Journal of Medical Sciences
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Faisalabad Chamber of Commerce & Indusrty
THE FAISALABAD CHAMBER OF COMMERCE & INDUSRTY FINAL ASSOCIATE VOTERS FOR THE YEAR 2016-17 Page 1 of 142 1. 2104577-3610 7. 2106048-4897 13. 2103964-3062 3-A TEXTILES A & H CORPORATION A.A ENTERPRISES P-1 SECOND FLOOR SARA TOWER CENTRE OFFICE # 4, 2ND FLOOR ABUTURAB P-27 GALI NO 7 MOHALLAH QASIM MAIN SUSAN ROAD MADINA BUILDING, AMINPUR BAZAR FAISALABAD ABAD,JHANG ROAD, FAISALABAD TOWN,FAISALABAD NTN : 2681221-5 NTN : 2259549-0 NTN : 1324438-8 STN : STN : STN : 08-90-9999-882-82 TEL : 041-8559844,5506962 TEL : 041-2551678 TEL : 041-8723388 CELL: 0300-9656930 CELL: 0300-9652354,0321-7220920 CELL: 0300-8668801 EMAIL :[email protected], rana_248@hotmai EMAIL :[email protected] EMAIL :[email protected] REP : RANA MUNAWAR HUSSAIN REP : HAMID BASHIR REP : AIJAZ AHMAD NIC : 33100-0147581-1 NIC : 33100-4747059-7 NIC : 33100-5628937-9 2. 2106191-5024 8. 2300939-682 14. 2102967-2222 381 INTERNATIONAL A & H ENTERPRISES A.A ENTERPRISES 1ST FLOOR UNION TRADER OPP. SHELL CHEEMA MARKET RAILWAY ROAD SHOP NO 4 AL HAKEEM CENTRE CHTTREE PUMP NEAR GHOUSHALA DIJKOT ROAD FAISALABAD WALA CHOWK JINNAH COLONY FAISALABAD NTN : 2164711-9 FAISALABAD NTN : 2736536-7 STN : 08-01-5900-008-46 NTN : 2316510-3 STN : TEL : 041-2643933 STN : TEL : 041-2626381 CELL: 0300-8666818 TEL : 041-8739180 CELL: 0344-4444381 EMAIL :[email protected] CELL: 0300-8656607 EMAIL :[email protected] REP : MUHAMMAD ASIM EMAIL :[email protected] REP : JAWAD ALI NIC : 33100-1808192-7 REP : ATIF IDREES NIC : 33100-6169762-5 NIC : 33104-2111449-9 3. 2105589-4504 9. -

SARHAD CHAMMBER of COMMERCE and INDUSTRY Chamber House, G.T.Road, Peshawar
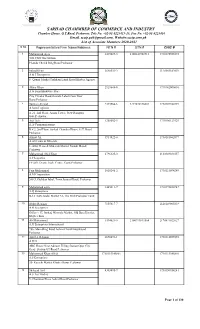
SARHAD CHAMMBER OF COMMERCE AND INDUSTRY Chamber House, G.T.Road, Peshawar. Tele No. +92-91-9225413-15, Fax No. +92-91-9225416 Emai.:[email protected], Websit:sccip.com.pk List of Associate Members 2019-2020 S No Representative/Firm Name/Address NTN # STN # CNIC # 1 Mohammad Ayaz 3419029-5 2100341902916 1730175925573 3GS CNG Gas Station Phandu Chowk Ring Road Peshawar 2 Irshad Khan 3648532-2 2120303182039 A & J Enterprises 8- Qaumi Market Torkham Landi Kotal Khyber Agency 3 Akbar Khan 2929648-0 17301620000601 A & Sons Hardware Store City Circular Road,Outside Lahori Gate,Near Bano,Peshawar 4 Asif Aziz 1288602-5 1730106123929 A.A Communications R # 2, 2nd Floor, Sarhad Chamber House, G.T. Road, Peshawar. 5 Azmat Ali 3914822-0 1730181862877 A.Ali Gems & Minerals 1- Swat Gems & Minerals Market Namak Mandi Peshawar 6 Javaid Khan Bangash 2494400-9 1430119590389 A.K Traders Zain Market Chowk Yadgar Peshawar 7 Faiz Muhammad 1018246-2 1730115094249 A.M.Corporation 588/3, Gulshan Iqbal, Town,Jamrud Road, Peshawar 8 Mohammad asim 1445611-7 1730192426947 A.Q Enterprises B-12 Satta Gadai Market 32- The Mall Peshawar Cantt 9 Abdur Rehman 7155817-7 2120149805839 A.R Enterprises 5-2nd Floor Abdul Market Namak Mandi Peshawar 10 Ali Muhammad 3394021-5 2100999811564 2170891022627 A.R Enterprises International 786- Main Ring Road Achini Chowk Hayatabad Peshawar 11 Aziz Ur Rehman 2670691-1 1730114035959 A.R.G ARG House Near Admore Filling Station Opp: City Grade Station GT Road Peshawar 12 Shehzad Arif 4303495-7 1730150954241 A.S Tea Traders 9- Chairman -

Name of Applicant in Membership Drive Ph-I (Journalist) Date of SNO Cat
Name of Applicant in Membership Drive Ph-I (Journalist) Date of SNO Cat. Name of Applicant DOB Mobile Number CNIC Rank with Post Parent Department Present Department Submission 1 1 28-May-15 HAFIZ MUHAMMAD TAHIR 24-Jun-64 3009558367 6110118416603 CHIEF EDITOR JR JR 2 1 28-May-15 HAFIZ MUHAMMAD IQBAL 6-Nov-65 3335101543 3740594408475 EDITOR JR JR SYED TABASSUM ABBAS INTERNATIONAL MEDIA 3 1 3-Jun-15 6-Oct-77 3335103856 3720178576793 EDITOR SHAH INSIGHT (IMI) NEWS AGENCY 4 1 4-Jun-15 MUMTAZ HUSSAIN 18-Jul-72 3335182812 3740581049865 EDITOR DAILY DIN RAWALPINDI INTER FAITH NEWS INTER FAITH NEWS 5 1 9-Jun-15 BASHIR AHMED KHAN 1-Apr-58 3036669407 3630227401989 EDITOR NETWORKS NETWORKS ISLAMABAD ROZE NEWS ROZE NEWS TELEVISION 6 1 10-Jun-15 WAHEED HUSSAIN 4-Mar-68 3008505467 3740560321723 SR. ANCHORPERSON TELEVISION CHANNEL CHANNEL 7 1 12-Jun-15 ATIF SAEED 20-Oct-69 3322224230 3520158241459 ANSAR MEHMOOD DIPLOMATIC NEWS AGENCY 8 1 16-Jun-15 3-Aug-69 3335203232 6110120881037 EDITOR BHATTI (DNA) MONTHLY CENTRELINE 9 1 23-Jun-15 AQEEL AHMAD TAREEN 10-Oct-74 3008506474 3740651885337 ROSDENT EDITOR EDITORIAL DAILY WATEENN 10 1 24-Jun-15 NIAZ HUSSAIN HAIDERY 14-Jun-72 3448484849 3740513837495 EDITOR ISLAMABAD GHULAM MOHIUDDIN DAILY KASHMIR POST DAILY KASHMIR POST 11 1 30-Jun-15 20-Nov-69 3335108940 3740503819943 EDITOR DAR INTERNATIONAL INTERNATIONAL DAILY KASHMIR POST DAILY KASHMIR POST 12 1 30-Jun-15 IMTIAZ AHMED 16-Nov-73 3005205400 6110188845291 CHIEF EDITOR INTERNATIONAL INTERNATIONAL DAILY AZADI DAILY AZADI 13 1 2-Jul-15 MUMTAZ AHMAD SADIQ 14-Jan-63 -

1002573 Waqas Ahmed 1,320,157 H No 359 St No 14 F 10 2 Islamabad Islamabad 517738 Chaudhry Kamran Waheed 591,813 H No 164 Shah
PUBLIC NOTICE AUCTION OF GOLD ORNAMENTS AND VALUABLES Finance facilities were extended by JS Bank Limited to its customers mentioned below against the security of deposit and pledge of Gold ornaments/valuables. The customers have neglected and failed to repay the finances extended to them by JS Bank Limited along with the mark-up thereon. The current outstanding liability of such customers is mentioned below. Notice is hereby given to the under mentioned customers that if payment of the entire outstanding amount of finance along with mark-up is not made by them to JS Bank Limited within 15 days of the publication of this notice, JS Bank Limited shall auction the Gold ornaments/valuables after issuing public notice regarding the date and time of the public auction and the proceeds realized from such auction shall be applied towards the outstanding amount due and payable by the customers to JS Bank Limited. No further public notice shall be issued to call upon the customers to make payment of the outstanding amounts due and payable to JS Bank as mentioned hereunder: Total Outstanding as Customer ID Customer Name Address of 8th March, 2020 1002573 WAQAS AHMED 1,320,157 H NO 359 ST NO 14 F 10 2 ISLAMABAD ISLAMABAD 517738 CHAUDHRY KAMRAN WAHEED 591,813 H NO 164 SHAHJAMAL C OLONY LAHORE LAHORE 200877 MUHAMMAD NAHEED KHAN ABBASI 578,646 BARSAL PO KOHALA TEH AND DISTT MUZAFFERABAD AZAD K ASHMIR AZAD KASHMIR 1008854 NANIK RAM 514,149 VILLAGE JARWAR PSOT OFFICE JARWAR GHOTKI 65110 PAK SITAN GHOTKI 1077154 GHULAM MUSTAFA HAKRO 475,518 STREET NO -
Final Voter List (Associate) 2020-21
SARHAD CHAMMBER OF COMMERCE AND INDUSTRY Chamber House, G.T.Road, Peshawar. Tele No. +92-91-9225413-15, Fax No. +92-91-9225416 Email. [email protected], Website:sccip.com.pk List of Associate Members 2020-2021 S No Representative/Firm Name/Address NTN # STN # CNIC # 1 Mohammad Ayaz 3419029-5 2100341902916 1730175925573 3GS CNG Gas Station Phandu Chowk Ring Road Peshawar 2 Irshad Khan 3648532-2 2120303182039 A & J Enterprises 8- Qaumi Market Torkham Landi Kotal Khyber Agency 3 Akbar Khan 2929648-0 1730162000601 A & Sons Hardware Store City Circular Road,Outside Lahori Gate,Near Bano,Peshawar 4 Tanveer Ahmad 2393366-6 3277876146001 1730107480749 A Sons Logistics A-21, 2nd Floor, Arsala Tower, New Rampura Gate,Peshawar 5 Asif Aziz 1288602-5 1730106123929 A.A Communications R # 2, 2nd Floor, Sarhad Chamber House, G.T. Road, Peshawar. 6 Azmat Ali 3914822-0 1730181862877 A.Ali Gems & Minerals 1- Swat Gems & Minerals Market Namak Mandi Peshawar 7 Muhammad Abid Khan 2796325-0 2120349031057 A.F Logistics FF-269, Deans Trade Centre, Cantt,Peshawar 8 Faiz Muhammad 1018246-2 1730115094249 A.M.Corporation 588/3, Gulshan Iqbal, Town,Jamrud Road, Peshawar 9 Mohammad asim 1445611-7 1730192426947 A.Q Enterprises B-12 Satta Gadai Market 32- The Mall Peshawar Cantt 10 Abdur Rehman 7155817-7 2120149805839 A.R Enterprises Office # 17, Ittehad Minerals Market, Old Bara District, Khyber Bara 11 Ali Muhammad 3394021-5 2100999811564 2170891022627 A.R Enterprises International 786- Main Ring Road Achini Chowk Hayatabad Peshawar 12 Aziz Ur Rehman 2670691-1 1730114035959 -
Inance Facilities Were Extended by JS Bank Limited to Its Customers Mentioned Below Against the Security of Deposit and Pledge of Gold Ornaments/Valuables
PUBLIC NOTICE AUCTION OF GOLD ORNAMENTS AND VALUABLES Finance facilities were extended by JS Bank Limited to its customers mentioned below against the security of deposit and pledge of Gold ornaments/valuables. The customers have neglected and failed to repay the finances extended to them by JS Bank Limited along with the mark-up thereon. The current outstanding liability of such customers is mentioned below. Notice is hereby given to the under mentioned customers that if payment of the entire outstanding amount of finance along with mark-up is not made by them to JS Bank Limited within 15 days of the publication of this notice, JS Bank Limited shall auction the Gold ornaments/valuables after issuing public notice regarding the date and time of the public auction and the proceeds realized from such auction shall be applied towards the outstanding amount due and payable by the customers to JS Bank Limited. No further public notice shall be issued to call upon the customers to make payment of the outstanding amounts due and payable to JS Bank as mentioned hereunder: Total Overdue S.NO Customer ID Customer Name (in Rs.)as of 6 Address January, 2020 1 517738 CHAUDHRY KAMRAN WAHEED 1,372,630 H NO 164 SHAHJAMAL C OLONY LAHORE LAHORE 2 517738 CHAUDHRY KAMRAN WAHEED 1,372,630 H NO 164 SHAHJAMAL C OLONY LAHORE LAHORE 3 517738 CHAUDHRY KAMRAN WAHEED 1,372,630 H NO 164 SHAHJAMAL C OLONY LAHORE LAHORE 4 517738 CHAUDHRY KAMRAN WAHEED 1,372,630 H NO 164 SHAHJAMAL C OLONY LAHORE LAHORE 5 1002573 WAQAS AHMED 1,283,585 H NO 359 ST NO 14 F 10 2 ISLAMABAD -

Table of Contents
Table of Contents Departments Page No Bio Informatics……........................................................... 01 Computer Science………………..…………………..……………………. 04 Environmental Science……………………………………………………. 106 Mathematics…………………..……………………………………………… 109 Software Engineering………...………………………………………….. 111 For further information please contact: Muhammad Rafiq Chaudhary (Principal Librarian) Central Library, International Islamic University, Islamabad T: 9257955, 9019383 (Incampus calling: 2383) E‐mail: [email protected] Bio Informatics MS S.No Title Author Year Call. No 1. Genetic analysis and candidate genes Saiam Zubair 2009 MS prediction in Pakistan families with 576.55491 Retinal Dystrophies SAG 2. Genetic analysis and candidate genes Tahira Noor 2009 MS prediction in Pakistani families with 572.869 hearing impairment TAG 3. Genetic analysis and insilico gene Shagufta kanwal 2009 MS identification and drug designing of 572.88 inherited vitiligo in Pakistan SHG 4. Genetic studies and computational Sumaira Nishat 2009 MS analysis of hereditary limb anomalies and 571.948 muscular dystrophy SUG 5. In silico mutation analysis of LAH2 & Amara Jabeen 2009 MS LAH3 576.5 AMS 6. In silico protein analysis of genes Anjum , Iffat 2009 MS involved in alopecia areata Farzana 572.88 ANI 7. Molecular characterization of mitogen Awaisa Ghazal 2009 MS activated protein kinase kinase 3 (MKK3) 612.62 AWM BS S.No Title Author Year Call No 1. Molecular docking studies and design of Madiha 2010 BS anti hepatitis B Drugs in silico sattar; Mahira 616.3623 Arooj; Muniba MAM Safdar 2. Identification and phylogenetic analysis Aimen Sulaiman 2010 BS of novel species of Bacteria from ; Anam Naz 571.3 Pakistan ecology ; Rabia Farid AII 3. Mol‐Ds molecular dynamics simulator Naila Zaman 2010 BS ; Shifa Tahir 530.41 NAM 4. -

UNESCO Condemns Killing of Journalists Assassinated Journalists in Pakistan
UNESCO Condemns Killing of Journalists Assassinated Journalists in Pakistan Sohail Khan (Pakistani) Reporter for K2 Daily Times Killed on 16 October 2018 in Pakistan UNESCO Statement Abid Hussain (Pakistani) Journalist Killed on 23 August 2018 in Pakistan UNESCO Statement Zeeshan Ashraf Butt (Pakistan) Journalist for the local newspaper Nawa-i-Waqt Killed on 27 March 2018 [UNESCO Statement] Anjum Munir Raja (Pakistan) Sub-editor Killed on 1 March 2018 [UNESCO Statement] [Response from Member State 2018] Haroon Khan (Pakistan) Broadcast journalists Killed on 12 October 2017 [UNESCO Statement] Baksheesh Elahi (Pakistani) Journalist Killed on 11 June 2017 [UNESCO Statement] Taimur Abbas (Pakistani) Media worker for Samaa TV Killed on 12 February 2017 in Pakistan [UNESCO Statement] 1 UNESCO Condemns Killing of Journalists Assassinated Journalists in Pakistan Muhammad Jan (Pakistani) Reporter for the Urdu-language daily Qudrat and Brahui language daily Talar Quetta Killed on 12 January 2017 in Pakistan [UNESCO Statement] Shehzad Ahmed (Pakistani) Cameraman for Aaj TV Killed on 8 August 2016 in Pakistan [UNESCO Statement] Mehmood Khan (Pakistani) Cameraman for Dawn News Killed on 8 August 2016 in Pakistan [UNESCO Statement] Khurram Zaki (Pakistani) Editor of an online website, Let us Build Pakistan Killed on 7 May 2016 in Pakistan [UNESCO Statement] Muhammad Umar (Pakistani) Correspondent for local newspaper Daily Dera Killed on 16 January 2016 in Pakistan [UNESCO Statement] Hafeez Ur Rehman (Pakistani) Reporter for independent network Neo -

Pakistan 2020 LGBT Index and Exhibits
[NAME] [FIRM] [ADDRESS] [PHONE NUMBER] [FAX NUMBER] UNITED STATES DEPARTMENT OF JUSTICE EXECUTIVE OFFICE FOR IMMIGRATION REVIEW IMMIGRATION COURT [CITY, STATE] ) In the Matter of: ) ) File No.: A _____________ _______________________ ) ) In removal proceedings ) ) INDEX TO DOCUMENTATION OF COUNTRY CONDITIONS REGARDING PERSECUTION OF LGBTQ INDIVIDUALS IN PAKISTAN TAB SUMMARY GOVERNMENTAL SOURCES 1. Excerpt of Pakistan Penal Code § 377, available at: https://www.oecd.org/site/adboecdanti-corruptioninitiative/46816797.pdf • “Whoever voluntarily has carnal intercourse against the order of nature with any man, woman or animal, shall be punished with imprisonment for life, or with imprisonment of either description for a term which shall not be less than two years nor more than ten years, and shall also be liable to fine.” • “Explanation: Penetration is sufficient to constitute the carnal intercourse necessary to the offence described in this section.” 2. Bureau of Democracy, Human Rights and Labor, U.S. Dep’t of State, Pakistan 2019 Human Rights Report (Mar. 11, 2020), available at: https://www.state.gov/wp-content/uploads/2020/03/PAKISTAN-2019-HUMAN- RIGHTS-REPORT.pdf TAB SUMMARY • “Consensual same-sex sexual conduct is a criminal offense. The penalty for conviction of same-sex relations is a fine, two years to life imprisonment, or both. Lesbian, gay, bisexual, male transgender, and intersex persons rarely revealed their sexual orientation or gender identity in the public sphere. There were communities of openly transgender women, but they were marginalized and were frequently the targets of violence and harassment.” (p. 43) • “Violence and discrimination continued against lesbian, gay, bisexual, transgender, and intersex (LGBTI) persons. -

Tentative List of Applicants Who Applied in Membership Drive Phase - Ii Quota: Journalists
TENTATIVE LIST OF APPLICANTS WHO APPLIED IN MEMBERSHIP DRIVE PHASE - II QUOTA: JOURNALISTS DATE OF DATE OF MEMBERSHIP DRIVE S.NO CG NO CATEGORY APPLICANT NAME DESIGNATION DEPARTMENT MEMBERSHIP BIRTH DURATION 1 71095 I 8/7/2015 HANIF KHALID 8/14/1947 06-04-2015 to 13-05-2016 2 72640 I 8/25/2015 ABDUL QAYYUM FAROOQUI 6/30/1965 06-04-2015 to 13-05-2016 SENIOR 3 78315 I 5/9/2016 MATIULLAH JAN 11/2/1968 JHOUNRALIST WAQT NEWS 06-04-2015 to 13-05-2016 ANCHOPTERSON 4 85589 I 5/13/2016 TARIQ MEHMOOD 3/6/1976 DIRECTOR NEWS ASIAN NEWS NETWORK (ANN) 06-04-2015 to 13-05-2016 BUREAU CHIEF 5 3153 I 7/7/2015 MUHAMMAD SABIR SHAKIR 8/18/1968 ARY NEWS TELEVISION (MEDIA) ISLAMABAD 06-04-2015 to 13-05-2016 ANCHOR PERSON 6 3266 I 7/7/2015 MANZOOR AHMAD DAR 3/1/1970 CHIEF NEW EDITOR ONLINE INT NEWS NETOWRK ISLAMABAD 06-04-2015 to 13-05-2016 7 38023 I 2/15/2016 M ANWAR 11/29/1976 06-04-2015 to 13-05-2016 8 48758 I 8/13/2015 MAIN IMRAN YAQOOB 8/4/1972 DAWN NEWS 06-04-2015 to 13-05-2016 9 60348 I 6/5/2015 TANVEER HUSSAIN AWAN 10/24/1973 EDITOR 06-04-2015 to 13-05-2016 10 83178 I 5/13/2016 MIAN FAZAL 2/22/1962 06-04-2015 to 13-05-2016 11 83294 I 5/13/2016 SHAHZAD ANWAR 1/15/1972 BUREAU CHIEF 7 NEWS TV 06-04-2015 to 13-05-2016 12 79536 I 5/11/2016 HUMAIRA TAHIRA 2/11/1964 EXECUTIVE EDITOR DAILY NAWA I PAK 06-04-2015 to 13-05-2016 EDITOR 13 4238 I 7/28/2015 EJAZ AHMED ANJUM 7/10/1968 DAILY METRO WATCH ISLAMBAD 06-04-2015 to 13-05-2016 CORDINATOR 14 27831 I 8/6/2015 RAJA MEHTAB KHAN 5/2/1957 CHIEF EDITOR DAILY AUSAF 2D I&T CENTRE G-6/1-1 ISLAMMABAD 06-04-2015 to 13-05-2016 -

State, Nationalism, and Islamization, Palgrave Studies in Religion, Politics, and Policy, DOI 10.1007/978-3-319-54006-1 260 BIBLIOGRAPHY
BIBLIOGRAPHY 9/11 Commission. 2004. “The 9/11 Commission Report.” http://www.9- 11commission.gov/report/911Report.pdf. Abbas, Shemeem. 1993. “The Power of English in Pakistan.” World Englishes 12 (2): 147–156. doi:10.1111/j.1467-971X.1993.tb00017.x. Abbasi, Hamza Ali. 2016. “Saneha APS Qaum Ko Mutahid Kare Ga ...!” Bol News. http://www.awaztoday.pk/News-Talk-Shows/136583/Bol-News- Headquarter-16th-December-2016.aspx. Abbtakk.tv. 2015. “Using 21st Amendment to Malign Islam Is Improper: Siraj.” Abb Takk News. January 7. http://abbtakk.tv/en/using-21st-amendment-to- malign-islam-is-improper-siraj07012015/. Abdelal, Rawi. 2001. National Purpose in the World Economy: Post-Soviet States in Comparative Perspective. Ithaca: Cornell University Press. Abdul, Shehzad. 2016. “Erdogan Brings American Muslims Home to New Mosque.” Yahoo News.April2.http://news.yahoo.com/erdogan-brings- american-muslims-home-mosque-231504791.html. Ablak, Ersu. 2012. “Private Information?” Hurriyet Daily News, March 1. http:// www.hurriyetdailynews.com/private-information-.aspx?pageID=449&nID= 14964&NewsCatID=407. Abu-Odeh, Lama. 2004. “Modernizing Muslim Family Law: The Case of Egypt.” Vanderbilt Journal of Transnational Law 37: 1043. Adanali, Ahmet Hadi. 2008. “The Presidency of Religious Affairs and the Principle of Secularism in Turkey.” The Muslim World 98 (2–3): 228–241. doi:10.1111/j.1478-1913.2008.00221.x. Adanali, Hadi. 2002. “The Many Dimensions of Religious Instruction in Turkey.” In Religious Education in Schools: Ideas and Experiences from around the World, © The Author(s) 2017 259 R.M. Ali Saleem, State, Nationalism, and Islamization, Palgrave Studies in Religion, Politics, and Policy, DOI 10.1007/978-3-319-54006-1 260 BIBLIOGRAPHY edited by Zarrin T. -

Provisional Voter List of Associate Members 2020-2021
SARHAD CHAMMBER OF COMMERCE AND INDUSTRY Chamber House, G.T.Road, Peshawar. Tele No. +92-91-9225413-15, Fax No. +92-91-9225416 Emai.:[email protected], Websit:sccip.com.pk Provisional List of Associate Members 2020-2021 S No Representative/Firm Name/Address NTN # STN # CNIC # 1 Mohammad Ayaz 3419029-5 2100341902916 1730175925573 3GS CNG Gas Station Phandu Chowk Ring Road Peshawar 2 Irshad Khan 3648532-2 2120303182039 A & J Enterprises 8- Qaumi Market Torkham Landi Kotal Khyber Agency 3 Akbar Khan 2929648-0 1730162000601 A & Sons Hardware Store City Circular Road,Outside Lahori Gate,Near Bano,Peshawar 4 Tanveer Ahmad 2393366-6 3277876146001 1730107480749 A Sons Logistics A-21, 2nd Floor, Arsala Tower, New Rampura Gate,Peshawar 5 Asif Aziz 1288602-5 1730106123929 A.A Communications R # 2, 2nd Floor, Sarhad Chamber House, G.T. Road, Peshawar. 6 Azmat Ali 3914822-0 1730181862877 A.Ali Gems & Minerals 1- Swat Gems & Minerals Market Namak Mandi Peshawar 7 Muhammad Abid Khan 2796325-0 2120349031057 A.F Logistics FF-269, Deans Trade Centre, Cantt,Peshawar 8 Faiz Muhammad 1018246-2 1730115094249 A.M.Corporation 588/3, Gulshan Iqbal, Town,Jamrud Road, Peshawar 9 Mohammad asim 1445611-7 1730192426947 A.Q Enterprises B-12 Satta Gadai Market 32- The Mall Peshawar Cantt 10 Abdur Rehman 7155817-7 2120149805839 A.R Enterprises Office # 17, Ittehad Minerals Market, Old Bara District, Khyber Bara 11 Ali Muhammad 3394021-5 2100999811564 2170891022627 A.R Enterprises International 786- Main Ring Road Achini Chowk Hayatabad Peshawar 12 Aziz Ur Rehman 2670691-1