A Time Series Analysis: Exploring the Link Between Human Activity and Blood Glucose Fluctuation
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Read an Extract from Lichfield and the Lands of St Chad
Contents List of illustrations vii General Editor’s preface ix Acknowledgements xi Abbreviations xii Introduction 1 Early medieval communities 2 The communities of the lands of St Chad 9 1 Lichfield and the English Church 11 The episcopal list tradition 12 Theodore’s church 19 Church and kingdom 21 The division of the Mercian see 26 The English Church and the Mercian kingdom 33 The English Church from the late ninth century 40 Conclusions 44 2 The Church of Lichfield 48 The Lastingham narrative 48 Bishop Chad and Bishop Wilfrid 54 The diocesan community 60 The Church of Lichfield and the diocesan community 80 3 The cathedral and the minsters 86 Hunting for minsters 87 Lichfield cathedral 110 Minsters attested by pre-c.1050 hagiography 123 Minsters attested by post-c.1050 hagiography 137 Minsters securely attested by stone sculpture 141 Minsters less securely attested 146 Minsters and communities 150 4 The bishop and the lords of minsters 156 Ecclesiastical tribute 157 Episcopal authority over the lords of minsters 166 Conclusions 175 5 The people 177 Agricultural communities and the historic landscape 177 Domainal communities and the possession of land 186 Brythonic place-names 190 Old English place-names 195 Eccles place-names 203 Agricultural and domainal communities in the diocese of Lichfield 206 6 The parish 216 Churches and parishes 217 Churches, estates and ‘regnal territories’ 225 Regnal territories and the regnal community 240 A parochial transformation 244 Conclusion 253 Bibliography 261 Index 273 Introduction This book explores a hole at the heart of Mercia, the great Midland kingdom of early medieval England. -
Catalogue of Adoption Items Within Worcester Cathedral Adopt a Window
Catalogue of Adoption Items within Worcester Cathedral Adopt a Window The cloister Windows were created between 1916 and 1999 with various artists producing these wonderful pictures. The decision was made to commission a contemplated series of historical Windows, acting both as a history of the English Church and as personal memorials. By adopting your favourite character, event or landscape as shown in the stained glass, you are helping support Worcester Cathedral in keeping its fabric conserved and open for all to see. A £25 example Examples of the types of small decorative panel, there are 13 within each Window. A £50 example Lindisfarne The Armada A £100 example A £200 example St Wulfstan William Caxton Chaucer William Shakespeare Full Catalogue of Cloister Windows Name Location Price Code 13 small decorative pieces East Walk Window 1 £25 CW1 Angel violinist East Walk Window 1 £50 CW2 Angel organist East Walk Window 1 £50 CW3 Angel harpist East Walk Window 1 £50 CW4 Angel singing East Walk Window 1 £50 CW5 Benedictine monk writing East Walk Window 1 £50 CW6 Benedictine monk preaching East Walk Window 1 £50 CW7 Benedictine monk singing East Walk Window 1 £50 CW8 Benedictine monk East Walk Window 1 £50 CW9 stonemason Angel carrying dates 680-743- East Walk Window 1 £50 CW10 983 Angel carrying dates 1089- East Walk Window 1 £50 CW11 1218 Christ and the Blessed Virgin, East Walk Window 1 £100 CW12 to whom this Cathedral is dedicated St Peter, to whom the first East Walk Window 1 £100 CW13 Cathedral was dedicated St Oswald, bishop 961-992, -

Weekly Newsletter St Joseph's and St Wilfrid's
Weekly Newsletter St Joseph’s and St Wilfrid’s A P ARISH OF T HE D I O CE SE OF H EXHAM & NE WCA ST L E R EGISTERED CHARITY NO.1143450 PARISH PRIEST: VERY REV DR MICHAEL BROWN PRESBYTERY: ST JOSEPH’S HIGH WEST STREET GATESHEAD NE8 1LX TELEPHONE NOS.: ST JOSEPH’S: 477 1631 ST WILFRID’S: 477 1631 http://www.stjosephscatholicchurchgateshead.org.uk/ BOOKINGS FOR ST JOSEPH’S HALL: 07989 734644 email: [email protected] Week Commencing 17th March 2019 St Patrick’s Day Second Sunday of Lent Saint Patrick’s Feast Day 17th March REMEMBER 19th March 6pm CMUK th 19 March 7pm High Mass Services for Bishop Robert’s Installation followed by shared table (all held at St Contrary to popular belief Ireland’s National Mary’s Cathedral) th colour has not always been green. Saint 20 March 10am th th Sunday 24 March - Patrick's colour was blue, and from the 12 Community 4.30 pm Solemn century blue adorned the Ancient Irish flags Choir Vespers and the Royal Court. Everybody in the 22nd March 5pm Diocese is invited to The Shamrock has always been the National Good attend. emblem of Ireland and its banning by the Shepherd for Monday 25th March English only served to strengthen its ages 3-6yrs - 12 noon Episcopal symbolism reflected in the green uniforms Installation Mass worn by Irish soldiers to show their solidarity Entry by invitation against the British who wore red. only, you will not be During the rebellion of 1798 the clover permitted without a ticket. -

Veterans Memorial (By Names & Numbers).Xlsx
Name Service Branch Conflict Monument ID# Entries Emblem at Top of Mon. Abbott, Donald H. US Army WWII 18-B-Right Col 9 3632 Disable American Veterans Abbott, James P. US Air Force Persian Gulf 18-B-Right Col 23 3646 Disable American Veterans Abbott, John D. US Air Force Vietnam 18-B-Right Col 21 3644 Disable American Veterans Abbott, John D. Jr. US Air Force Panama 18-B-Right Col 22 3645 Disable American Veterans Abbott, Robert P. US Marine Corps Vietnam 28-B-Left Col. 19 5748 Air National Guard Achorn, Richard L. US Navy WWII 8-A Right Col. 46 1612 POW-MIA Logo Adamen, Stanley M. US Army WWII 17-B-Left Col 14 3367 AMVETS Adams, Bernard L. Jr. US Army WWII 28-A-Left Col. 14 5635 Air National Guard Adams, Byron C. Jr. US Army WWII 11-B-Right Col. 44 2366 Veterans of Foreign Wars Adams, Garfield D. US Navy WWII 20-A-Right Col 10 3957 US Army WAC Logo Adams, Harold C. US Army WWII 22-A-Left Col 15 4340 US Navy Waves Adams, Harold F. US Army Vietnam 32-A-Right Col. 21 6560 Destroyer Escort Assoc. Adams, Preston G. US Navy WWII 21-A-Left Col 24 4133 US Air Force Women Adams, Ralph S. US Army Korea 2-B Right Col. 33 411 State of Maine Seal Adams, Richard C. US Army WWI 22-B-Left Col 11 4444 US Navy Waves Adams, Richard M. US Army WWII 10-B Right Col. 40 2146 Order of the Purple Heart Adams, Robert P. -
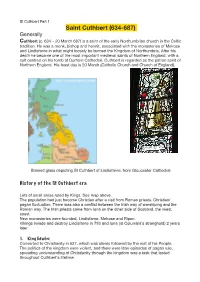
St Cuthbert Part 1 Saint Cuthbert (634-687) Generally Cuthbert (C
St Cuthbert Part 1 Saint Cuthbert (634-687) Generally Cuthbert (c. 634 – 20 March 687) is a saint of the early Northumbrian church in the Celtic tradition. He was a monk, bishop and hermit, associated with the monasteries of Melrose and Lindisfarne in what might loosely be termed the Kingdom of Northumbria. After his death he became one of the most important medieval saints of Northern England, with a cult centred on his tomb at Durham Cathedral. Cuthbert is regarded as the patron saint of Northern England. His feast day is 20 March (Catholic Church and Church of England), Stained glass depicting St Cuthbert of Lindisfarne, from Gloucester Cathedral History of the St Cuthbert era Lots of small areas ruled by Kings. See map above. The population had just become Christian after a visit from Roman priests. Christian/ pagan fluctuation. There was also a conflict between the Irish way of worshiping and the Roman way. The Irish priests came from Iona on the other side of Scotland, the /west coast. New monasteries were founded, Lindisfarne, Melrose and Ripon. Vikings invade and destroy Lindisfarne in 793 and Iona (st Columbia’s stronghold) 2 years later. 1. King Edwin: Converted to Christianity in 627, which was slowly followed by the rest of his People. The politics of the kingdom were violent, and there were later episodes of pagan rule, spreading understanding of Christianity through the kingdom was a task that lasted throughout Cuthbert's lifetime. Edwin had been baptised by Paulinus of York, an Italian who had come with the Gregorian mission from Rome. -
St. Oswald of Worcester Catholic.Net
St. Oswald of Worcester Catholic.net Roman Martyrology: King of Northumbria from 634 until his death, and is venerated as a saint, of which there was a particular cult in the Middle Ages. SHORT BIOGRAPHY Oswald was of a noble Saxon family, and was endowed with a very rare and beautiful form of body and with a singular piety of soul. He was brought up by his uncle, St. Odo, Archbishop of Canterbury, and was chosen, while still young, dean of the secular canons of Winchester, then very relaxed. His attempt to reform them was a failure; and he saw, with that infallible instinct which so often guides the Saints in critical times, that the true remedy for the corruptions of the clergy was the restoration of the monastic life. He therefore went to France and took the habit of St. Benedict, but returned, only to receive the news of Odo's death. He found, however, a new patron in St. Dunstan, now metropolitan, through whose influence he was nominated to the see of Worcester. To these two Saints, together with Ethelwold of Winchester, the monastic revival of the tenth century is mainly due. Oswald's first care was to deprive of their benefices the disorderly clerics, whom he replaced as far as possible by regulars, and himself founded seven religious houses. Considering that in the hearts of the secular canons there were yet some sparks of virtue, he would not at once expel them, but rather entrapped them by a holy artifice. Adjoining the cathedral he built a church in honor of the Mother of God, causing it to be served by a body of strict religious. -

69-19,257 STOLTZ, Linda Elizabeth, 1938- the DEVELOPMENT OF
THE DEVELOPMENT OF THE LEGEND OF ST. CUTHBERT Item Type text; Dissertation-Reproduction (electronic) Authors Stoltz, Linda Elizabeth, 1938- Publisher The University of Arizona. Rights Copyright © is held by the author. Digital access to this material is made possible by the University Libraries, University of Arizona. Further transmission, reproduction or presentation (such as public display or performance) of protected items is prohibited except with permission of the author. Download date 10/10/2021 21:02:21 Link to Item http://hdl.handle.net/10150/287860 This dissertation has been microfilmed exactly as received 69-19,257 STOLTZ, Linda Elizabeth, 1938- THE DEVELOPMENT OF THE LEGEND OF ST. CUTHBERT. University of Arizona, Ph.D., 1969 Language and Literature, general University Microfilms, Inc., Ann Arbor, Michigan THE DEVELOPMENT OP THE LEGEND OP ST. CUTHBERT by Linda Elizabeth Stoltz A Dissertation Submitted to the Faculty of the DEPARTMENT OF ENGLISH In Partial Fulfillment of the Requirements For the Degree of DOCTOR OF PHILOSOPHY In the Graduate College THE UNIVERSITY OF ARIZONA 19 6 9 THE UNIVERSITY OF ARIZONA GRADUATE COLLEGE I hereby recommend that this dissertation prepared under my direction by Linda Elizabeth Stoltz entitled The Development of the Legend of St. Cuthbert be accepted as fulfilling the dissertation requirement of the degree of Doctor of Philosophy LSIL jf/r. / /9/9 Disseycation Director Date After inspection of the final copy of the dissertation, the following members of the Final Examination Committee concur in its approval and recommend its acceptance:-• Z- y£~ ir ApJ /9S? $ Lin— • /5 l*L°l ^ ^7^ /(, if6? C^u2a,si*-> /4 /f(?,7 . -
The Cult of St Æthelwold and Its Context, C. 984 - C
The Cult of St Æthelwold and its Context, c. 984 - c. 1400 Rebecca Browett Institute of Historical Research School of Advanced Study, University of London A Thesis Submitted for the Degree of Ph.D in History September 2016 1 Declaration This thesis is submitted to the University of London in support of my application for the degree of Doctor of Philosophy. I, Rebecca Browett, hereby confirm that the work presented in this thesis is my own, carried out during the course of my studies. The copyright of this thesis rests with the author. Quotation from it is permitted, provided that full acknowledgement is made. This thesis may not be reproduced without the consent of the author. Signed: Date: 2 Abstract This thesis documents the cult of St Æthelwold, a tenth-century bishop of Winchester, from its inception (c. 984) until the late Middle Ages. During his life, Æthelwold was an authoritative figure who reformed monasteries in southern England. Those communities subsequently venerated him as a saint and this thesis examines his cult at those centres. In particular, it studies how his cult enabled monasteries to forge their identities and to protect their rights from avaricious bishops. It analyses the changing levels of veneration accorded to Æthelwold over a five hundred year period and compares this with other well-known saints’ cults. It uses diverse evidence from hagiographies, chronicles, chartularies, poems, church dedications, wall paintings, and architecture. Very few studies have attempted to chart the development of an early English saint's cult over such a long time period, and my multidisciplinary approach, using history, art, and literary studies, offers insight into the changing role of native saints in the English church and society over the course of the Middle Ages. -

Msdep1980 1 Ripon Index (148Kb)
Handlist 47 APPENDIX III. PRINTED TEXTS CITED Ripon Chapter Acts Acts of Chapter of the Collegiate Church of SS. Peter and Wilfrid, Ripon AD 1452 to AD 1506; [edited by J T Fowler]. (Surtees Society volume 4). 1875 Memorials of Ripon Memorials of the Church of SS Peter and Wilfrid, Ripon; [edited by J T Fowler]. (Surtees Society, volumes 74, 78, 81, 115) 1882, 1884, 1888, 1908. INDEX Abbott, Christopher letter to, 4 September 1827 397.2 Act books 39-50 extracts from 448.2 Acts of Parliament see Parliament Adam (Sawley chapel) 356, p 57 Advocate General Opinion (1844) 21.1, 200.1 Affidavits of burials in woollen 113, 446 Affidavits of debt (Canon Fee Court) (1733-57) 327.1 (1758-1817) 335 Agarde, Arthur (1579) 370(5(f)) Aislabie, Mr. (1782) 381.2; William 389, p 90-91 Aismunderby, chapel of St John the Baptist 356, p 43-44 Easter dues (1661) 366.17 land 356, p 43-44; (1140) 370(5(b)) map of George Dawson's estates, 1619 366 property leases (1571-1636) 360.9 tenants (1461) 370(5(d)) (tithe) apportionments 400.1 tithes (1623) 366.4 Aismunderby, Lady Emma of 356, p 44 Alan 356,p29 Alan, canon 356, p 30 Alan, lord, of Aldfield 356, p 24 Alan, son of John Delat 356, p 8 Alben,Rogerof 356,p43-44 Aldbrough in Holderness tithes, 1795 425.1 Aldburgh tithes 356, p 5 Aldfield, chapel baptisms (1816-1838) 126-128 burials (1818-1839) 152-3 returns of register entries, 1839 157 chapel of St Laurence the Martyr 356, p 27-28 right of presentation to (1724-1744) 260.5 chantry chaplain 356 111 Handlist 47 pastoral supervision (3 November 1942) 278.12 Aldfield,LordAlanof -

“Æthelthryth”: Shaping a Religious Woman in Tenth-Century Winchester" (2019)
University of Massachusetts Amherst ScholarWorks@UMass Amherst Doctoral Dissertations Dissertations and Theses August 2019 “ÆTHELTHRYTH”: SHAPING A RELIGIOUS WOMAN IN TENTH- CENTURY WINCHESTER Victoria Kent Worth University of Massachusetts Amherst Follow this and additional works at: https://scholarworks.umass.edu/dissertations_2 Part of the Feminist, Gender, and Sexuality Studies Commons, History Commons, History of Art, Architecture, and Archaeology Commons, Literature in English, British Isles Commons, Medieval Studies Commons, Other English Language and Literature Commons, and the Religion Commons Recommended Citation Worth, Victoria Kent, "“ÆTHELTHRYTH”: SHAPING A RELIGIOUS WOMAN IN TENTH-CENTURY WINCHESTER" (2019). Doctoral Dissertations. 1664. https://doi.org/10.7275/13999469 https://scholarworks.umass.edu/dissertations_2/1664 This Open Access Dissertation is brought to you for free and open access by the Dissertations and Theses at ScholarWorks@UMass Amherst. It has been accepted for inclusion in Doctoral Dissertations by an authorized administrator of ScholarWorks@UMass Amherst. For more information, please contact [email protected]. “ÆTHELTHRYTH”: SHAPING A RELIGIOUS WOMAN IN TENTH-CENTURY WINCHESTER A Dissertation Presented By VICTORIA KENT WORTH Submitted to the Graduate School of the University of Massachusetts Amherst in partial fulfillment of the requirements for the degree of DOCTOR OF PHILOSOPHY May 2019 Department of English © Copyright by Victoria Kent Worth 2019 All Rights Reserved “ÆTHELTHRYTH”: SHAPING -

ABSTRACT Whitby, Wilfrid, and Church-State Antagonism in Early
ABSTRACT Whitby, Wilfrid, and Church-State Antagonism in Early Medieval Britain Vance E. Woods, M.A. Mentor: Charles A. McDaniel, Ph.D. In 664, adherents of the Dionysian and Celtic-84 Easter tables gathered at the Northumbrian abbey of Whitby to debate the proper calculation of Easter. The decision to adopt the former, with its connections to the papacy, has led many to frame this encounter in terms of Roman religious imperialism and to posit a break between the ecclesiastical culture of Northumbria prior to the Synod of Whitby and afterward. This study will propose a different interpretation of the change that took place in the Northumbrian Church after 664. Rather than focusing solely on matters of religion, this project will seek also to demonstrate Whitby’s political implications. Instead of the end of alienation between the Celtic Church and the balance of Christendom, the Synod of Whitby will be identified, in the person of its main protagonist Wilfrid, as the beginning of alienation between the Northumbrian state and the hierarchy of the Church. Whitby, Wilfrid, and Church-State Antagonism in Early Medieval Britain by Vance E. Woods, B.A. A Thesis Approved by the J.M. Dawson Institute of Church-State Studies ___________________________________ Christopher Marsh, Ph.D., Chairperson Submitted to the Graduate Faculty of Baylor University in Partial Fulfillment of the Requirements for the Degree of Master of Arts Approved by the Thesis Committee ___________________________________ Charles A. McDaniel, Ph.D., Chairperson ___________________________________ Beth Allison Barr, Ph.D. ___________________________________ Daniel Payne, Ph.D. Accepted by the Graduate School May 2009 ___________________________________ J. -

Saints and Their Function in the Kingdom of Mercia, 650-850
SAINTS AND THEIR FUNCTION IN THE KINGDOM OF MERCIA, 650-850 By WILLIAM MICHAEL FRAZIER Bachelor of Science Oklahoma State University Stillwater, Oklahoma 1995 Submitted to the Faculty of the Graduate College of the Oklahoma State University in partial fulfillment of the requirements for the degree of MASTER OF ARTS December, 1998 SAINTS AND THEIR FUNCTION IN THE KINGDOM OF MERCIA, 650-850 Thesis Approved: Dean ofthe Graduate College ACKNOWLEDGMENTS I would like to express my deepest appreciation to my advisor, Dr. J. Paul Bischoff, for his guidance throughout the creation ofthis thesis. Without his suggestions and criticisms, I would have never completed a work worth submitting. To Dr Bischoff I also owe thanks for giving me something I have rarely had in my life: a challenge. I would also like to thank my other commi.ttee members, Dr. Eldevik and Dr. Petrin, who gave me many valuable suggestions during the revision ofthe thesis. Any mistakes that remain after their help are without a doubt my own. I truly appreciate the support which the History department extended to me, especially the financial support ofthe Teaching Assistantship I was generously given. To the wonderful people of the interlibrary loan department lowe an enormous debt. I simply could not have completed this work without the many articles and books which they procured for me. I would also like to thank my parents, Ron and Nancy, for their constant support. Anything good that I achieve in this life is a reflection on them. They have made me who I am today. Finally, I would like to extend my greatest appreciation to my wife, Cindy, who has stayed supportive throughout what has seemed an eternity of research and writing.