Serial Extraction
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Spring 2012 Ad Tk Volume 84 | No
VOLUME 84 | NO. 1 BulletinPACIFIC COAST SOCIETY OF ORTHODONTISTS Faculty Files: 15 Long-Term Stability Study of American Board of Orthodontics Cases Seasoned Practitioner’s Corner: 27 Dr. Terry McDonald Interviews Dr. Milton Chan on Canine Substitution Portrait of a Professional: 34 Leonard V. Cheney, DDS SPRING 2012 AD TK VOLUME 84 | NO. 1 published quarterly by and for the pacific coast society of orthodontists Usps 114-950 Issn 0191-7951 edItor Bulletin Gerald nelson, dds NEWS AND REVIEWS OF THE PACIFIC COAST SOCIETY OF ORTHODONTISTS 279 Vernon st., apt. 2 oakland, ca 94619 (510) 530-0744 Features northern reGIon edItors Bruce p. hawley, dds, msd presIdent’s messaGe 2 4215 -198th st. s.W., #204 PCSO Delegation to the AAO | By Dr. Rob Merrill, PCSO President, 2011-2012 Lynnwood, Wa 98036-6738 charity h. siu, DMD, Frcd (c) execUtIVe dIrector’s Letter 4 1807-805 W Broadway Vancouver, Bc V5Z 1K1 canada Bittersweet | By Jill Nowak, PCSO Executive Director centraL reGIon edItor Dr. shahram nabipour edItorIaL 5 2295 Francisco st #105 Accreditation | By Dr. Gerald Nelson, PCSO Bulletin Editor san Francisco ca 94123 soUthern reGIon edItor pcso BUsINESS 8 douglas hom, dds AAO Trustee’s Report | Dr. Robert Varner 1245 W huntington dr #200 arcadia, ca 91007 FACULtY FILes 15 pUBLIcatIon manaGer Long-Term Stability Study of American Board of Orthodontics Cases | anne evers 2856 diamond street By Dr. Raymond M. Sugiyama, DDS, MS, FACD, FICD san Francisco, ca 94131 Los Alamitos/Loma Linda University; edited by Dr. Ib Nielsen (415) 333-4785 phone/fax adVertIsInG manaGer PRACTIce manaGement dIarY 26 Kathy richardson/AAOSI Handouts | By Dr. -

Serial Extraction: Is It a Panacea for Crowded Arches?
Review article Annals and Essences of Dentistry SERIAL EXTRACTION: IS IT A PANACEA FOR CROWDED ARCHES? * Radhika Chopra * Senior Lecturer, Karnavati School of Dentistry, Ghandhinagar ABSTRACT Serial Extraction or the guidance of eruption is an age old procedure to correct crowded arches and is still used in routine dental practice. But the efficacy of this procedure has always been controversial and it requires very precise clinical skill for a favorable outcome. This article presents a review regarding the proper selection of cases for serial extraction, its limitations and various adjuncts that are required to get good results. INTRODUCTION: Robert Bunon,23 in his Essay on Diseases of Intercepting certain forms of malocculsion Teeth, published in 1743, made the first reference with a preliminary program of serial extraction has a to early extractions. legitimate place in orthodontics. Dewel defines Linderer23(1851) wrote that quite often in serial extraction as an orthodontic treatment order to accommodate lateral incisor, one must strip procedure that involves the orderly removal of or extract deciduous canines and to relieve selected deciduous and permanent teeth in a subsequent crowding in buccal segments, removal predetermined sequence. of first premolar would be necessary. Serial extraction is based on the premise Strangely their early recommendations that in certain cases the orthodontist is confronted were ignored for nearly two centuries. It was not with a continuing discrepancy between total tooth until the 1947-48 Transactions of the European material and deficient arch length. He is presented Orthodontic Society had been published that the with a limited amount of basal bone, present or procedure was again presented. -

Serial Extraction
أ. د. أكرم فيصل الحويزي 5th Year Lec. No. 11 SERIAL EXTRACTION Serial extraction involves the timed extraction of primary and, ultimately, permanent teeth to relieve severe crowding and to guide the erupting permanent teeth into a more favorable position. It is better termed it ‘Guidance of Eruption’ or ‘Guidance of Occlusion’. Commonly at 7-8 years of age the maxillary and mandibular central incisors have erupted, but there is inadequate space in anterior segments to allow normal eruption and positioning of lateral incisors. In some cases, mandibular lateral incisors have already erupted but they are usually lingually positioned and rotated. The same is with the maxillary lateral incisors. The orthodontist has four option: Wait for growth to provide more space and re-evaluate later. Expansion of the dental arch. However, the stability of expansion may be compromised by the insufficient alveolar basal bone. Cement a transpalatal or lingual bar to preserve the Leeway space for later on. Serial extraction can reduce crowding and irregularity during the mixed dentition. HISTORY Bunon (1743) made the first reference to the extraction of deciduous teeth to achieve a better alignment of permanent teeth. In 1929, Kjellgren of Sweden first used the term ‘serial extraction’. In the 1940s, the technique was popularised in the United States by Nance who is known as the Father of serial extraction. It was advocated originally as a method to treat severe crowding by their own dentists without or with only minimal use of appliance therapy, thus minimizing demands upon the orthodontic service. Although serial extraction makes later comprehensive treatment easier and often quicker, by itself it almost never results in ideal tooth position or closure of excess space. -

Serial Extraction: a Review
8902 Indian Journal of Forensic Medicine & Toxicology, October-December 2020, Vol. 14, No. 4 Serial Extraction: A Review Sulagna Pradhan1, Sushant Mohanty2, Sonu Acharya3, Sonali Bhuyan1, Mrinali Shukla1 1Post Graduate Trainee, 2Professor & Head, 3Professor, Department of Paediatric and Preventive Dentistry, Institute of Dental Sciences, Siksha O Anusandhan (Deemed to be University), Bhubaneswar 751003,Odisha, India Abstract Serial extraction or eruption with guidance is a pre-planned, premature extraction of certain primary teeth to create space that has been compromised. It is followed by the extraction of certain permanent teeth to maintain the proper proportion of tooth size and dentoalveolar bone space. However, this procedure is challenging as it requires in-depth clinical knowledge and skill. This article provides essential insights to the clinicians to identify and categorize the cases meticulously for serial extraction, apply both theoretical and practical aspects of growth and development, and diagnose the alarming signs of primary crowding in early mixed dentition period. Keywords: Serial Extraction, Primary Teeth, Mixed Dentition, Developing Malocclusion. Introduction aesthetic of the rest. Paisson was the first to recommend the procedure to relieve the crowding and align the Serial extraction is fundamentally based on the teeth. Robert Bunon in 1743, in his publication“Essay concept that in certain cases the orthodontists face a on Diseases of Teeth”, first wrote about the importance challenging situation such as limited space between the of early extractions. Linderer (1851)5 suggested that arch length and total tooth material. Hence, it is crucial the primary canines should be stripped or removed to enlarge the basal bone, so that all the teeth get proper to accommodate the lateral incisors followed by the accommodation. -
Orthodontic Management of Missing Teeth
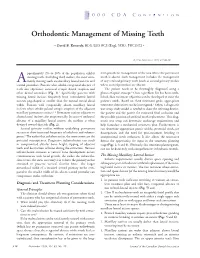
2000 CDA CONVENTION Orthodontic Management of Missing Teeth • David B. Kennedy, BDS, LDS RCS (Eng), MSD, FRCD(C) • © J Can Dent Assoc 1999; 65:548-50 pproximately 2% to 10% of the population exhibit term prosthetic management of the area where the permanent missing teeth. Excluding third molars, the most com- tooth is absent. Such management includes the management A monly missing teeth are maxillary lateral incisors and of any retained primary teeth (such as second primary molars second premolars. Patients who exhibit congenital absence of where second premolars are absent). teeth also experience increased ectopic dental eruption and The patient needs to be thoroughly diagnosed using a other dental anomalies (Fig. 1).1 Specifically, patients with planes-of-space concept.3 Once a problem list has been estab- missing lateral incisors frequently have contralateral lateral lished, then treatment objectives can be developed to meet the incisors peg-shaped or smaller than the normal mesial distal patient’s needs. Based on these treatment goals, appropriate width. Patients with congenitally absent maxillary lateral treatment alternatives can be investigated.3 Often, a diagnostic incisors often exhibit palatal ectopic eruption of the adjacent wax setup study model is needed to show the referring dentist, maxillary permanent canines.1,2 Permanent canines adjacent to the patient and the parent the estimated final occlusion and absent lateral incisors also erupt mesially. In cases of unilateral the possible position of artificial tooth replacement. This diag- absence of a maxillary lateral incisor, the midline is often nostic wax setup can determine anchorage requirements and deviated toward that side (Fig. -

Relapse of Anterior Crowding in Patients Treated with Extraction and Nonextraction of Premolars
ORIGINAL ARTICLE Relapse of anterior crowding in patients treated with extraction and nonextraction of premolars Aslıhan Ertan Erdinc,a Ram S. Nanda,b and Erdal Is¸ ıksalc Izmir, Turkey, and Oklahoma City, Okla Introduction: The purpose of this study was to evaluate long-term stability of incisor crowding in orthodontic patients treated with and without premolar extractions. Methods: Dental casts and cephalometric records of 98 patients were evaluated before treatment (T1), at posttreatment (T2), and at postretention (T3). Half of the patients had been treated with extractions, and half were treated nonextraction. Results: Irregularity, as measured by the irregularity index, decreased 5.51 mm in the extraction group and 2.38 mm in the nonextraction group. Mandibular incisor irregularity increased 0.97 mm in the extraction group and 0.99 mm in the nonextraction group, respectively, in the postretention period. Maxillary incisor irregularity relapse was smaller than mandibular incisor relapse for both groups. Intercanine width expanded during treatment. At T3, mandibular intercanine width decreased in both groups, but the differences were not statistically significant. At T3, intermolar width was stable, arch depth decreased, overbite and overjet slightly increased, SN mandibular plane angle decreased, and incisor positions in both groups tended to return to T1 values. Clinically acceptable stability was obtained. Conclusions: With the exception of the interincisal angle, no statistically significant differences were recorded between the extraction and nonextraction groups from T2 to T3. No statistically significant correlations were found between any variables studied and mandibular incisor irregularity at T1, T2, and T3. (Am J Orthod Dentofacial Orthop 2006;129:775-84) major goal of orthodontic treatment is to arises as to which treatment procedure is most helpful achieve long-term stability of posttreatment in achieving long-term stability. -

Curriculum Vitae I. Name Ariana Gabriela Feizi [email protected] II. Education University of Maryland School of Dentist
Evaluating Oropharyngeal Airway Volume in Patients with Class II Dental Relationships with Extractions vs Non-Extraction Orthodontic Treatment Item Type dissertation Authors Feizi, Ariana Gabriela Publication Date 2021 Abstract Purpose: The purpose of this study is to support the position of the AAO by demonstrating that the oropharyngeal volume does not decrease as a result of premolar extractions and orthodontic treatment. Materials and Methods: Cone-beam CT’s were obt... Keywords oropharyngeal airway volume; Orthodontics; Tooth Extraction Download date 29/09/2021 16:15:11 Link to Item http://hdl.handle.net/10713/15772 Curriculum Vitae I. Name Ariana Gabriela Feizi [email protected] II. Education University of Maryland School of Dentistry Baltimore, MD Certificate in Orthodontics and Master of Science in Biomedical Sciences, Expected Graduation May 2021 University of Maryland School of Dentistry Baltimore, MD Doctor of Dental Surgery, May 2018 University of Maryland, College Park, MD Bachelor of Science in Physiology and Neurobiology, May 2014 III. Research Master’s Thesis University of Maryland School of Dentistry Department of Orthodontics Baltimore, MD Evaluating oropharyngeal airway volume in patients with Class II dental relationships with extraction vs non-extraction orthodontic treatment July 2018- Present Journal of General Dentistry Publication University of Maryland School of Dentistry Department of Orthodontics Baltimore, MD What every general dentist needs to know about clear aligners Published July 2020 Research Assistant University of Maryland School of Dentistry Department of Orthodontics Baltimore, MD Dental and Skeletal Changes seen on CBCT with Damon Self-ligating Bracket System vs. Conventional Bracket System 2017 Research Program University of Maryland Gemstone Honors Society, College Park, MD Evaluating Linear-Radial Electrode Conformations for Tissue Repair and Organizing a Device for Experimentation August 2010- May 2014 IV. -

An Evaluation of Serial Extraction Among Navajo Indian Children
An evaluation of serial extraction among Navajo Indian children Russell 0. Glauser, D.D.S.* Phoenix, A&. W ithin the borders of the United States, there are more than 100,000 Indian children living in rural areas where no orthodontists are available to provide orthodontic services. Of the varied malocclusion problems, many are the result of dental crowding. The crowding problem appears to be accentuated in this ethnic group by large mesiodistal crown diameter. In a survey of tooth size that I carried out on Navajo students, it was found that, on the average, the individual Navajo tooth is 0.37 mm. larger than the average Caucasian tooth. The Navajo lateral incisor is the tooth which varies to the greatest extent. This tendency toward large teeth has also been demonstrated in the Aleut dentition.14 The present study was designed to evaluate serial extraction as an adjunct to interceptive orthodontic treatment and particularly to ascertain whether it may be applied advantageously in situations where comprehensive orthodontic services are not available. For the purposes of this article, serial extraction is defined as the predetermined sequential removal of deciduous teeth and four premolars, one in each quadrant, to allow sufficient space for alignment of per- manent incisors and subsequent favorable eruption and interdigitation of the remaining permanent canines and premolars. Methods and procedures In a screening examination performed on 816 Navajo children residing on the Navajo Reservation, 279 children who had clinical symptoms of dental crowding were selected for appraisal. Orthodontic records were taken on all children selected. These records consisted of a patient history, full-mouth peri- apical roentgenograms, left and right oblique cephalometric roentgenograms, Presented at the meeting of the Eastman Orthodontic Alumni Association, Rochester, N. -

Serial Extraction in Orthodontics – Review Article Dr
European Journal of Molecular & Clinical Medicine ISSN 2515-8260 Volume 07, Issue 2, 2020 Serial Extraction In Orthodontics – Review Article Dr. Arif Yezdani.A1 , Dr. Nithya Nandhini.P 2, Dr.Padmavati.R 3 1. Professor and Director, Department of Orthodontics and Dentofacial Orthopedics, Sree Balaji Dental College and Hospital, Bharath Institute of Higher Education and Research, Chennai. 2. Undergraduate student, Sree Balaji Dental College and Hospital, Bharath Institute of Higher Education and Research, Chennai. 3. Senior Lecturer, Department of Orthodontics and Dentofacial Orthopedics, Sree Balaji Dental College and Hospital, Bharath Institute of Higher Education and Research, Chennai. Department of Orthodontics and Dentofacial Orthopedics, Sree Balaji Dental College and Hospital, Bharath Institute of Higher Education and Research, Chennai. Mail id: [email protected] Abstract Serial extraction or guidance of eruption is the planned and sequential extraction of certain deciduous teeth followed by extraction of specific permanent teeth in the early mixed dentition period in order to encourage the spontaneous correction of tooth irregularities. It is an integral part of interceptive orthodontics aimed at reducing the severity of the developing malocclusion. Keywords: Serial extraction, mixed dentition, Interceptive orthodontics, developing malocclusion, preventive procedure Introduction Serial extraction is a sequential plan of premature removal of one or more deciduous teeth so as to enhance alignment of succedaneous permanent teeth with eventual removal of permanent teeth to take care of the right ratio between tooth size and available bone. [1] Dental crowding exists when there is more tooth material in relation to the basal and alveolar bone that supports the teeth. [2] This procedure is typically done at an early mixed dentition period. -

Managing the Developing Occlusion
Managing the Developing Occlusion A guide for dental practitioners INTRODUCTION Whether knowingly or not, every dentist ORTHODONTIC ADVICE who treats children practices orthodontics. First, when considering potential orthodontic It is not enough to think of orthodontics advice for the patient, the dental practitioner should consider the following general questions: as being solely concerned with appliances. 1. Is the patient’s basic dental health under Orthodontics is the longitudinal care of control and is the parent available for the developing occlusion and any consultation? problems associated with it. All qualified 2. Is the orthodontic condition minor, moderate dental practitioners should be encouraged or severe in nature and does it cause the patient to consider the orthodontic requirements concern? of their patients. 3. Can the practitioner provide adequate advice in the short, medium and long term, or is specialist advice required and, if so, at what level? This booklet is designed to help general dental practitioners examine children 4. Would the patient and parent prefer a specialist opinion? from an orthodontic viewpoint. It will highlight the assessment of patients at TREATMENT different stages of dental development Secondly, when considering potential orthodontic and will outline the interceptive treatment for patients, the dental practitioner should consider the following general questions: procedures and treatments available to deal with the conditions most commonly 1. Does the patient want the condition changed? encountered. 2. Is the patient receptive to the idea of, and available for, orthodontic treatment? Before specific assessment and 3. Is specialist treatment required and, if so, at treatments are considered, a general what level? view of the developing dentition and face is advisable. -
James A. Mcnamara Jr
E NTR E VISTA Uma entrevista com James A. McNamara Jr. • Graduado em Odontologia e Ortodontia pela University of California, San Francisco. • Doutor em Anatomia pela University of Michigan. • Professor da Cadeira Thomas M. e Doris Graber, no Departamento de Ortodontia e Odontopediatria - University of Michigan. • Professor de Biologia Celular e Desenvolvimento - University of Michigan. • Professor Pesquisador no Centro para Crescimento e Desenvolvimento Humano na University of Michigan. • Autor do livro “Orthodontics and Dentofacial Orthopedics”. • Prêmio Milo Hellman Research (AAO - 1973). • Conferencista E. Sheldon Friel (Sociedade Europeia de Ortodontia - 1979). • Prêmio Jacob A. Salzmann (AAO - 1994). • Prêmio James E. Brophy (AAO - 2001). • Conferencista Valentine Mershon (AAO - 2002). • Prêmio Albert H. Ketcham (AAO - 2008). • Diplomado pelo American Board of Orthodontics - ABO. • Fellow do American College of Dentists. • Ex-Presidente da Edward H. Angle Society of Orthodontists - Midwest. • Editor-Chefe da série “Craniofacial Growth Monograph” - publicada pela University of Michigan. • Mais de 250 artigos publicados. • Escreveu, editou ou contribuiu com mais de 68 livros. • Ministrou cursos e conferências em 37 países. Conheci James A. McNamara Jr. no final dos anos 70, quando nós dois nos tornamos membros efetivos da Edward H. Angle Society of Orthodontists - Midwest. Jim é um dos membros mais ativos, sempre procurando romper fronteiras com trabalhos novos. Nestes mais de 30 anos, eu o vi sendo agraciado com todos os prêmios e honrarias existentes no campo da Ortodontia. Conhecendo sua capacidade e persistência, tenho certeza de que, se no futuro forem instituídos outros prêmios, Jim estará lá para, com todo mérito, conquistá-los. É afortunado por possuir uma família que o apoia e incentiva: sua mulher Charlene, que o acompanha em todas as viagens, e Laurie, sua filha e colega, hoje sócia em sua clínica. -

Deciduous Dentition Normal Occlusion
Normal occlusion: Deciduous dentition Early Treatment ♦ OB: Moderate to Shallow ♦ OJ: 3mm Columbia University ♦ Molar occlusion: Flush terminal plane School of Dental and Oral Surgery ♦ Buccal OJ: Positive all around Dr. Shany Park 2006 Normal occlusion: Early Treatment Deciduous dentition ♦ Preventive Orthodontic treatment ♦ Spacing: ♦ Interceptive orthodontic treatment – Generalized spacing ♦ Phase I treatment – Primate Spacing Normal Occlusion: Normal Occlusion: Deciduous dentition Early Mixed dentition ♦ Age: 2 ½ to 5 ½ years old ♦ OB: Shallow ♦ OJ: Shallow ♦ Molar Occlusion: – Mesial step or Flush terminal will shift to Cl I molar occlusion 1 Normal Occlusion: Abnormal Occlusion Early Mixed dentition ♦ No Primate spaces ♦ Diastema (ugly duckling stage) ♦ Mild crowding is accepted Normal Occlusion: Abnormal Occlusion Early Mixed dentition ♦ Lee way space: – Maxilla: 1.5 mm each side – Mandible: 2.5 mm each side Normal Occlusion: Abnormal Occlusion Early Mixed dentition 2 Abnormal Occlusion Abnormal Occlusion Abnormal Occlusion Early Treatment: Benefits ♦ Guide growth ♦ Reduce chance of extraction or surgery ♦ Reduce phase II treatment time ♦ Esthetics Abnormal Occlusion When do we treat early? ♦ Functional problems ♦ Higher chance for Trauma ♦ Space Management ♦ Esthetics 3 Increased susceptibility to Functional Problems Trauma ♦ Crossbites ♦ Severe Class II – Functional shift – Increased OJ •Anterior – Trauma to maxillary central incisors • Lateral – Constriction of maxilla • Narrow maxilla • Narrow smile Functional Problems Space