Combat Wounded Veteran Mountaineering Challenge – Denali
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Bozeman Climbers Tackle Gan
BOZEMAN CLIMBERS TACKLE GANNETT PEAK TO BENEFIT U... http://chronicleoutdoors.com/2010/03/18/bozeman-climbers-to-tackle-w... Chronicle Outdoors Dedicated to outdoor adventure in Southwest Montana Home Photo Gallery Where Am I Contest About Contact .: This week's poll :. Fifteen years ago wolves were released into Yellowstone Park. They have since established range outside the park and been embroiled in controversy. Do you think their presence is appropriate? Yes, wolves are a native predator that help maintain a natural balance in the Greater Yellowstone Ecosystem. No way, wolves have depleted elk herds, killed sheep and cattle and caused conflict. They create more problems than they solve. Vote View Results .: Gallatin ational Forest Avalanche Report :. GNFAC Avalanche Advisory for Sun Mar 21, 2010 Good Morning. This is Eric Knoff with the Gallatin National Forest Avalanche Advisory issued on Sunday, March 21, at 7:30 a.m. Bountiful Table, in cooperation with the Friends of the Avalanche Center, sponsors today's advisory. This advisory does not apply to operating ski areas. Mountain Weather: A ridge of high pressure has stalled over southwest M […] .: Latest news from Montana Fish, Wildlife & Parks :. Wild Bison’s Future In Montana What is the future for wild bison in Montana? […] Three Bear Aware Meetings Planned For Front State wildlife officials are planning three community meetings in April to remind north central Montana residents to be bear aware. The meetings will begin at 7 p.m. and take place April 12, Simms high school; April 13, Marias River Electric Coop in Shelby; and April 14, Wolf Creek School. -
Alaska Range
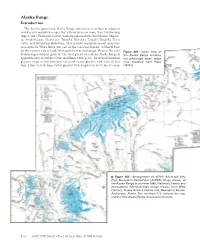
Alaska Range Introduction The heavily glacierized Alaska Range consists of a number of adjacent and discrete mountain ranges that extend in an arc more than 750 km long (figs. 1, 381). From east to west, named ranges include the Nutzotin, Mentas- ta, Amphitheater, Clearwater, Tokosha, Kichatna, Teocalli, Tordrillo, Terra Cotta, and Revelation Mountains. This arcuate mountain massif spans the area from the White River, just east of the Canadian Border, to Merrill Pass on the western side of Cook Inlet southwest of Anchorage. Many of the indi- Figure 381.—Index map of vidual ranges support glaciers. The total glacier area of the Alaska Range is the Alaska Range showing 2 approximately 13,900 km (Post and Meier, 1980, p. 45). Its several thousand the glacierized areas. Index glaciers range in size from tiny unnamed cirque glaciers with areas of less map modified from Field than 1 km2 to very large valley glaciers with lengths up to 76 km (Denton (1975a). Figure 382.—Enlargement of NOAA Advanced Very High Resolution Radiometer (AVHRR) image mosaic of the Alaska Range in summer 1995. National Oceanic and Atmospheric Administration image mosaic from Mike Fleming, Alaska Science Center, U.S. Geological Survey, Anchorage, Alaska. The numbers 1–5 indicate the seg- ments of the Alaska Range discussed in the text. K406 SATELLITE IMAGE ATLAS OF GLACIERS OF THE WORLD and Field, 1975a, p. 575) and areas of greater than 500 km2. Alaska Range glaciers extend in elevation from above 6,000 m, near the summit of Mount McKinley, to slightly more than 100 m above sea level at Capps and Triumvi- rate Glaciers in the southwestern part of the range. -
Beyond the Exit
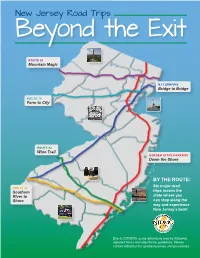
New Jersey Road Trips Beyond the Exit ROUTE 80 Mountain Magic NJ TURNPIKE Bridge to Bridge ROUTE 78 Farm to City ROUTE 42 Wine Trail GARDEN STATE PARKWAY Down the Shore BY THE ROUTE: Six major road ROUTE 40 Southern trips across the River to state where you Shore can stop along the way and experience New Jersey’s best! Due to COVID19, some attractions may be following adjusted hours and attendance guidelines. Please contact attraction for updated policies and procedures. NJ TURNPIKE – Bridge to Bridge 1 PALISADES 8 GROUNDS 9 SIX FLAGS CLIFFS FOR SCULPTURE GREAT ADVENTURE 5 6 1 2 4 3 2 7 10 ADVENTURE NYC SKYLINE PRINCETON AQUARIUM 7 8 9 3 LIBERTY STATE 6 MEADOWLANDS 11 BATTLESHIP PARK/STATUE SPORTS COMPLEX NEW JERSEY 10 OF LIBERTY 11 4 LIBERTY 5 AMERICAN SCIENCE CENTER DREAM 1 PALISADES CLIFFS - The Palisades are among the most dramatic 7 PRINCETON - Princeton is a town in New Jersey, known for the Ivy geologic features in the vicinity of New York City, forming a canyon of the League Princeton University. The campus includes the Collegiate Hudson north of the George Washington Bridge, as well as providing a University Chapel and the broad collection of the Princeton University vista of the Manhattan skyline. They sit in the Newark Basin, a rift basin Art Museum. Other notable sites of the town are the Morven Museum located mostly in New Jersey. & Garden, an 18th-century mansion with period furnishings; Princeton Battlefield State Park, a Revolutionary War site; and the colonial Clarke NYC SKYLINE – Hudson County, NJ offers restaurants and hotels along 2 House Museum which exhibits historic weapons the Hudson River where visitors can view the iconic NYC Skyline – from rooftop dining to walk/ biking promenades. -
Guide to the Battles of Trenton and Princeton
Hidden Trenton Guide to the Battles of Trenton and Princeton Nine Days that Changed the World December 26, 1776 to January 3, 1777 A self-guided tour of the places and events that shaped the battles and changed the history of America Go to http://HiddenTrenton.com/BattleTour for links to online resources Updated 2017 Copyright © 2011, 2017 all rights reserved. The pdf file of this document may be distributed for non- commercial purposes over the Internet in its original, complete, and unaltered form. Schools and other non-profit educational institutions may print and redistribute sections of this document for classroom use without royalty. All of the illustrations in this document are either original creations, or believed by the author to be in the public domain. If you believe that you are the copyright holder of any image in this document, please con- tact the author via email at [email protected]. Forward I grew up in NJ, and the state’s 1964 Tricentennial cel- Recently, John Hatch, my friend and business partner, ebration made a powerful impression on me as a curious organized a “Tour of the Battle of Trenton” as a silent 4th grader. Leutez’ heroic portrait of Washington Cross- auction item for Trenton’s Passage Theatre. He used ing the Delaware was one of the iconic images of that Fischer’s book to research many of the stops, augmenting celebration. My only memory of a class trip to the park his own deep expertise concerning many of the places a year or two later, is peering up at the mural of Wash- they visited as one of the state’s top restoration architects. -

High Point, New Jersey – ‘09
High Point, New Jersey – ‘09 High Point, New Jersey is located a few miles from the NJ-NY-PA tri-point. The summit is 1803 feet above sea level. It is a drive-up located inside of High Point State Park. At the top of the 220-foot structure, observers have a breathtaking view of the ridges of the Pocono Mountains toward the west, the Catskill Mountains to the north and the Wallkill River Valley in the southeast. Convention Headquarters --- Best Western Inn at Hunt’s Landing The convention headquarters will be located in Matamoras, Pennsylvania -- a ten minute drive from the highpoint, directly across the Delaware River. The Best Western can accommodate 600 people for a banquet and the patio can host the Friday night reception with a beautiful view of the highpoint. In addition to the 108 rooms at the Best Western Inn, the following accommodations are located within 10 miles of the highpoint. Hotel Accommodations Camping Comfort Inn 104 rooms High Point State Park 50 tent sites Red Carpet Inn 26 rooms River Beach (on the Delaware River) 160 multi-use sites Hotel Fauchere 15 rooms Tri-State RV Park 33 multi-use sites Scottish Inn 21 rooms Other Activities and Points of Interest * Canoeing and rafting in the Delaware River * Rock climbing in The Gunks * Horseback riding * NYC day trips by commuter rail * Bushkill Falls * Delaware Water Gap Nat. Rec. area * NJ-NY-PA tri-state marker * Fishing * Appalachian Trail hiking * Mountain Creek Waterpark Nearest Highpoints (Driving Distance) Mount Frissell 115 miles Ebright Azimuth 150 miles Mount Greylock 170 miles Jerimoth Hill 190 miles Mount Marcy 270 miles Mount Mansfield 320 miles . -

Breasts on the West Buttress Climbing the Great One for a Great Cause
Breasts on the West Buttress Climbing the Great One for a great cause Nancy Calhoun, Sheldon Kerr, Libby Bushell A Ritt Kellogg Memorial Fund Proposal Calhoun, Kerr, Bushell; BOTWB 24 Table of Contents Mission Statement and Goals 3 Libby’s Application, med. form, agreement 4-8 Libby’s Resume 9-10 Nancy’s Application, med. form, agreement 11-15 Nancy’s Resume 16-17 Sheldon’s Application, med. form, agreement 18-23 Sheldon’s Resume 24-25 Ritt Kellogg Fund Agreement 26 WFR Card copies 27 Travel Itinerary 28 Climbing Itinerary 29-34 Risk Management 35-36 Minimum Impact techniques 37 Gear List 38-40 First Aid Contents 41 Food List 42-43 Maps 44 Final Budget 45 Appendix 46-47 Calhoun, Kerr, Bushell; BOTWB 24 Breasts on the West Buttress: Mission Statement It may have started with the simple desire to climb North America’s tallest peak, but with a craving to save the world a more pressing concern on the minds of three Colorado College women (a Vermonter, an NC southern gal, and a life-long Alaskan), we realized that climbing Denali could and should be only a mere stepping stone to the much greater task at hand. Thus, we’ve teamed up with the American Breast Cancer Foundation, an organization that is doing their part to save our world, one breast at a time, in order to do our part, in hopes of becoming role models and encouraging the rest of the world to do their part too. So here’s our plan: We are going to climb Denali (Mount McKinley) via the West Buttress route in June of 2006. -
Fostertext Pdf, Rev
HISTORY AND DYNAMICS OF A RIDGETOP PITCH PINE COMMUNITY MOUNT EVERETT, MASSACHUSETTS GLENN MOTZKIN DAVID A. ORWIG and DAVID R. FOSTER HISTORY AND DYNAMICS OF A RIDGETOP PITCH PINE COMMUNITY MOUNT EVERETT, MASSACHUSETTS GLENN MOTZKIN DAVID A. ORWIG and DAVID R. FOSTER 2002 HARVARD FOREST HARVARD UNIVERSITY PETERSHAM, MASSACHUSETTS HARVARD FOREST PAPER NO. 25 Copyright © 2002 by the President and Fellows of Harvard College All rights reserved. Printed in the United States of America Front cover: Southern slope of Mt. Everett viewed from Mt. Race. Back cover: Contorted crown of red oak (Quercus rubra) with scars and broken branches from winter storms. SUMMARY 1. The summit of Mt. Everett in the Town of Mount early historical periods. Because the site has long Washington, Massachusetts supports a highly been a destination for local residents for recre- unusual dwarf pitch pine-oak community; similar ation and for berry gathering, it is possible that vegetation is found on only a few sites throughout fire or cutting were used historically to improve the northeastern United States. Age-structure fruit production or expand views, but we found analyses and historical records of human and no documentation of such activities. natural disturbance were used to investigate the 5. During the twentieth century, under management long-term history and dynamics of the summit by the Commonwealth of Massachusetts, access vegetation. trails and two fire towers were constructed on the 2. Throughout the historical period, the summit of summit, one of which still stands although it is in Mt. Everett has been dominated by dwarf pitch poor repair and has rarely, if ever, been staffed. -
2018 Annual Mountaineering Summary
2018 Annual Mountaineering Summary NPS Photo (M. Coady) 2018 Statistical Year in Review Each season's !!!~~D.~~.iD.~.~- ~!~~ . !:.~':!.!~ . ~!~!!~!!~~ · including total attempts and total summits for Denali and Foraker, are now compiled into one spreadsheet spanning from 1979 to 2018. The P.~ .':1.~.1 ! ..l?.!~P.~!~~~~ blog can provide a more detailed perspective of the 2018 season, including daily statistics, weather, conditions reports, photos, and random climbing news. Thank you to the 31 !!!~~!:.'~.~.i.':1.~.~-~!~~t~.<?.1.':l. ~!~~~~ ~! .':1::~~~~! (VIP's) who teamed up with Denali rangers to staff the mountain camps in 2018. Read about the efforts of the 2018 recipients of the M.i.:;. 1.~~:~~~- ~~~~ - g-~D.~.l.i.. ~~~ Award. Quick Facts - Denali • Climbers from the USA: 694 (63% of total) Climbers hailed from 42 of the 50 states in 2018. Colorado was the most heavily represented with 114 climbers. Alaska followed close behind with 111 climbers. There were 87 climbers from Washington and 72 from California. • International climbers: 420 (37% of total) 51 foreign nations were represented on Denali in 2018. Of the international climbers, Poland generated the highest number of climbers with 47. Canada was next with 42. Australia was suprisingly well-represented on Denali this season, with 28 climbers. China and Japan each had 24 climbers on Denali. We had one climber each from Andorra, Kazakhstan, and Qatar. • Average trip length The average trip length on Denali was 17 days; independent teams averaged a day less (16 days), while guided teams averaged a day more (18 days). The average length of a Muldrow Glacier climb was 27 days. -

Climbing America's
batical leave in Scandinavia, I finally reached the 5895m summit of Africa’s high- est mountain. In 1986, the year after I climbed Kilimanjaro, Dick Bass, Frank Wells, and Rick Ridgeway published Seven Summits, an account of Bass and Wells’ attempt to climb the highest peak on each of the world’s seven continents. I bought their book and devoured it. Inspired by it, I devised my own climbing goal—to climb at least ‘Three-and-a-Half Summits’: namely, at least three of the six highest of the Seven Summits plus Australia’s Mt Kosciuszko, which is a mere 2228m above sea level (i.e., less than half the height of Antarctica’s Vinson Massif, the sixth-lowest of the Seven Summits), and Kosciuszko can therefore, as a Kiwi I quipped, really only be regarded as a half-summit. I made reasonably quick progress towards achieving my goal. In August 1994, I climbed Russia’s Mt Elbrus, 5642m, the highest mountain in Europe. In December the same year, I summited 6962m-high Cerro Aconcagua in Argentina, the highest mountain in South America (which I like to tell people is ‘the highest mountain in the world outside Asia,’ and then hope their geography is so weak that they don’t realise how huge an exclusion clause those two words, ‘outside Asia’, are). I then decided to have a crack at climbing Denali, and on 6 July 1997 stood proudly on the 6194m-high summit of North America’s high- est peak and held up a t-shirt from Victoria University (which is where I taught political science for many years). -

Radio Control Tower, Southwest Buttress, It's Included
AAC Publications Radio Control Tower, southwest buttress, It’s Included Alaska, Central Alaska Range In June, Alan Rousseau and I flew into the Southeast Fork of the Kahiltna Glacier between guiding trips on Denali to see what we could get done. With huge amounts of snowfall and warming temps, we ruled out all routes with snow above them. We decided to get a bit creative. This led us up a new route on the very rocky southwest buttress of Radio Control Tower (8,670’), which is located just east of Kahiltna Base Camp. The route was an interesting outing with some harder pitches and lots of exploration required to reach the top of the buttress: It’s Included (1,000’, 5.10+ AI3 M7). – Mark Pugliese Editor’s note: Previously unreported, in May 2013, Alan Rousseau and Aaron Kurland made the first recorded ascent of the west face of Radio Control Tower, climbing a prominent gully and snow-ramp system just left of the southwest buttress. They called the seven-pitch climb Spindrift Couloir (1,000’, AI3 M5). Given the proximity of Radio Control Tower to the Kahiltna Base Camp it’s possible other routes have gone unreported. Images The southwest buttress of Radio Control Tower showing the new route It’s Included (1,000’, 5.10+ AI3 M7). The west face of Radio Control Tower showing the previously unreported route Spindrift Couloir (1,000’, AI3 M5). The new route It’s Included climbs the buttress just to the right. Article Details Author Mark Pugliese Publication AAJ Volume 57 Issue 89 Page 0 Copyright Date 2015 Article Type Climbs and expeditions. -

Position Outreach Announcement
Outreach - GS-0462-10 Supervisory Forestry Technician (Airbase/Short-haul Base Manager) Bridger-Teton National Forest (BTNF)/Grand Teton National Park (GTNP) In Jackson, Wyoming The Announcement Numbers for this position will be forthcoming in a subsequent announcement. Duty Location for this position will be Jackson, Wyoming Government housing may be available. The North Zone of the Bridger-Teton National Forest is planning to fill an Airbase/Short- haul Base Manager position in the near future. Outreach responses are expected by October 23, 2015 and the application deadline will be November 01, 2015. The referral lists will be requested on November 01, 2015. This is a permanent position, GS-0462-10, the position will be based at the Jackson Airport where the Teton Helibase is located; tour of duty will be PFT and employment will be through the Bridger-Teton Forest. Anyone interested in further information should e-mail Steve Markason, North Zone FMO, at [email protected], 307-739-5431. To apply and for more information go to: https://www.usajobs.gov THE POSITION The program is interagency in its composition and mission. In addition to suppression, the program provides search and rescue, fire use, aerial ignition, and project services directly to the BTNF and GTNP. Search and rescue missions also occur in support of area county Sheriffs Offices. Personnel and aircraft are regularly dispatched off-area when not required by local staffing requirements. The Teton Helitack program successfully implemented the Forest Service Short Haul program in 2015. The position serves as the Airbase/Shorthaul Manager supervising with a GS-09 Helitack Supervisor for a 20 person, two helicopter program located at the Teton Interagency Helibase. -

Naturalist Pocket Reference
Table of Contents Naturalist Phone Numbers 1 Park info 5 Pocket GRTE Statistics 6 Reference Timeline 8 Name Origins 10 Mountains 12 Things to Do 19 Hiking Trails 20 Historic Areas 23 Wildlife Viewing 24 Visitor Centers 27 Driving Times 28 Natural History 31 Wildlife Statistics 32 Geology 36 Grand Teton Trees & Flowers 41 National Park Bears 45 revised 12/12 AM Weather, Wind Scale, Metric 46 Phone Numbers Other Emergency Avalanche Forecast 733-2664 Bridger-Teton Nat. Forest 739-5500 Dispatch 739-3301 Caribou-Targhee NF (208) 524-7500 Out of Park 911 Grand Targhee Resort 353-2300 Jackson Chamber of Comm. 733-3316 Recorded Information Jackson Fish Hatchery 733-2510 JH Airport 733-7682 Weather 739-3611 JH Mountain Resort 733-2292 Park Road Conditions 739-3682 Information Line 733-2291 Wyoming Roads 1-888-996-7623 National Elk Refuge 733-9212 511 Post Office – Jackson 733-3650 Park Road Construction 739-3614 Post Office – Moose 733-3336 Backcountry 739-3602 Post Office – Moran 543-2527 Campgrounds 739-3603 Snow King Resort 733-5200 Climbing 739-3604 St. John’s Hospital 733-3636 Elk Reduction 739-3681 Teton Co. Sheriff 733-2331 Information Packets 739-3600 Teton Science Schools 733-4765 Wyoming Game and Fish 733-2321 YELL Visitor Info. (307) 344-7381 Wyoming Highway Patrol 733-3869 YELL Roads (307) 344-2117 WYDOT Road Report 1-888-442-9090 YELL Fill Times (307) 344-2114 YELL Visitor Services 344-2107 YELL South Gate 543-2559 1 3 2 Concessions AMK Ranch 543-2463 Campgrounds - Colter Bay, Gros Ventre, Jenny Lake 543-2811 Campgrounds - Lizard Creek, Signal Mtn.