Rental Housing Application 04/2019
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

2008 Agreement for the Recognition of The
November 30, 2007 Agreement for the Recognition of the Qalipu Mi’kmaq Band FNI DOCUMENT 2007 NOVEMBER 30, 1 November 30, 2007 Table of Contents Parties and Preamble...................................................................................................... 3 Chapter 1 Definitions....................................................................................................... 4 Chapter 2 General Provisions ......................................................................................... 7 Chapter 3 Band Recognition and Registration .............................................................. 13 Chapter 4 Eligibility and Enrolment ............................................................................... 14 Chapter 5 Federal Programs......................................................................................... 21 Chapter 6 Governance Structure and Leadership Selection ......................................... 21 Chapter 7 Applicable Indian Act Provisions................................................................... 23 Chapter 8 Litigation Settlement, Release and Indemnity............................................... 24 Chapter 9 Ratification.................................................................................................... 25 Chapter 10 Implementation ........................................................................................... 28 Signatures ..................................................................................................................... 30 -
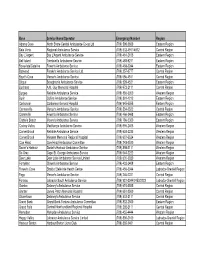
Revised Emergency Contact #S for Road Ambulance Operators
Base Service Name/Operator Emergency Number Region Adams Cove North Shore Central Ambulance Co-op Ltd (709) 598-2600 Eastern Region Baie Verte Regional Ambulance Service (709) 532-4911/4912 Central Region Bay L'Argent Bay L'Argent Ambulance Service (709) 461-2105 Eastern Region Bell Island Tremblett's Ambulance Service (709) 488-9211 Eastern Region Bonavista/Catalina Fewer's Ambulance Service (709) 468-2244 Eastern Region Botwood Freake's Ambulance Service Ltd. (709) 257-3777 Central Region Boyd's Cove Mercer's Ambulance Service (709) 656-4511 Central Region Brigus Broughton's Ambulance Service (709) 528-4521 Eastern Region Buchans A.M. Guy Memorial Hospital (709) 672-2111 Central Region Burgeo Reliable Ambulance Service (709) 886-3350 Western Region Burin Collins Ambulance Service (709) 891-1212 Eastern Region Carbonear Carbonear General Hospital (709) 945-5555 Eastern Region Carmanville Mercer's Ambulance Service (709) 534-2522 Central Region Clarenville Fewer's Ambulance Service (709) 466-3468 Eastern Region Clarke's Beach Moore's Ambulance Service (709) 786-5300 Eastern Region Codroy Valley MacKenzie Ambulance Service (709) 695-2405 Western Region Corner Brook Reliable Ambulance Service (709) 634-2235 Western Region Corner Brook Western Memorial Regional Hospital (709) 637-5524 Western Region Cow Head Cow Head Ambulance Committee (709) 243-2520 Western Region Daniel's Harbour Daniel's Harbour Ambulance Service (709) 898-2111 Western Region De Grau Cape St. George Ambulance Service (709) 644-2222 Western Region Deer Lake Deer Lake Ambulance -

Geology Map of Newfoundland
LEGEND POST-ORDOVICIAN OVERLAP SEQUENCES POST-ORDOVICIAN INTRUSIVE ROCKS Carboniferous (Viséan to Westphalian) Mesozoic Fluviatile and lacustrine, siliciclastic and minor carbonate rocks; intercalated marine, Gabbro and diabase siliciclastic, carbonate and evaporitic rocks; minor coal beds and mafic volcanic flows Devonian and Carboniferous Devonian and Carboniferous (Tournaisian) Granite and high silica granite (sensu stricto), and other granitoid intrusions Fluviatile and lacustrine sandstone, shale, conglomerate and minor carbonate rocks that are posttectonic relative to mid-Paleozoic orogenies Fluviatile and lacustrine, siliciclastic and carbonate rocks; subaerial, bimodal Silurian and Devonian volcanic rocks; may include some Late Silurian rocks Gabbro and diorite intrusions, including minor ultramafic phases Silurian and Devonian Posttectonic gabbro-syenite-granite-peralkaline granite suites and minor PRINCIPAL Shallow marine sandstone, conglomerate, limey shale and thin-bedded limestone unseparated volcanic rocks (northwest of Red Indian Line); granitoid suites, varying from pretectonic to syntectonic, relative to mid-Paleozoic orogenies (southeast of TECTONIC DIVISIONS Silurian Red Indian Line) TACONIAN Bimodal to mainly felsic subaerial volcanic rocks; includes unseparated ALLOCHTHON sedimentary rocks of mainly fluviatile and lacustrine facies GANDER ZONE Stratified rocks Shallow marine and non-marine siliciclastic sedimentary rocks, including Cambrian(?) and Ordovician 0 150 sandstone, shale and conglomerate Quartzite, psammite, -

Regional News
REGIONAL FIS E IES NEWS J liaRY 1970 ( 1 • Mdeit,k40 111.111111111...leit 9 DEPARTMENT OF FISHERIES OF CANADA NEWFOUNDLAND REGION REDUCTION PLANT OFFICIALLY OPENED The ne3 3/4-million NATLAKE herring reduction plant at Burgeo was officially opened January 28th by Premier J. R. Smallwood. Among special guests attending the opening ceremonies were: federal Transport Minister Don Jamieson, provincial Minister of Fisheries A. Maloney and our Regional Director, H. R. Bradley. Privately financed, the new plant is a joint effort of Spencer Lake, the Clyde Lake Group and National Sea Products of Nova Scotia. Ten herring seiners from Nova Scotia, New Brunswick and British Columbia are under contract to land catches at the plant. Fifty people will be employed as production workers at the plant which will operate on a 21-hour, three shift basis. - 0 - 0 - 0 - ATTEND CAMFI CONFERENCE Four representatives of Regional Headquarters staff are attending the Conference on Automation and Mechanization in the Fishing Industry being held in Montreal February 3 - 6. The conference is sponsored by the Federal-Provincial Atlantic Fisheries Committee which is comprised of the deputy ministers responsible for fisheries in the Federal Government and the governments of Quebec, Nova Scotia, New Brunswick, Prince Edward Island and Newfoundland. The Secretariat for the conference was provided by the Industrial Development Service, Department of Fisheries and Forestry, Ottawa. Attending the conference from the Newfoundland. Region were: J. P. Hennessey, R. n. Prince, m. Barnes and E. B. Dunne. ****** ****** FROZEN TROUT RETURN TO LIFE A true story told by Bob Ebsary, a former technician with our Inspection Laboratory, makes one wonder whether or not trout, like cats, have nine lives. -

ROUTING GUIDE - Less Than Truckload
ROUTING GUIDE - Less Than Truckload Updated December 17, 2019 Serviced Out Of City Prov Routing City Carrier Name ABRAHAMS COVE NL TORONTO, ON Interline Point ADAMS COVE NL TORONTO, ON Interline Point ADEYTON NL TORONTO, ON Interline Point ADMIRALS BEACH NL TORONTO, ON Interline Point ADMIRALS COVE NL TORONTO, ON Interline Point ALLANS ISLAND NL TORONTO, ON Interline Point AMHERST COVE NL TORONTO, ON Interline Point ANCHOR POINT NL TORONTO, ON Interline Point ANGELS COVE NL TORONTO, ON Interline Point APPLETON NL TORONTO, ON Interline Point AQUAFORTE NL TORONTO, ON Interline Point ARGENTIA NL TORONTO, ON Interline Point ARNOLDS COVE NL TORONTO, ON Interline Point ASPEN COVE NL TORONTO, ON Interline Point ASPEY BROOK NL TORONTO, ON Interline Point AVONDALE NL TORONTO, ON Interline Point BACK COVE NL TORONTO, ON Interline Point BACK HARBOUR NL TORONTO, ON Interline Point BACON COVE NL TORONTO, ON Interline Point BADGER NL TORONTO, ON Interline Point BADGERS QUAY NL TORONTO, ON Interline Point BAIE VERTE NL TORONTO, ON Interline Point BAINE HARBOUR NL TORONTO, ON Interline Point BAKERS BROOK NL TORONTO, ON Interline Point BARACHOIS BROOK NL TORONTO, ON Interline Point BARENEED NL TORONTO, ON Interline Point BARR'D HARBOUR NL TORONTO, ON Interline Point BARR'D ISLANDS NL TORONTO, ON Interline Point BARTLETTS HARBOUR NL TORONTO, ON Interline Point BAULINE NL TORONTO, ON Interline Point BAULINE EAST NL TORONTO, ON Interline Point BAY BULLS NL TORONTO, ON Interline Point BAY DE VERDE NL TORONTO, ON Interline Point BAY L'ARGENT NL TORONTO, ON -

Overview of the International Appalachian Trail Extended Into
Overview of the International Appalachian Trail n Extended into Newfoundland [Amended July 2005] a m r r u o o e N rb v a Co e H p s n k' eo a o ig E C o P L C y S a I y B a a B Sacred H E w Bay L o a L ll a H E h B S F Griquet Hr O IT rm A Milan A R St. Lunaire Bay ST Great Brehat Bay k o ro B Square Bay ig B Northwest St. Anthony Arm P H a o t H w ey r Cr v e ém ill a e Goose Cove Hr illè re STRAIT OF BELLE ISLE HAR E B West AY Br ook Ariege (Belvy) Bay Ste. Genevieve Bay e Great Islets Hr k a k L B ile M n e t T s e St w . M th a u rga o re S t B Croque Harbour ay ay r B r B ave ro lie Be o Pi k CAPE ROUGE Northeast Crouse PENINSULA Cape RougeHarbour ove y C C Squid a o B Roddickton n ST.JOHN BAY y c e h North Summit n He m GREY ISLANDS a i r h b C o u St. John Island r m r A Otter Cove e d i Torrent Cove B BELL ISLAND Englee Port au Choix Canada r Bay ive t R Grey Islands Harbour as Ingornachoix Bay E ay s B Hooping Harbour wke Cat Cove Ha Hooping Harbour E C Williamsport N E Fourché Harbour R S W Eastern Tro N use Blue Pd I r C A ove Pi L .649 A ge on T C Blue Mountain ov Deer Cove e N G . -

Office Allowances - Office Accommodations 01-Apr-18 to 31-Mar-19
House of Assembly Newfoundland and Labrador Member Accountability and Disclosure Report Office Allowances - Office Accommodations 01-Apr-18 to 31-Mar-19 Dean, Jerry, MHA Page: 1 of 1 Summary of Transactions Processed to Date for Fiscal 2018/19 Expenditure Limit (Net of HST): $19,200.00 Transactions Processed as of: 31-Mar-19 Expenditures Processed to Date (Net of HST): $19,200.00 Funds Available (Net of HST): $0.00 Percent of Funds Expended to Date: 100.0% Date Source Document # Vendor Name Expenditure Details Amount 01-Apr-18 HOA004815 W REID CONSTRUCTION Lease payment for the Constituency Office of the MHA for the District of Exploits 1,600.00 LTD located in Bishop's Falls. 01-May-18 HOA004871 W REID CONSTRUCTION Lease payment for the Constituency Office of the MHA for the District of Exploits 1,600.00 LTD located in Bishop's Falls. 01-Jun-18 HOA004908 W REID CONSTRUCTION Lease payment for the Constituency Office of the MHA for the District of Exploits 1,600.00 LTD located in Bishop's Falls. 01-Jul-18 HOA004946 W REID CONSTRUCTION Lease payment for the Constituency Office of the MHA for the District of Exploits 1,600.00 LTD located in Bishop's Falls. 01-Aug-18 HOA004983 W REID CONSTRUCTION Lease payment for the Constituency Office of the MHA for the District of Exploits 1,600.00 LTD located in Bishop's Falls. 01-Sep-18 HOA005021 W REID CONSTRUCTION Lease payment for the Constituency Office of the MHA for the District of Exploits 1,600.00 LTD located in Bishop's Falls. -
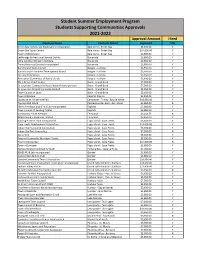
Students Supporting Communities Program
Student Summer Employment Program Students Supporting Communities Approvals 2021-2022 Approval Amount Hired Employer Name Electoral District Approved Y/N Green Bay Community Employment Corporation Baie Verte - Green Bay $3,650.00 Y Green Bay Youth Centre Baie Verte - Green Bay $14,600.00 Y Town of Woodstock Baie Verte - Green Bay $3,650.00 Y Lethbridge & Area Local Service District Bonavista $3,650.00 Y Little Catalina Women's Institute Bonavista $3,650.00 Y Trinity Historical Society Incorporated Bonavista $3,650.00 Y Burnt Island Town council Burgeo - La Poile $3,550.00 Y Burnt Islands Economic Development Board Burgeo - La Poile $3,500.00 Y DG Four Enterprises Burgeo - La Poile $3,650.00 Y Recreation Committee of Burnt Islands Burgeo - La Poile $3,650.00 Y Main Street Youth Centre Burin - Grand Bank $7,300.00 Y St. Lawrence Community Youth Network Incorporated Burin - Grand Bank $7,300.00 Y St. Lawrence Retirement Living Limited Burin - Grand Bank $3,650.00 Y Town Council of Lawn Burin - Grand Bank $3,650.00 Y Town of Bauline Cape St. Francis $3,550.00 Y Society of St. Vincent de Paul Carbonear - Trinity - Bay de Verde $10,950.00 Y Tourism Bell Island Conception Bay East - Bell Island $3,650.00 N Norris Arm Boys and Girls Club Incorporated Exploits $7,300.00 Y Town Council of Leading Tickles Exploits $3,650.00 Y Community Youth Network Ferryland $3,218.75 N MMB Dining Enterprises Limited Ferryland $3,650.00 Y Banting Historic Trust Incorporated Fogo Island - Cape Freels $3,650.00 Y Cape Freels Development Association Fogo Island - -

BOARD MEETING –Norris Arm 1:00 P.M. December 7, 2017 Attendance
Central Newfoundland Waste Management P. O. Box 254, Norris Arm, NL, A0G 3M0 Phone: 709 653 2900 Fax :709 653 2920 Web: www.cnwmc.com E-mail: [email protected] BOARD MEETING –Norris Arm 1:00 p.m. December 7, 2017 Attendance Terry Best Badger/Buchans/Buchans Junction/Millertown – Ward 1 Kevin Butt NWI/Twillingate – Ward 3 Wayne Collins Fogo Island – Ward 4 Keith Howell Gander Bay – Ward 5 Lloyd Pickett Indian Bay – Ward 6 Glenn Arnold Terra Nova – Ward 7 Percy Farwell Town of Gander - Ward 8 Darrin Finn Town of Grand Falls-Windsor – Ward 9 Ross Rowsell Norris Arm/Norris Arm North – Ward 11 Derrick Luff Direct Haul – Ward 12 Ed Evans Chief Administrative Officer - CNWM Karen White Attwood Manager of Finance/Administration – CNWM Mark Attwood Manager of Operations – CNWM Jerry Collins Dept of Municipal Affairs and Environment - Conference Call Ian Duffett Dept of Municipal Affairs and Environment – Conference Call Apologies Brad Hefford Service NL Wayne Lynch Service NL Robert Elliott Point Leamington – Ward 2 Perry Pond Bishops Falls/Botwood/Lewisporte – Ward 10 1. Review of Minutes of November 9, 2017 MOTION: Moved by G. Arnold to adopt the minutes of November 9, 2017. Seconded by R. Rowsell. M/C 2. Business Arising Mayor Betty Clarke has stepped down as representative of Ward 10 (Botwood, Bishops Falls, and Lewisporte). Perry Pond will now represent Ward 10. 3. Technical Committee – Representatives from the Board, Government and engineers from the Towns of Grand Falls – Windsor and Gander will continue to sit at the Technical committee December 7, 2017 4. Financial Report MOTION: Moved by W. -

Rental Housing Portfolio March 2021.Xlsx
Rental Housing Portfolio Profile by Region - AVALON - March 31, 2021 NL Affordable Housing Partner Rent Federal Community Community Housing Approved Units Managed Co-op Supplement Portfolio Total Total Housing Private Sector Non Profit Adams Cove 1 1 Arnold's Cove 29 10 39 Avondale 3 3 Bareneed 1 1 Bay Bulls 1 1 10 12 Bay Roberts 4 15 19 Bay de Verde 1 1 Bell Island 90 10 16 116 Branch 1 1 Brigus 5 5 Brownsdale 1 1 Bryants Cove 1 1 Butlerville 8 8 Carbonear 26 4 31 10 28 99 Chapel Cove 1 1 Clarke's Beach 14 24 38 Colinet 2 2 Colliers 3 3 Come by Chance 3 3 Conception Bay South 36 8 14 3 16 77 Conception Harbour 8 8 Cupids 8 8 Cupids Crossing 1 1 Dildo 1 1 Dunville 11 1 12 Ferryland 6 6 Fox Harbour 1 1 Freshwater, P. Bay 8 8 Gaskiers 2 2 Rental Housing Portfolio Profile by Region - AVALON - March 31, 2021 NL Affordable Housing Partner Rent Federal Community Community Housing Approved Units Managed Co-op Supplement Portfolio Total Total Housing Goobies 2 2 Goulds 8 4 12 Green's Harbour 2 2 Hant's Harbour 0 Harbour Grace 14 2 6 22 Harbour Main 1 1 Heart's Content 2 2 Heart's Delight 3 12 15 Heart's Desire 2 2 Holyrood 13 38 51 Islingston 2 2 Jerseyside 4 4 Kelligrews 24 24 Kilbride 1 24 25 Lower Island Cove 1 1 Makinsons 2 1 3 Marysvale 4 4 Mount Carmel-Mitchell's Brook 2 2 Mount Pearl 208 52 18 10 24 28 220 560 New Harbour 1 10 11 New Perlican 0 Norman's Cove-Long Cove 5 12 17 North River 4 1 5 O'Donnels 2 2 Ochre Pit Cove 1 1 Old Perlican 1 8 9 Paradise 4 14 4 22 Placentia 28 2 6 40 76 Point Lance 0 Port de Grave 0 Rental Housing Portfolio Profile by Region - AVALON - March 31, 2021 NL Affordable Housing Partner Rent Federal Community Community Housing Approved Units Managed Co-op Supplement Portfolio Total Total Housing Portugal Cove/ St. -

HYDROGEOLOGY 50°0' Central Newfoundland
55°15' 55°0' 54°45' 54°30' 54°15' 54°0' 53°45' 53°30' 53°15' 50°15' Department of Environment and Conservation Department of Natural Resources Map No. 3b HYDROGEOLOGY 50°0' Central Newfoundland Well Yield Well Depth 50°0' Characteristics Characteristics (m) Number (L/min) Hydrostratigraphic Unit Lithology of Wells Average Median Average Median Unit 1 schist, gneiss, Low to Moderate Yield 73 20 6 51 48 quartzite, slate Metamorphic Strata siltstone, Unit 2 conglomerate, argillite, Low to Moderate Yield 1403 20 7 51 46 greywacke, with Sedimentary Strata minor volcanic 49°45' flows and tuff Unit 3 basic pillow Low to Moderate Yield lava, flows, 723 22 9 50 46 Barr'D Islands Volcanic Strata breccia and tuff 49°45' Fogo Joe Batt's Arm Tilting Unit 4 mafic and ultramafic Shoal Bay Pike's Arm Low Yield intrusions of ophiolite 13 9 7 58 61 Herring Neck Change Islands complexes FogoC oIsolkasn Pdond Ophiolite Complexes Durrell Deep Bay Fogo Island Region Unit 5 granite, granodiorite, Salt Harbour N o r t h Twillingate Island Harbour diabase, and diorite 688 22 9 44 37 Little Harbour Cobbs Arm A t l a n t i c Low to Moderate Yield Too Good Arm Seldom intrusions Notre Dame Bay O c e a n Plutonic Strata Gilliards Cove F Jenkins Cove rid Keattyle Cove Black Duck Cove Little Seldom Tizzard's Harbour B Rogers Cove ay Indian Cove Surficial deposits - Unconsolidated sediments Stag Harbour Newville Valley Pond Moreton's Harbour Surficial Hydrostratigraphic Units Fairbanks-Hillgrade Unit A - Till Deposits Hillgrade Port Albert Well yields range from 2 litres per minute (L/min) to 136 L/min and averaged 29 L/min Bridgeport 49°30' Virgin Arm-Carter's Cove with a median value of 18 L/min. -

Review of Applications for Membership in the Qalipu Mi'kmaq First Nation Band Important Information for Applicants July 2013
IMPORTANT INFORMATION FOR APPLICANTS JULY 2013 REVIEW OF APPLICATIONS FOR MEMBERSHIP IN THE QALIPU MI’KMAQ FIRST NATION BAND Note: Applicants are advised that this document is not a substitute for the June 2013 Supplemental Agreement, the June 2013 Directive to the Enrolment Committee, or the 2008 Agreement. This Information Update is intended to provide general guidelines on what information applicants can start to gather to support their application for enrolment in the Qalipu Mi’kmaq First Nation. On July 4, 2013, Canada and the Federation of Newfoundland Indians (FNI) announced a Supplemental Agreement that clarifies the process for enrolment in the Qalipu Mi’kmaq First Nation and resolves issues that emerged in the implementation of the 2008 Agreement. All applications submitted between December 1, 2008, and November 30, 2012, except those previously rejected, will be reviewed to ensure that applicants meet the criteria for eligibility set out in the 2008 Agreement. This includes the applications of all those who have gained Indian status as members of the Qalipu Mi’kmaq First Nation. No new applications will be accepted. In November 2013, all applicants, except those Checklist previously rejected, will be sent a letter. Where an application is invalid, the letter will advise applicants that Ensure your address is up to date (Section A) their application is denied. Where an application is valid, Provide birth certificate, and proof of the letter will outline general documentation and request, by September 3, 2013 (Section B) informational requirements as well as where to send additional information applicants may wish to submit. It Understand Requirements to support is the sole responsibility of applicants to determine what self-identification (Section C) additional documentation they wish to submit in support Gather documents to support demonstration of their applications.