Expert Panel Discussion on Atherectomy and Vessel Prep
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

TAXUS® Express2™ and TAXUS EXPRESS2 ATOM™ Paclitaxel-Eluting Coronary Stent System Layer
6.4 Carcinogenicity, Genotoxicity, and Reproductive Toxicology ............5 Table 9.6.7 HORIZONS AMI Secondary Endpoints by Gender ........16 6.5 Pregnancy ....................................................................................................5 Table 9.6.8 HORIZONS AMI Clinical Endpoints, All TAXUS 2012-06 6.6 Lactation ........................................................................................................5 Express® Male and Female Patients at 30 Days, 1 Year, 2 Years 90776901-01 < EN > and 3 Years (Stent ITT Population) ........................................................16 7 OVERVIEW OF CLINICAL STUDIES ....................................................................5 9.7 Pooled Results of the TAXUS SR stent versus BMS (TAXUS I, II-SR, 7.1 TAXUS Clinical Trials ...................................................................................5 IV, and V de novo) .............................................................................................16 ® 2™ Table 7.1 TAXUS Slow-Release Formulation Trials ..............................6 Table 9.7.1 TAXUS SR ITT Patients Disposition Table (N=2793; TAXUS Express 7.2 ARRIVE Clinical Registry .............................................................................6 TAXUS I, II-SR, IV, and V de novo) .........................................................16 8 ADVERSE EVENTS ................................................................................................6 Figure 9.7.1 Efficacy – Target Vessel Revascularization (TVR) in and -

TAXUS™ Liberte™ Paclitaxel-Eluting Coronary Stent
TAXUS® Express2 ™ Paclitaxel-Eluting Coronary Stent System TAXUS® Liberté® Paclitaxel-Eluting Coronary Stent System A Patient’s Guide Table of Contents Coronary Artery Disease ........................................................................................................... 2 Who Is at Risk? .................................................................................................................. 3 Diagnosis of Coronary Artery Disease ................................................................................ 3 Treatment of Coronary Artery Disease ...................................................................................... 3 Angioplasty ......................................................................................................................... 4 Coronary Artery Stents ....................................................................................................... 4 Restenosis ........................................................................................................................... 5 Your Drug-Eluting Stent ........................................................................................................... 7 Drug-Eluting Stents ........................................................................................................... 7 The Express® Stent and Liberté® Stent Platforms for the TAXUS® Stent ............................ 7 The Polymer Coating on the TAXUS Stent ....................................................................... 8 The Drug That Is -

View Annual Report
2007 ANNUAL REPORT Profile of a Global Leader • One of the world’s largest medical device companies, with $8.357 billion in sales • Sales in more than 100 countries • Portfolio of approximately 13,000 products, many with #1 positions • A global leader in cardiovascular medicine $8,357 $7,821 • #1 worldwide in drug-eluting stent market • 24 million products shipped $6,283 • More than 13,800 patents issued worldwide $5,624 • More than $1 billion invested in R&D A Better Future. LEARN HOW WE’RE BUILDING IT. • 37 manufacturing, distribution and technology centers worldwide $3,476 $2,842 $2,919 $2,664 $2,673 $2,234 $1,831 $1,551 $1,191 $449 $315 $380 92 93 94 95 96 97 98 99 00 01 02 03 04 05 06 07 Revenue in millions | Years Boston Scientific Corporation One Boston Scientific Place Natick, MA 01760-1537 508.650.8000 www.bostonscientific.com Note: Information above is accurate as of December 31, 2007. Copyright © 2008 by Boston Scientific Corporation or its affiliates. All rights reserved. BSCAR2008 32737CVR.indd 1 3/14/08 3:38:46 PM Corporate Information EXECUTIVE OFFICERS AND DIRECTORS Uwe E. Reinhardt, Ph.D. 1,3,5 ANNUAL MEETING John E. Abele Director; Professor of Economics and Public Affairs, The annual meeting for shareholders will take Director; Founder Princeton University place on Tuesday, May 6, 2008, beginning In 2007, Boston Scientifi c made signifi cant progress toward restoring sustainable and more profi table 2,6 at 10:00 a.m. at Harvard Club of Boston, 374 Donald S. -

TAXUS™ Express 2 ™ Paclitaxel-Eluting
TAXU S ® Express 2® Paclitaxel-Eluting Coronary Stent System Patient Information Guide Table of Contents Notes Coronary Artery Disease . 2 Who is at Risk? . .3 Diagnosis of Coronary Artery Disease . 3 Treatment of Coronary Artery Disease . 3 Angioplasty . 4 Coronary Artery Stents . 4 Restenosis . 5 Your Drug-Eluting Stent, the TAXUS ® Express 2® Paclitaxel-Eluting Coronary Stent System . 7 Drug-Eluting Stents . 7 The Express ® Stent Platform for the TAXUS ® Express ® Stent . 7 The Polymer Coating on the TAXUS Express Stent . 7 The Drug that is Released from the TAXUS Express Stent . 8 When should the TAXUS Express Stent NOT be Used . 8 What are the Risks & Potential Benefits of Treatment with the TAXUS Express Stent? . 9 Alternative Practices and Procedures . 11 The Angioplasty Procedure . 12 Preparation for the Procedure . 12 Angioplasty and Stent Placement Procedure . 12 Post-Treatment . 13 After the Procedure . 13 Activity . 14 Medications . 14 Follow-Up Examinations . 15 Magnetic Resonance Imaging (MRI) . 15 Frequently Asked Questions . 16 Glossary . 17 Patient Information Card . Inside Back Cover 1 Notes Coronary Artery Disease Coronary Artery Disease (CAD) is usually caused by atherosclerosis, and affects the coronary arteries that surround the heart. These coronary arteries supply blood with oxygen and other nutrients to the heart muscle to make it function properly. CAD occurs when the inner walls of the coronary arteries thicken due to a buildup of cholesterol, fatty deposits, calcium, and other elements. This material is known as plaque. As plaque develops, the vessel narrows. When the vessel narrows (for example with physical exertion or mental stress), Aorta blood flow through the vessel is reduced so less oxygen and Right Left other nutrients reach Coronary Coronary the heart muscle. -

Bsx-2020-Jpm-Presentation-Final.Pdf
Mike Mahoney Chairman and Chief Executive Officer Safe harbor for forward-looking statements This presentation contains forward-looking statements within the meaning of Section 27A of the Securities Act of 1933 and Section 21E of the Securities Exchange Act of 1934. Forward-looking statements may be identified by words like “anticipate,” “expect,” “project,” “believe,” “plan,” “estimate,” “intend” and similar words. These forward-looking statements are based on our beliefs, assumptions and estimates using information available to us at the time and are not intended to be guarantees of future events or performance. If our underlying assumptions turn out to be incorrect, or if certain risks or uncertainties materialize, actual results could differ materially from the expectations and projections expressed or implied by our forward-looking statements. Factors that may cause such differences can be found in our most recent Form 10-K and Forms 10-Q filed or to be filed with the Securities and Exchange Commission under the headings “Risk Factors” and “Safe Harbor for Forward-Looking Statements.” Accordingly, you are cautioned not to place undue reliance on any of our forward-looking statements. We disclaim any intention or obligation to publicly update or revise any forward-looking statements to reflect any change in our expectations or in events, conditions, or circumstances on which they may be based, or that may affect the likelihood that actual results will differ from those contained in the forward-looking statements. 2 Regulatory disclaimers Product Regulatory Disclaimer WATCHMAN FLX™ CE Marked. U.S.: Caution: Investigational Device. Limited by Federal (or U.S.) law to investigational use only. -
Vela Proximal Endograft System Phoenix Atherectomy System
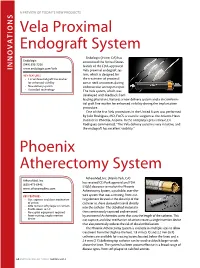
A PREVIEW OF today’s NEW PRODUCTS ONS I Vela Proximal Endograft System Endologix (Irvine, CA) has Endologix announced the United States (949) 595-7200 launch of the FDA-approved INNOVAT www.endologix.com/Vela Vela proximal endograft sys- KEY FEATURES tem, which is designed for • Circumferential graft line marker the treatment of proximal for enhanced visibility aortic neck anatomies during • New delivery system endovascular aneurysm repair. • ActiveSeal technology The Vela system, which was developed with feedback from leading physicians, features a new delivery system and a circumferen- tial graft line marker for enhanced visibility during the implantation procedure. One of the first Vela procedures in the United States was performed by Julio Rodriguez, MD, FACS, a vascular surgeon at the Arizona Heart Institute in Phoenix, Arizona. In the company’s press release, Dr. Rodriguez commented, “The Vela delivery system is very intuitive, and the endograft has excellent visibility.” Phoenix Atherectomy System AtheroMed, Inc. (Menlo Park, CA) AtheroMed, Inc. has received CE Mark approval and FDA (650) 473-6846 510(k) clearance to market the Phoenix www.atheromedinc.com Atherectomy System, a pushable, over-the- KEY FEATURES wire system that uses a rotating, front-cut- • Cut, capture, and clear mechanism ting element located at the distal tip of the of action catheter to shave diseased material directly • Able to treat soft plaque or calcium • Profile down to 5 F into the catheter. The debulked material is • No capital equipment required then continuously captured and removed • Front-cutting, single insertion by an internal Archimedes screw that runs the length of the catheter. -

ANALYSIS of AGREEMENT CONTAINING CONSENT ORDER to AID PUBLIC COMMENT in the Matter of Boston Scientific Corporation and Guidant Corporation File No
ANALYSIS OF AGREEMENT CONTAINING CONSENT ORDER TO AID PUBLIC COMMENT In the Matter of Boston Scientific Corporation and Guidant Corporation File No. 061 0046 The Federal Trade Commission (“Commission”) has accepted, subject to final approval, an Agreement Containing Consent Order (“Consent Agreement”) from Boston Scientific Corporation (“Boston Scientific”). The purpose of the proposed Consent Agreement is to remedy the anticompetitive effects that would otherwise result from Boston Scientific’s acquisition of Guidant Corporation (“Guidant”). Under the terms of the proposed Consent Agreement, Boston Scientific and Guidant are required: (a) to divest all assets (including intellectual property) related to Guidant’s vascular business to a third party, enabling that third party to make and sell drug eluting stents (“DESs”) with the Rapid Exchange (“RX”) delivery system; Percutaneous Transluminal Coronary Angioplasty (“PTCA”) balloon catheters; and coronary guidewires, and (b) to reform Boston Scientific’s contractual rights with Cameron Health, Inc. (“Cameron”) to limit Boston Scientific’s control over certain Cameron actions and the sharing of non-public information about Cameron’s Implantable Cardioverter Defibrillator (“ICD”) product. The proposed Consent Agreement has been placed on the public record for thirty days to solicit comments from interested persons. Comments received during this period will become part of the public record. After thirty days, the Commission will again review the proposed Consent Agreement and the comments received, and will decide whether it should withdraw the proposed Consent Agreement or make it final. Pursuant to an Agreement and Plan of Merger dated January 25, 2006, Boston Scientific proposes to acquire Guidant in exchange for cash and voting securities in a transaction valued at approximately $27 billion. -

Diagnosing and Treating Vascular Disease
THE CENTER FOR VASCULAR CARE AT WASHINGTON HOSPITAL CENTER Diagnosing and Treating Vascular Disease If you have symptoms of vascular disease or Peripheral Artery Disease (PAD), the best thing to do is see your physician for examination and possible testing. And, if you have the following risk factors, see your doctor to determine if you should be tested. The Center for Vascular Care at Washington Hospital Center can provide painless, risk free tests and the most complete array of treatment options for vascular disease in the region. RISK FACTORS TESTING FOR VASCULAR DISEASE FOR VASCULAR DISEASE Ankle-brachial Index: Patients with leg I Cigarette smoking artery blockage are at increased risk of I Older than age 50* heart attack and stroke. This test (ABI) is I Obesity a simple, safe, painless test for blockages. A blood pressure cuff is placed above I Diabetes the ankles and pressures are measured I Heart disease compared to arm pressures to determine I High Cholesterol the risk of cardiovascular events. It takes I High-stress lifestyle 5–10 minutes. I High blood pressure Carotid Duplex Scan: Blockage in a major I Family history of aneurysms artery increases the likelihood of a stroke. *Over age 65 if no other risk factors exist Thickening of the walls of the carotid arteries can lead to heart attack. An arterial SYMPTOMS OF VASCULAR DISEASE duplex scan is a safe, painless, highly I Leg pain that goes away with rest accu rate method of determining blockage. A sound wave device, placed lightly on the I Numbness of the legs or feet at rest skin, can tell if there is a problem. -

BSX Investor Day 2019 Full Presentation
Susan Lisa Vice President, Investor Relations Safe harbor for forward-looking statements This presentation contains forward-looking statements within the meaning of Section 27A of the Securities Act of 1933 and Section 21E of the Securities Exchange Act of 1934. Forward-looking statements may be identified by words like “anticipate,” “expect,” “project,” “believe,” “plan,” “estimate,” “intend” and similar words. These forward-looking statements are based on our beliefs, assumptions and estimates using information available to us at the time and are not intended to be guarantees of future events or performance. If our underlying assumptions turn out to be incorrect, or if certain risks or uncertainties materialize, actual results could differ materially from the expectations and projections expressed or implied by our forward-looking statements. Factors that may cause such differences can be found in our most recent Form 10-K and Forms 10-Q filed or to be filed with the Securities and Exchange Commission under the headings “Risk Factors” and “Safe Harbor for Forward-Looking Statements.” Accordingly, you are cautioned not to place undue reliance on any of our forward-looking statements. We disclaim any intention or obligation to publicly update or revise any forward-looking statements to reflect any change in our expectations or in events, conditions, or circumstances on which they may be based, or that may affect the likelihood that actual results will differ from those contained in the forward-looking statements. Regulatory disclaimers Product Regulatory Disclaimer EXALT™ Model D Not available for sale, currently pending 510(k) clearance in the US. SpyGlass™ Discover Device under development. -

2020 Annual Report Boston
BOSTON REPORT SCIENTIFIC 2020 ANNUAL 2020 Annual Report Boston Scientific Corporation 300 Boston Scientific Way Marlborough, MA 01752-1234 bostonscientific.com © 2021 Boston Scientific Corporation or its affiliates. All rights reserved. AR2020 23006_031221_10k_Cover.indd 1 3/15/21 1:02 PM Board of Directors Executive Officers Stockholder Information Nelda J. Connors 2,4 Daniel J. Brennan Stock Listing Certifications of the Chief Founder and Chief Executive Vice President Boston Scientific Corporation Executive Officer and Chief Executive Officer, Pine and Chief Financial Officer common stock is traded on the Financial Officer certifying the Grove Holdings, LLC NYSE under the symbol “BSX.” accuracy of the Company’s Arthur C. Butcher public disclosures have been 1,4 Executive Vice President Charles J. Dockendorff Transfer Agent filed with the Securities and and President, Asia Pacific Former Executive Vice Inquiries concerning the Exchange Commission as President and Chief transfer or exchange of Wendy Carruthers exhibits to the Company’s Financial Officer, shares, lost stock certificates, Senior Vice President, Annual Report on Form Covidien plc duplicate mailings, or changes Human Resources 10-K for the year ended of address should be directed Yoshiaki Fujimori 4 December 31, 2020. Jodi Euerle Eddy to the Company’s Transfer Senior Executive Advisor Senior Vice President and Agent at: Copies of these reports are of Japan, CVC Capital Chief Information and also available by directing Partners Computershare Inc. Digital Officer requests to: P.O. Box 30170 Donna A. James 2,3 Investor Relations Joseph M. Fitzgerald College Station, TX 77842-3170 Founder, President Boston Scientific Corporation Executive Vice President and Managing Director, Shareholder website: 300 Boston Scientific Way and President, Interventional Lardon & Associates, LLC www.computershare.com/ Marlborough, MA 01752-1234 Cardiology investor 508-683-4000 Edward J. -

Drug-Eluting Stents in Elderly Patients with Coronary Artery Disease (SENIOR): a Randomised Single-Blind Trial
Articles Drug-eluting stents in elderly patients with coronary artery disease (SENIOR): a randomised single-blind trial Olivier Varenne, Stéphane Cook, Georgios Sideris, Sasko Kedev, Thomas Cuisset, Didier Carrié, Thomas Hovasse, Philippe Garot, Rami El Mahmoud, Christian Spaulding, Gérard Helft, José F Diaz Fernandez, Salvatore Brugaletta, Eduardo Pinar-Bermudez, Josepa Mauri Ferre, Philippe Commeau, Emmanuel Teiger, Kris Bogaerts, Manel Sabate, Marie-Claude Morice, Peter R Sinnaeve, for the SENIOR investigators Summary Published Online Background Elderly patients regularly receive bare-metal stents (BMS) instead of drug-eluting stents (DES) to shorten November 1, 2017 http://dx.doi.org/10.1016/ the duration of double antiplatelet therapy (DAPT). The aim of this study was to compare outcomes between these S0140-6736(17)32713-7 two types of stents with a short duration of DAPT in such patients. See Online/Comment http://dx.doi.org/10.1016/ Methods In this randomised single-blind trial, we recruited patients from 44 centres in nine countries. Patients were S0140-6736(17)32803-9 eligible if they were aged 75 years or older; had stable angina, silent ischaemia, or an acute coronary syndrome; and had at Hôpital Cochin, Assistance least one coronary artery with a stenosis of at least 70% (≥50% for the left main stem) deemed eligible for percutaneous Publique—Hôpitaux de Paris, coronary intervention (PCI). Exclusion criteria were indication for myocardial revascularisation by coronary artery bypass Paris, France, and Cardiology Department, Université Paris grafting; inability to tolerate, obtain, or comply with DAPT; requirement for additional surgery; non-cardiac comorbidities Descartes, Sorbonne Paris-Cité, with a life expectancy of less than 1 year; previous haemorrhagic stroke; allergy to aspirin or P2Y12 inhibitors; contraindication Paris, France (Prof O Varenne MD); Cardiology to P2Y12 inhibitors; and silent ischaemia of less than 10% of the left myocardium with a fractional flow reserve of 0·80 or higher. -

Lower Extremity Invasive Diagnostic and Endovascular Procedures
UnitedHealthcare® Commercial Medical Policy Lower Extremity Invasive Diagnostic and Endovascular Procedures Policy Number: 2021T0602F Effective Date: July 1, 2021 Instructions for Use Table of Contents Page Related Commercial Policies Coverage Rationale ........................................................................... 1 • Pneumatic Compression Devices Documentation Requirements......................................................... 2 • Surgical and Ablative Procedures for Venous Definitions ........................................................................................... 3 Insufficiency and Varicose Veins Applicable Codes .............................................................................. 4 Description of Services ..................................................................... 5 Community Plan Policy Clinical Evidence ............................................................................... 5 • Lower Extremity Invasive Diagnostic and U.S. Food and Drug Administration ................................................ 7 Endovascular Procedures References ......................................................................................... 8 Medicare Advantage Coverage Summary Policy History/Revision Information................................................ 9 • Instructions for Use ........................................................................... 9 Cardiovascular Diagnostic Procedures Coverage Rationale Note: This policy does not apply to upper extremities. Diagnosis Lower extremity