Treatment Standards
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Glossary of Dental Terms
1 GLOSSARY OF DENTAL TERMS A PATIENT’S DENTAL PRIMER Amalgam - Silver filling. Bonding - Method of adhering a filling ( amalgam or composite ) to a tooth. Uses a white light to harden the material. Bridge - A cemented structure used to replace missing teeth. Composed of several caps soldered together using a pontic to replace the missing tooth. Calculus -Tartar, a hard substance that forms on the teeth. Once formed, it must be professionally removed. Composite - White filling used in front or back teeth. Crown - 1. Same thing as a cap. Can be all metal ( either gold or a combination of other met- als) or a combination of metal and an esthetic material such as porcelain. 2. The part of the tooth that is visible in the mouth. Denture - A Removable Prosthesis - can be either a full or partial ( replaces a few or several teeth) denture. Sometimes called a ' plate '. Should not be confused with a bridge. Endodontist - A dentist that specializes in performing root canal therapy. Explorer - The pointed instrument used during the examination. Frenum - The little piece of tissue which goes from the inside of your lip to the gum tissue just above your front teeth. There is also a frenum which goes from the under surfac your tongue to the bottom of your mouth. Frenum are not essential structures and very often need to be removed if they are causing physical or esthetic problems. Gingiva - Gum tissue. Inflammation - Red, sore, puffy bleeding gums tissue. Due to the accumulation of bacteria and lack of required home care. Inlay/Onlay - A type of restoration that replaces a part of the tooth. -

Pdf (930.25 K)
EGYPTIAN Vol. 64, 951:962, April, 2018 DENTAL JOURNAL I.S.S.N 0070-9484 Orthodontics, Pediatric and Preventive Dentistry www.eda-egypt.org • Codex : 214/1804 CLINICAL AND RADIOGRAPHIC ASSESSMENT OF PULPOTOMY MATERIALS IN PRIMARY MOLARS Gihan Abuelniel* and Sherif Eltawil* ABSTRACT Aim or purpose: Clinical and radiographic evaluation of four different materials utilized in vital pulpotomy in mandibular primary molars Materials and methods: one hundred and sixty mandibular primary molars in forty children were included as split mouth design. Patients were medically free with an age range from 4-6 years. Inclusion criteria: patients presented with deep carious lesions including the first and second primary molars bilaterally, no evidence of any clinical pathology, mobility and had no tenderness to percussion. Pre-operative radiographs showed no evidence of external or internal root resorption, absence of furcal, periapical radiolucency or widened periodontal ligament space and no more than one-third root resorption detected. The included molars undergone vital pulp therapy and bilaterally randomly divided into four equal groups, group (1) formocresol, group (2) ferric sulphate, group (3) MTA (mineral trioxide aggregate) and group (4) Metapex (calcium hydroxide &iodoform). All treated molars were evaluated both clinically and radiographically for 12 months evaluation period. Data were collected and analysed statistically. Results: It was shown that, at base line, there was no statistically significant difference between clinical as well as radiographic success rates among the four groups. After 3 as well as 6 months, there was a statistically significant difference between clinical and radiographic success rates among the four groups. FS, MTA and Metapex groups showed higher clinical and radiographic success rates than FC group. -

The Evolution of Surgical Endodontics: Never and Always Prof. Marwan Abou-Rass DDS, MDS, Ph.D
The Evolution of Surgical Endodontics: Never and Always Prof. Marwan Abou-Rass DDS, MDS, Ph.D Introduction This paper came out of discussions with Hu-Friedy as we were developing new materials describing the Marwan Abou-Rass, or “MAR” microsurgical endodontic instrument line. Since I have been teaching, conducting research and performing microsurgical endodontics for many years, Hu-Friedy was interested in my perspective on the evolution of the specialty, and what the future might hold. I tried to fit it all in the sales brochure we were working on, but how can one compress decades of change into a few short paragraphs? Hence, we decided to make it a separate venture. Since graduating from dental school and completing my endodontic training, I have been immersed in university environments where dialog regarding best practices in endodontics can be collaborative, and sometimes heated -- because my academic and clinical peers are passionate about what we do. Throughout my career I have collaborated with many global peers who have combined innovation and critical thinking with willingness to risk being “wrong”. As a result, the profession has made significant advances for which we have all benefited. It is for them that I dedicate this paper. This paper outlines my perspective on how microsurgical endodontics has progressed over several decades, from its infancy in the 1940s, through developments which have shaped the practice today. I conclude with “educated guesses” regarding what the future may hold. I. The Influence of Oral Surgery Period In the 1940s, endodontic surgery was often performed by oral surgeons, adapting their methods and instruments used for oral surgery. -
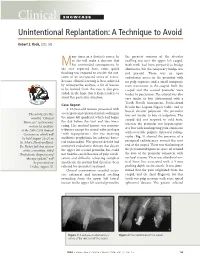
Clinical SHOWCASE Unintentional Replantation: a Technique to Avoid
Clinical SHOWCASE Unintentional Replantation: A Technique to Avoid Robert S. Roda, DDS, MS any times in a dentist’s career, he the greatest contour of the alveolar or she will make a decision that swelling was over the upper left cuspid. Mhas unintended consequences. In Both teeth had been prepared as bridge the case reported here, some quick abutments, but the temporary bridge was thinking was required to resolve the out- not present. There was an open come of an unexpected series of events. endodontic access in the premolar with Because clinical learning is best achieved no pulp exposure and a small composite by retrospective analysis, a list of lessons resin restoration in the cuspid. Both the to be learned from this case is also pro- cuspid and the second premolar were vided, in the hope that it helps readers to tender to percussion. The cuspid was also avoid this particular situation. very tender to bite (determined with a Tooth Slooth instrument, Professional Case Report Results Inc, Laguna Niguel, Calif.) and to A 63-year-old woman presented with buccal alveolar palpation. The premolar severe pain and extraoral facial swelling in The articles for this was not tender to bite or palpation. The the upper left quadrant, which had begun month’s “Clinical cuspid did not respond to cold tests, the day before the visit and was wors- Showcase” section were whereas the premolar was hyperrespon- ening. Her medical history was noncon- written by speakers sive but with nonlingering pain consistent at the 2006 CDA Annual tributory except for mitral valve prolapse with reversible pulpitis. -

Material Selection and Shade Matching for a Single Central Incisor
CLINICAL SCIENCE KAHNG Material Selection and Shade Matching for a Single Central Incisor INTRODUCTION With regard to esthetics, the single central incisor poses the greatest re- by storative challenge for the clinician; not surprisingly, it can also be the most Luke S. Kahng, C.D.T. difficult tooth for the dental technician to match. Selecting the shade of the restoration depends in part on the material used for the understructure, and Mr. Kahng is the founder and owner of there is a wide assortment available from which to choose. The following are Capital Dental Technology Laboratory, among the most common: Inc., in Naperville, Illinois. The labora- tory specializes in all fixed restorations and its LSK 121 division provides per- An experienced technician can mask the underlying dark tooth color using sonalized custom cosmetic work. A porcelains with detailed color-masking techniques. strong proponent of collaborative den- tistry, Mr. Kahng stresses education, communication, and a team approach to patient care. A member of the AACD, UNDERSTRUCTURE MATERIAL his training has included extensive study with Russell DeVreugd, C.D.T., Dr. • Zirconia (e.g., Procera® [Nobel Biocare; Yorba Linda, CA], Lava™ [3M Frank Spear, Dr. Peter Dawson, and ESPE, St. Paul, MN], Cercon® [Dentsply Int., York, PA], Everest™ [KaVo others. America Corp.; Lake Zurich, IL], In-Ceram® [Vident; Brea, CA]) Mr. Kahng is the official clinician for --Flexural strength: approximately 1,200 MPa GC America, Bisco, and Captek. He is --Translucency: very low a frequent lecturer and program facili- tator for dentists and dental technicians, --Opacity: high and has published articles in Practical • Alumina core or glass-infiltrated alumina (e.g., Procera, In-Ceram) Procedures and Aesthetic Dentistry --Flexural strength: 450 to 700 MPa and Dental Dialogue. -

New Treatment Option for an Incomplete Vertical Root Fracture-A
Hadrossek and Dammaschke Head & Face Medicine 2014, 10:9 http://www.head-face-med.com/content/10/1/9 HEAD & FACE MEDICINE CASE REPORT Open Access New treatment option for an incomplete vertical root fracture–a preliminary case report Paul Henryk Hadrossek and Till Dammaschke* Abstract Instead of extraction this case report presents an alternative treatment option for a maxillary incisor with a vertical root fracture (VRF) causing pain in a 78-year-old patient. After retreatment of the existing root canal filling the tooth was stabilized with a dentine adhesive and a composite restoration. Then the tooth was extracted, the VRF gap enlarged with a small diamond bur and the existing retrograde root canal filling removed. The enlarged fracture line and the retrograde preparation were filled with a calcium-silicate-cement (Biodentine). Afterwards the tooth was replanted and a titanium trauma splint was applied for 12d. A 24 months clinical and radiological follow-up showed an asymptomatic tooth, reduction of the periodontal probing depths from 7 mm prior to treatment to 3 mm and gingival reattachment in the area of the fracture with no sign of ankylosis. Hence, the treatment of VRF with Biodentine seems to be a possible and promising option. Keywords: Biodentine, Calcium silicate cement, MTA, Treatment, Vertical root fracture Background attempt to preserve teeth with VRF by using MTA was Vertical root fractures (VRF) are fractures of enamel and rejected [4]. Hence, until today, no valid treatment op- dentine along the long axis of the tooth towards the apex tion to preserve teeth with VRF can be recommended. -

ADA Statement on Dental Patient Rights and Responsibilities
ADA Statement on Dental Patient Rights and Responsibilities Background: The ADA Council on Ethics, Bylaws and Judicial Affairs (CEBJA) has developed the following template Dental Patient Rights and Responsibilities Statement (DPRR Statement) as a guide and as an aid to be used by constituent and component societies and practitioners in creating their own dental patients rights and responsibilities statements. In the DPRR Statement that follows, the term “rights” is used not in a legal sense, but merely to convey an indication that a patient should have an expectation of experiencing treatment in accordance with the enumerated “rights.” Several other dental and medical related organizations publish patient rights statements; indeed, CEBJA reviewed those statements during the development of the DPRR Statement, as well as Standard 5-3 of the ADA Commission on Dental Accreditation (CODA) Standards for Predoctoral Dental Education Programs, which also refers to a statement of patients’ rights. The DPRR Statement grew out of a collaborative ethics summit conducted in March 2006 by the American College of Dentists (ACD) and the American Dental Association (ADA) on the topic of commercialism in dentistry. Members of CEBJA were invited to attend along with representatives from ADA and ACD leadership, the ADA Council on Dental Education and Licensure, the recognized specialty groups, the National Dental Association, the U.S. Department of Veterans Affairs, the American Dental Education Association, dental school deans and faculty, ethicists, dental editors and leading representatives from the insurance, practice management and dental product manufacturers industry. The summit attendees noted that patients have become more assertive in seeking elective procedures and that the dental profession seeks to be mindful of protecting patient autonomy while balancing the importance of overall dental health and lifelong consequences. -

Dental Implants Placement of Dental Implants Is a Procedure, Not an American Dental Association (ADA) Recognized Dental Specialty
Dental Implants Placement of dental implants is a procedure, not an American Dental Association (ADA) recognized Dental Specialty. Dental implants like all dental procedures require dental education and training. Implant therapy is a prosthodontic procedure with radiographic and surgical components. Using a dental implant to replace missing teeth is dictated by individual patient needs as determined by their dentist. An implant is a device approved and regulated by the FDA, which can provide support for a single missing tooth, multiple missing teeth, or all teeth in the mouth. The prosthodontic and the surgical part of implant care can each range from straightforward to complex. A General Dentist who is trained to place and restore implants may be the appropriate practitioner to provide care for dental implant procedures. This will vary depending on an individual clinician’s amount of training and experience. However, the General Dentist should know when care should be referred to a specialist (a Prosthodontist, a Periodontist or an Oral and Maxillofacial Surgeon). Practitioners should not try to provide care beyond their level of competence. Orthodontists may place and use implants to enable enhanced tooth movement. Some Endodontists may place an implant when a tooth can’t be successfully treated using endodontic therapy. Maxillofacial Prosthodontists may place special implants or refer for placement when facial tissues are missing and implants are needed to retain a prosthesis. General Dentists are experienced in restorative procedures, and many have been trained and know requirements for the dental implant restorations they provide. However, if a patient’s implant surgical procedure is beyond the usual practice of a dentist, this part of the care should be referred to another dentist that is competent in placement of implants. -

Apicoectomy Treatment
INFORMED CONSENT DISCUSSION FOR APICOECTOMY TREATMENT Patient Name: Date: DIAGNOSIS: Patient’s initials required Twisted, curved, accessory or blocked canals may prevent removal of all inflamed or infected pulp/nerve during root canal treatment. Since leaving any pulp/nerve in the root canal may cause your symptoms to continue or worsen, this might require an additional procedure called an apicoectomy. Through a small opening cut in the gums and surrounding bone, any infected tissue is removed and the root canal is sealed, which is referred to as a retrofilling procedure. An apicoectomy may also be required if your symptoms continue after root canal therapy and the tooth does not heal. Benefits of Apicoectomy, Not Limited to the Following: Apicoectomy treatment is intended to help you keep your tooth, allowing you to maintain your natural bite and the healthy functioning of your jaw. This treatment has been recommended to relieve the symptoms of the diagnosis described above. Risks of Apicoectomy, Not Limited to the Following: I understand that following treatment I may experience bleeding, pain, swelling and discomfort for several days, which may be treated with pain medication. It is possible that infection may accompany treatment and must be treated with antibiotics. I will immediately contact the office if my condition worsens or if I experience fever, chills, sweats or numbness. I understand that I may receive a local anesthetic and/or other medication. In rare instances patients have a reaction to the anesthetic, which may require emergency medical attention, or find that it reduces their ability to control swallowing. This increases the chance of swallowing foreign objects during treatment. -
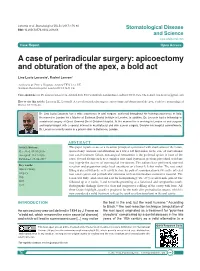
A Case of Periradicular Surgery: Apicoectomy and Obturation of the Apex, a Bold Act
Locurcio et al. Stomatological Dis Sci 2017;1:76-80 DOI: 10.20517/2573-0002.2016.08 Stomatological Disease and Science www.sdsjournal.com Case Report Open Access A case of periradicular surgery: apicoectomy and obturation of the apex, a bold act Lino Lucio Locurcio1, Rachel Leeson2 1Ashford & St. Peter‘s Hospitals, Ashford TW15 3AA, UK. 2Eastman Dental Hospital, London WC1X 8LD, UK. Correspondence to: Dr. Lino Lucio Locurcio, Ashford & St. Peter’s Hospitals, London Road, Ashford TW15 3AA, UK. E-mail: [email protected] How to cite this article: Locurcio LL, Leeson R. A case of periradicular surgery: apicoectomy and obturation of the apex, a bold act. Stomatological Dis Sci 2017;1:76-80. Dr. Lino Lucio Locurcio has a wide experience in oral surgery, achieved throughout his training experience in Italy. He moved to London for a Master at Eastman Dental Institute in London. In addition, Dr. Locurcio had a fellowship in craniofacial surgery at Great Ormond Street Children Hospital. At the moment he is working in London as oral surgeon and implantologist with a special interest in maxillofacial and skin cancer surgery. Besides his hospital commitments, Dr. Locurcio currently works in a private clinic in Battersea, London. ABSTRACT Article history: This paper reports a case of a recurrent periapical cyst treated with enucleation of the lesion, Received: 08-10-2016 apicoectomy, and root end obturation on a lower left first molar. In the case of conventional Accepted: 21-12-2016 root canal treatment failure, non-surgical retreatment is the preferred option in most of the Published: 29-06-2017 cases. -

Lower Lip Numbness Due to Peri-Radicular Dental Infection
Lower Lip Numbness Due to Peri~Radicular Dental Infection WC Ngeow, FFDRCS, Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, Universiti Kebangsaan Malaysia (UKM), Jalan Raja Muda Abdul Aziz, 50300 Kuala Lumpur lip numbness. She complained of a toothache on her lower left first premolar and had seen her dentist who Loss of sensation in the lower lip is a common symptom. performed emergency root canal treatment. Following Frequently, it can be ascribed to surgical procedures that, she felt numbness of her lower lip. carried our in the region of the inferior alveolar nerve or its mental branch. In addition, trauma, haematoma or Clinical examination revealed a mandibular left first acute infections may cause the problem 1. Localised and premolar with a dressing. The tooth was slightly tender metastatic neoplasms, systemic disorders and some to percussion. Other neighbouring teeth reacted nor drugs are the other causes responsible 1. mally to percussion. No swelling could be seen at the buccal sulcus of the premolar. Her lower left lip looked Although benign in appearance, mental nerve normal, but she could not distinguish sharp pain when neuropathy is frequently of significance. Most often it pricked with a dental probe. is associated with malignant diseases. Breast cancer is the most common cause '. Other common causes Radiographic examination revealed a radiolucency at the include malignant blood diseases 2 which may include peri-radicular area of the mandibular left first premolar Burkitt's lymphoma, Hodgkins lymphoma and and another radiolucency just slightly away from the multiple myeloma. peri-radicular area of the mandibular left canine tooth. -

TOOTH SUPPORTED CROWN a Tooth Supported Crown Is a Dental Restoration That Covers up Or Caps a Tooth
TOOTH SUPPORTED CROWN A tooth supported crown is a dental restoration that covers up or caps a tooth. It is cemented into place and cannot be taken out. Frequently Asked Questions 1. What materials are in a Tooth Supported Crown? Crowns are made of three types of materials: • Porcelain - most like a natural tooth in color • Gold Alloy - strongest and most conservative in its preparation • Porcelain fused to an inner core of gold alloy (Porcelain Fused to Metal or “PFM”) - combines strength and aesthetics 2. What are the benefits of having a Tooth Supported Crown? Crowns restore a tooth to its natural size, shape and—if using porce lain—color. They improve the strength, function and appearance of a broken down tooth that may otherwise be lost. They may also be designed to decrease the risk of root decay. 3. What are the risks of having a Tooth Supported Crown? In having a crown, some inherent risks exist both to the tooth and to the crown Porcelain crowns build back smile itself. The risks to the tooth are: • Preparation for a crown weakens tooth structure and permanently alters the tooth underneath the crown • Preparing for and placing a crown can irritate the tooth and cause “post- operative” sensitivity, which may last up to 3 months • The tooth underneath the crown may need a root canal treatment about 6% of the time during the lifetime of the tooth • If the cement seal at the edge of the crown is lost, decay may form at the juncture of the crown and tooth The risks to the crown are: • Porcelain may chip and metal may wear over time • If the tooth needs a root canal treatment after the crown is permanently cemented, the procedure may fracture the crown and the crown may need to be replaced.