of-way (ROW) through the Altamont Pass (14.5 miles); and the existing Union Pacific Railroad (UPRR) Corridor (16.1 miles) in Northern San Joaquin County. The Proposed Project includes the following stations: ⚫ Dublin/Pleasanton (BART Intermodal) Valley Link Draft EIR 1-1 December 2020 ICF 00004.19 Tri-Valley – San Joaquin Valley Regional Rail Authority Introduction ⚫ Isabel (Livermore) ⚫ Greenville (Livermore) ⚫ Mountain House (San Joaquin County) ⚫ Downtown Tracy Station (Tracy) ⚫ River Islands Station (Lathrop) ⚫ North Lathrop Station (ACE Intermodal) The Proposed Project also includes the proposed Tracy Operation and Maintenance Facility (OMF), which would be located in the City of Tracy. -

THE NORTHERN CALIFORNIA MEGAREGION We’Ve Outgrown the Original Boundaries of the Bay Area
THE NORTHERN CALIFORNIA MEGAREGION We’ve outgrown the original boundaries of the Bay Area. It’s time to start solving problems at the scale of the megaregion. SPUR ARTICLE This article originally appeared in the November/December 2007 issue of The Urbanist. The primary authors of this article were Gabriel Metcalf and Egon Terplan SPUR 654 Mission St., San Francisco, California 94105 www.spur.org SPUR November 2007 INDEX Introduction _______________________________________________________________________ 3 Historic Relationships That Have Defined the Region _____________________________________ 6 Land Consumption 8 Transportation Flows and Commute Patterns 9 Economic Integration 10 Cultural Integration 11 Defining the Megaregion ____________________________________________________________ 12 Solving Problems at the Megaregional Scale ___________________________________________ 13 A Northern California Rail Network 13 A Landscape Preservation Campaign for the Central Valley 15 An Equity Agenda for Northern California 17 Conclusion _______________________________________________________________________ 21 Appendix I: Mapping the Megaregion _________________________________________________ 22 Appendix II: History of the Megaregion Concept ________________________________________ 35 Appendix III: An Example of Megaregional Planning: The Regional Rail Plan ________________ 37 The Northern California Megaregion 2 INTRODUCTION The United States population is projected to grow by more than 45 percent in the next half-century. The total population -

Senior Resource Guide for North County
Senior Resource Guide for North County Nonprofit and Public Agencies Serving Alameda Albany Berkeley Emeryville Oakland Piedmont Alameda County Area Agency on Aging 6955 Foothill Boulevard, 3rd Floor, Oakland CA 94605, 1-800-510-2020 / 510-577-3530 http://alamedasocialservices.org (Revised 10/2010) ADULT DAY CARE/RESPITE (useful web site: www.adsnac.org) Adult Day Services Network of Alameda County (personalized referrals & community education) ... 510-883-0874 Alzheimer’s Services of the East Bay Adult Day Health Care, Berkeley .............................. 510-644-8292 Alzheimer’s Services of the East Bay Adult Day Health Care, Oakland............................... 510-268-1410 Bay Area Community Services Adult Day Care, Oakland.................................................... 510-601-1074 Berkeley Adult Day Health Care, Berkeley.......................................................................... 510-601-0167 Center for Elders Independence (PACE—A Program of All-inclusive Care for the Elderly) . 510-433-1150 Hong Fook Adult Day Health Care, Oakland (14th Street site)............................................. 510-839-9673 Hong Fook Adult Day Health Care, Oakland (Harrison Street site) ..................................... 510-302-0460 LifeLong Medical Care Adult Day Health Care, Oakland..................................................... 510-563-4390 St. Peter’s Community Adult Day Care, San Leandro ......................................................... 510-562-4037 ALCOHOLISM & DRUG ABUSE PREVENTION PROGRAMS Alameda -

Central Valley Immigration Integration Collaborative
CENTRAL VALLEY IMMIGRATION INTEGRATION COLLABORATIVE (CVIIC) Nonprofit Organizations Providing Immigration Assistance or Information (11 28 17) Visit our website for a list of free application workshops in the region: ValleCentral.org To receive information about free immigration workshops text ValleCentral to 71441 ORGANIZATION OFFICES SERVICE P.O. Box 188 Know-your-rights issues; ACLU of Northern California Fresno, CA 93707 Immigrants’ Rights Issues; Constitutional Violations 2377 W Shaw Avenue Suite 204 Fresno, California Rural Legal CA 93728 Provides DACA and Assistance Foundation 559-486-6278 (CRLAF) Naturalization services. www.crlaf.org Central California Legal 2115 Kern St Fresno, Ca 93721 Naturalization (Citizenship) Services (CCLS) 559-570-1200 information and Services. FRESNO 744 N Abby St Fresno, CA 93701 Centro Binacional para el 559-499-1178 Information and Event Desarrollo Indígena Oaxaqueño MADERA Organization. (CBDIO) 14215 RD 28 Madera, CA. 93638 559-675-7893 DACA Services, Family Petitions, U Visa, VAWA, T 302 Fresno St, Suite 102, Fresno, CA Visa, Naturalization 93706 Centro La Familia Advocacy (Citizenship). Support 559-237-2961 Services services such as public benefits, breast cancer, www.centrolafamilia.org parenting classes and mental health. DACA Services (Initial and 4290 E. Ashlan Ave., Fresno, CA 93726 Education and Leadership renewal), adjustment of (559) 291-5428 Foundation (ELF) Status, and naturalization www.education-leadership.org (Citizenship). Locations in Fresno, Merced, and Bakersfield. Faith in the