March 2, 2021 Emergency Order Under MCL 333.2253 – Gatherings
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Copy of 2020-2021 Semi-Monthly Calendar.Xlsx
Employee Time Sheet/Leave Sheet Schedule Supervisor Approval Deadline/ Pay Period Employee Submittal Deadline Paper Leave Request Due to HR by 11:59 PM 12 Noon Pay Day Wednesday, July 1, 2020 to Wednesday, July 15, 2020 Thursday, July 16, 2020 Friday, July 17, 2020 Friday, July 31, 2020 Thursday, July 16, 2020 to Friday, July 31, 2020 Monday, August 3, 2020 Tuesday, August 4, 2020 Friday, August 14, 2020 Saturday, August 1, 2020 to Saturday, August 15, 2020 Monday, August 17, 2020 Tuesday, August 18, 2020 Monday, August 31, 2020 Sunday, August 16, 2020 to Monday, August 31, 2020 Tuesday, September 1, 2020 Wednesday, September 2, 2020 Tuesday, September 15, 2020 Tuesday, September 1, 2020 to Tuesday, September 15, 2020 Wednesday, September 16, 2020 Thursday, September 17, 2020 Wednesday, September 30, 2020 Wednesday, September 16, 2020 to Wednesday, September 30, 2020 Thursday, October 1, 2020 Friday, October 2, 2020 Thursday, October 15, 2020 Thursday, October 1, 2020 to Thursday, October 15, 2020 Friday, October 16, 2020 Monday, October 19, 2020 Friday, October 30, 2020 Friday, October 16, 2020 to Saturday, October 31, 2020 Monday, November 2, 2020 Tuesday, November 3, 2020 Friday, November 13, 2020 Sunday, November 1, 2020 to Sunday, November 15, 2020 Monday, November 16, 2020 Tuesday, November 17, 2020 Monday, November 30, 2020 Monday, November 16, 2020 to Monday, November 30, 2020 Tuesday, December 1, 2020 Wednesday, December 2, 2020 Tuesday, December 15, 2020 Tuesday, December 1, 2020 to Tuesday, December 15, 2020 Wednesday, December -

2021-2022 Custom & Standard Information Due Dates
2021-2022 CUSTOM & STANDARD INFORMATION DUE DATES Desired Cover All Desired Cover All Delivery Date Info. Due Text Due Delivery Date Info. Due Text Due May 31 No Deliveries No Deliveries July 19 April 12 May 10 June 1 February 23 March 23 July 20 April 13 May 11 June 2 February 24 March 24 July 21 April 14 May 12 June 3 February 25 March 25 July 22 April 15 May 13 June 4 February 26 March 26 July 23 April 16 May 14 June 7 March 1 March 29 July 26 April 19 May 17 June 8 March 2 March 30 July 27 April 20 May 18 June 9 March 3 March 31 July 28 April 21 May 19 June 10 March 4 April 1 July 29 April 22 May 20 June 11 March 5 April 2 July 30 April 23 May 21 June 14 March 8 April 5 August 2 April 26 May 24 June 15 March 9 April 6 August 3 April 27 May 25 June 16 March 10 April 7 August 4 April 28 May 26 June 17 March 11 April 8 August 5 April 29 May 27 June 18 March 12 April 9 August 6 April 30 May 28 June 21 March 15 April 12 August 9 May 3 May 28 June 22 March 16 April 13 August 10 May 4 June 1 June 23 March 17 April 14 August 11 May 5 June 2 June 24 March 18 April 15 August 12 May 6 June 3 June 25 March 19 April 16 August 13 May 7 June 4 June 28 March 22 April 19 August 16 May 10 June 7 June 29 March 23 April 20 August 17 May 11 June 8 June 30 March 24 April 21 August 18 May 12 June 9 July 1 March 25 April 22 August 19 May 13 June 10 July 2 March 26 April 23 August 20 May 14 June 11 July 5 March 29 April 26 August 23 May 17 June 14 July 6 March 30 April 27 August 24 May 18 June 15 July 7 March 31 April 28 August 25 May 19 June 16 July 8 April 1 April 29 August 26 May 20 June 17 July 9 April 2 April 30 August 27 May 21 June 18 July 12 April 5 May 3 August 30 May 24 June 21 July 13 April 6 May 4 August 31 May 25 June 22 July 14 April 7 May 5 September 1 May 26 June 23 July 15 April 8 May 6 September 2 May 27 June 24 July 16 April 9 May 7 September 3 May 28 June 25. -

COVID-19 Latin America
COVID-19 Measures in Effect in Latin America March 27, 2020 Below is a brief overview, country by country, of some of the measures adopted in response to the COVID-19 virus in Latin America. This is not meant to be an all-encompassing document of every measure taken in each country, but rather a quick snapshot of the situation today. As with everywhere in the world, this is a fluid situation and measures will likely change over the coming days and weeks. ARGENTINA The Argentine government announced a total lockdown of the country starting at midnight on March 19 through March 31. Everything has been shut down except for security, health and grocery services. Ciruclation is restricted both on national routes and within cities across the country. Transfers will only be allowed for exceptional reasons, such as to guarantee essential production, supply, health services and all essential services. All repatriation efforts have been cancelled. All borders are closed to both Argentine and foreign citizens. All shows have been cancelled and no groupings over 50 people are permitted. Schools have been cancelled through the end of March but commerce remains open. With the aim of guaranteeing supplies and controlling the abuse regarding the increase of prices during the health emergency, the Ministry of Productive Development ordered that starting March 20 and for the next 30 days, the prices of basic food, beverages, personal hygiene items and cleaning supplies will be maintained, at the price they were being sold on March 6, before the COVID-19 outbreak. This measure will be applied to supermarkets, retail and wholesale supermarkets, mini-markets, warehouses and self-service markets. -

2021 7 Day Working Days Calendar
2021 7 Day Working Days Calendar The Working Day Calendar is used to compute the estimated completion date of a contract. To use the calendar, find the start date of the contract, add the working days to the number of the calendar date (a number from 1 to 1000), and subtract 1, find that calculated number in the calendar and that will be the completion date of the contract Date Number of the Calendar Date Friday, January 1, 2021 133 Saturday, January 2, 2021 134 Sunday, January 3, 2021 135 Monday, January 4, 2021 136 Tuesday, January 5, 2021 137 Wednesday, January 6, 2021 138 Thursday, January 7, 2021 139 Friday, January 8, 2021 140 Saturday, January 9, 2021 141 Sunday, January 10, 2021 142 Monday, January 11, 2021 143 Tuesday, January 12, 2021 144 Wednesday, January 13, 2021 145 Thursday, January 14, 2021 146 Friday, January 15, 2021 147 Saturday, January 16, 2021 148 Sunday, January 17, 2021 149 Monday, January 18, 2021 150 Tuesday, January 19, 2021 151 Wednesday, January 20, 2021 152 Thursday, January 21, 2021 153 Friday, January 22, 2021 154 Saturday, January 23, 2021 155 Sunday, January 24, 2021 156 Monday, January 25, 2021 157 Tuesday, January 26, 2021 158 Wednesday, January 27, 2021 159 Thursday, January 28, 2021 160 Friday, January 29, 2021 161 Saturday, January 30, 2021 162 Sunday, January 31, 2021 163 Monday, February 1, 2021 164 Tuesday, February 2, 2021 165 Wednesday, February 3, 2021 166 Thursday, February 4, 2021 167 Date Number of the Calendar Date Friday, February 5, 2021 168 Saturday, February 6, 2021 169 Sunday, February -
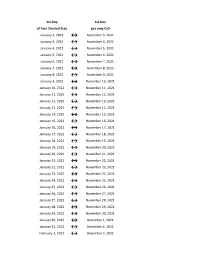
Flex Dates.Xlsx
1st Day 1st Day of Your Desired Stay you may Call January 2, 2022 ↔ November 3, 2021 January 3, 2022 ↔ November 4, 2021 January 4, 2022 ↔ November 5, 2021 January 5, 2022 ↔ November 6, 2021 January 6, 2022 ↔ November 7, 2021 January 7, 2022 ↔ November 8, 2021 January 8, 2022 ↔ November 9, 2021 January 9, 2022 ↔ November 10, 2021 January 10, 2022 ↔ November 11, 2021 January 11, 2022 ↔ November 12, 2021 January 12, 2022 ↔ November 13, 2021 January 13, 2022 ↔ November 14, 2021 January 14, 2022 ↔ November 15, 2021 January 15, 2022 ↔ November 16, 2021 January 16, 2022 ↔ November 17, 2021 January 17, 2022 ↔ November 18, 2021 January 18, 2022 ↔ November 19, 2021 January 19, 2022 ↔ November 20, 2021 January 20, 2022 ↔ November 21, 2021 January 21, 2022 ↔ November 22, 2021 January 22, 2022 ↔ November 23, 2021 January 23, 2022 ↔ November 24, 2021 January 24, 2022 ↔ November 25, 2021 January 25, 2022 ↔ November 26, 2021 January 26, 2022 ↔ November 27, 2021 January 27, 2022 ↔ November 28, 2021 January 28, 2022 ↔ November 29, 2021 January 29, 2022 ↔ November 30, 2021 January 30, 2022 ↔ December 1, 2021 January 31, 2022 ↔ December 2, 2021 February 1, 2022 ↔ December 3, 2021 1st Day 1st Day of Your Desired Stay you may Call February 2, 2022 ↔ December 4, 2021 February 3, 2022 ↔ December 5, 2021 February 4, 2022 ↔ December 6, 2021 February 5, 2022 ↔ December 7, 2021 February 6, 2022 ↔ December 8, 2021 February 7, 2022 ↔ December 9, 2021 February 8, 2022 ↔ December 10, 2021 February 9, 2022 ↔ December 11, 2021 February 10, 2022 ↔ December 12, 2021 February -
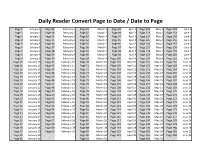
Daily Reader Convert Page to Date / Date to Page
Daily Reader Convert Page to Date / Date to Page Page 1 January 1 Page 32 February 1 Page 61 March 1 Page 92 April 1 Page 122 May 1 Page 153 June 1 Page 2 January 2 Page 33 February 2 Page 62 March 2 Page 93 April 2 Page 123 May 2 Page 154 June 2 Page 3 January 3 Page 34 February 3 Page 63 March 3 Page 94 April 3 Page 124 May 3 Page 155 June 3 Page 4 January 4 Page 35 February 4 Page 64 March 4 Page 95 April 4 Page 125 May 4 Page 156 June 4 Page 5 January 5 Page 36 February 5 Page 65 March 5 Page 96 April 5 Page 126 May 5 Page 157 June 5 Page 6 January 6 Page 37 February 6 Page 66 March 6 Page 97 April 6 Page 127 May 6 Page 158 June 6 Page 7 January 7 Page 38 February 7 Page 67 March 7 Page 98 April 7 Page 128 May 7 Page 159 June 7 Page 8 January 8 Page 39 February 8 Page 68 March 8 Page 99 April 8 Page 129 May 8 Page 160 June 8 Page 9 January 9 Page 40 February 9 Page 69 March 9 Page 100 April 9 Page 130 May 9 Page 161 June 9 Page 10 January 10 Page 41 February 10 Page 70 March 10 Page 101 April 10 Page 131 May 10 Page 162 June 10 Page 11 January 11 Page 42 February 11 Page 71 March 11 Page 102 April 11 Page 132 May 11 Page 163 June 11 Page 12 January 12 Page 43 February 12 Page 72 March 12 Page 103 April 12 Page 133 May 12 Page 164 June 12 Page 13 January 13 Page 44 February 13 Page 73 March 13 Page 104 April 13 Page 134 May 13 Page 165 June 13 Page 14 January 14 Page 45 February 14 Page 74 March 14 Page 105 April 14 Page 135 May 14 Page 166 June 14 Page 15 January 15 Page 46 February 15 Page 75 March 15 Page 106 April 15 Page 136 May -
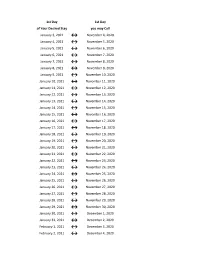
Flex Dates.Xlsx
1st Day 1st Day of Your Desired Stay you may Call January 3, 2021 ↔ November 4, 2020 January 4, 2021 ↔ November 5, 2020 January 5, 2021 ↔ November 6, 2020 January 6, 2021 ↔ November 7, 2020 January 7, 2021 ↔ November 8, 2020 January 8, 2021 ↔ November 9, 2020 January 9, 2021 ↔ November 10, 2020 January 10, 2021 ↔ November 11, 2020 January 11, 2021 ↔ November 12, 2020 January 12, 2021 ↔ November 13, 2020 January 13, 2021 ↔ November 14, 2020 January 14, 2021 ↔ November 15, 2020 January 15, 2021 ↔ November 16, 2020 January 16, 2021 ↔ November 17, 2020 January 17, 2021 ↔ November 18, 2020 January 18, 2021 ↔ November 19, 2020 January 19, 2021 ↔ November 20, 2020 January 20, 2021 ↔ November 21, 2020 January 21, 2021 ↔ November 22, 2020 January 22, 2021 ↔ November 23, 2020 January 23, 2021 ↔ November 24, 2020 January 24, 2021 ↔ November 25, 2020 January 25, 2021 ↔ November 26, 2020 January 26, 2021 ↔ November 27, 2020 January 27, 2021 ↔ November 28, 2020 January 28, 2021 ↔ November 29, 2020 January 29, 2021 ↔ November 30, 2020 January 30, 2021 ↔ December 1, 2020 January 31, 2021 ↔ December 2, 2020 February 1, 2021 ↔ December 3, 2020 February 2, 2021 ↔ December 4, 2020 1st Day 1st Day of Your Desired Stay you may Call February 3, 2021 ↔ December 5, 2020 February 4, 2021 ↔ December 6, 2020 February 5, 2021 ↔ December 7, 2020 February 6, 2021 ↔ December 8, 2020 February 7, 2021 ↔ December 9, 2020 February 8, 2021 ↔ December 10, 2020 February 9, 2021 ↔ December 11, 2020 February 10, 2021 ↔ December 12, 2020 February 11, 2021 ↔ December 13, 2020 -

BILLING CYCLE SCHEDULE Department of Procurement, Disbursements & Contract Services 1135 Old Main 600 Lincoln Avenue Charleston, IL 61920
Eastern Illinois University BILLING CYCLE SCHEDULE Department of Procurement, Disbursements & Contract Services 1135 Old Main 600 Lincoln Avenue Charleston, IL 61920 Billing Cycle Beginning Date Billing Cycle Ending Date June 26, 2018 July 25, 2018 Tuesday Wednesday July 26, 2018 August 24, 2018 Thursday Friday August 26, 2018 September 25, 2018 Sunday Tuesday September 26, 2018 October 25, 2018 Wednesday Thursday October 26, 2018 November 26, 2018 Friday Monday November 27, 2018 December 26, 2018 Tuesday Wednesday December 27, 2018 January 25, 2019 Thursday Friday January 26, 2019 February 25, 2019 Saturday Monday February 26, 2019 March 25, 2019 Tuesday Monday March 26, 2019 April 25, 2019 Tuesday Thursday April 26, 2019 May 24, 2019 Friday Friday May 26, 2019 June 25, 2019 Sunday Tuesday June 26, 2019 July 25, 2019 Wednesday Thursday Revised 2/2/18 1 Transactions with a Post Date of: Must be Reviewed Upload to Banner & Approved by: July 1, 2018 – July 6, 2018 July 12, 2018 July 13, 2018 Thursday Friday July 7, 2018 – July 13, 2018 July 19, 2018 July 20, 2018 Thursday Friday July 14, 2018 – July 20, 2018 July 26, 2018 July 27, 2018 Thursday Friday July 21, 2018 – July 27, 2018 August 2, 2018 August 3, 2018 Thursday Friday July 28, 2018 – August 3, 2018 August 9, 2018 August 10, 2018 Thursday Friday August 4, 2018 – August 10, 2018 August 16, 2018 August 17, 2018 Thursday Friday August 11, 2018 – August 17, 2018 August 23, 2018 August 24, 2018 Thursday Friday August 18, 2018 – August 24, 2018 August 30, 2018 August 31, 2018 Thursday -

Julian Date Cheat Sheet for Regular Years
Date Code Cheat Sheet For Regular Years Day of Year Calendar Date 1 January 1 2 January 2 3 January 3 4 January 4 5 January 5 6 January 6 7 January 7 8 January 8 9 January 9 10 January 10 11 January 11 12 January 12 13 January 13 14 January 14 15 January 15 16 January 16 17 January 17 18 January 18 19 January 19 20 January 20 21 January 21 22 January 22 23 January 23 24 January 24 25 January 25 26 January 26 27 January 27 28 January 28 29 January 29 30 January 30 31 January 31 32 February 1 33 February 2 34 February 3 35 February 4 36 February 5 37 February 6 38 February 7 39 February 8 40 February 9 41 February 10 42 February 11 43 February 12 44 February 13 45 February 14 46 February 15 47 February 16 48 February 17 49 February 18 50 February 19 51 February 20 52 February 21 53 February 22 54 February 23 55 February 24 56 February 25 57 February 26 58 February 27 59 February 28 60 March 1 61 March 2 62 March 3 63 March 4 64 March 5 65 March 6 66 March 7 67 March 8 68 March 9 69 March 10 70 March 11 71 March 12 72 March 13 73 March 14 74 March 15 75 March 16 76 March 17 77 March 18 78 March 19 79 March 20 80 March 21 81 March 22 82 March 23 83 March 24 84 March 25 85 March 26 86 March 27 87 March 28 88 March 29 89 March 30 90 March 31 91 April 1 92 April 2 93 April 3 94 April 4 95 April 5 96 April 6 97 April 7 98 April 8 99 April 9 100 April 10 101 April 11 102 April 12 103 April 13 104 April 14 105 April 15 106 April 16 107 April 17 108 April 18 109 April 19 110 April 20 111 April 21 112 April 22 113 April 23 114 April 24 115 April -
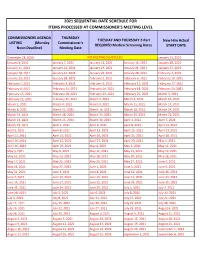
2021 Sequential Date List
2021 SEQUENTIAL DATE SCHEDULE FOR ITEMS PROCESSED AT COMMISSIONER'S MEETING LEVEL COMMISSIONERS AGENDA THURSDAY TUESDAY AND THURSDAY 2-Part New Hire Actual LISTING (Monday Commissioner's REQUIRED Medical Screening Dates START DATE Noon Deadline) Meeting Date December 28, 2020 NO MEETING SCHEDULED January 13, 2021 January 4, 2021 January 7, 2021 January 12, 2021 January 14, 2021 January 20, 2021 January 11, 2021 January 14, 2021 January 19, 2021 January 21, 2021 January 27, 2021 January 18, 2021 January 21, 2021 January 26, 2021 January 28, 2021 February 3, 2021 January 25, 2021 January 28, 2021 February 2, 2021 February 4, 2021 February 10, 2021 February 1, 2021 February 4, 2021 February 9, 2021 February 11, 2021 February 17, 2021 February 8, 2021 February 11, 2021 February 16, 2021 February 18, 2021 February 24, 2021 February 15, 2021 February 18, 2021 February 23, 2021 February 25, 2021 March 3, 2021 February 22, 2021 February 25, 2021 March 2, 2021 March 4, 2021 March 10, 2021 March 1, 2021 March 4, 2021 March 9, 2021 March 11, 2021 March 17, 2021 March 8, 2021 March 11, 2021 March 16, 2021 March 18, 2021 March 24, 2021 March 15, 2021 March 18, 2021 March 23, 2021 March 25, 2021 March 31, 2021 March 22, 2021 March 25, 2021 March 30, 2021 April 1, 2021 April 7, 2021 March 29, 2021 April 1, 2021 April 6, 2021 April 8, 2021 April 14, 2021 April 5, 2021 April 8, 2021 April 13, 2021 April 15, 2021 April 21, 2021 April 12, 2021 April 15, 2021 April 20, 2021 April 22, 2021 April 28, 2021 April 19, 2021 April 22, 2021 April 27, 2021 April -

2021 Rezoning Review Schedule
City of Waukee | 2021 ZONING AMENDMENT REVIEW SCHEDULE APPLICATION STAFF APPLICANT PUBLIC P & Z P & Z COUNCIL COUNCIL COUNCIL COUNCIL DUE COMMENTS REVISIONS by HEARING SUBMITTAL MEETING SUBMITTAL MEETING MEETING MEETING by 5:00 p.m. SENT 5:00 p.m. DATE SET by 5:00 p.m. 6:00 p.m. by 5:00 p.m. 5:30 p.m. 5:30 p.m. 5:30 p.m. 5:30 p.m. [1st Consider.] [2nd Consider.] [3rd Consider.] (TUES.) (TUES.) (TUES.) (MON.) (THUR.) (TUES.) (WED.) (MON.) (MON.) (MON.) November 17 November 24 December 1 December 7 December 17 December 22 December 30 January 4 January 18 February 1 December 8 December 15 December 22 December 21 January 7 January 12 January 13 January 18 February 1 *February 16* December 22 December 29 January 5 January 4 January 21 January 26 January 27 February 1 *February 16* March 1 January 5 January 12 January 19 January 18 February 4 February 9 February 10 *February 16* March 1 March 15 January 19 January 26 February 2 February 1 February 18 February 23 February 24 March 1 March 15 April 5 February 2 February 9 February 16 *February 16* March 4 March 9 March 10 March 15 April 5 April 19 February 16 February 23 March 2 March 1 March 18 March 23 March 31 April 5 April 19 May 3 March 2 March 9 March 16 March 15 April 8 April 13 April 14 April 19 May 3 May 17 March 16 March 23 March 30 April 5 April 22 April 27 April 28 May 3 May 17 June 7 March 30 April 6 April 13 April 19 May 6 May 11 May 12 May 17 June 7 June 21 April 13 April 20 April 27 May 3 May 20 May 25 June 2 June 7 June 21 *July 6* April 27 May 4 May 11 May 17 June 3 June 8 June -

Date of Close Contact Exposure
Date of Close Contact Exposure 7 days 10 days 14 days Monday, November 16, 2020 Tuesday, November 24, 2020 Friday, November 27, 2020 Tuesday, December 1, 2020 Tuesday, November 17, 2020 Wednesday, November 25, 2020 Saturday, November 28, 2020 Wednesday, December 2, 2020 Wednesday, November 18, 2020 Thursday, November 26, 2020 Sunday, November 29, 2020 Thursday, December 3, 2020 Thursday, November 19, 2020 Friday, November 27, 2020 Monday, November 30, 2020 Friday, December 4, 2020 Friday, November 20, 2020 Saturday, November 28, 2020 Tuesday, December 1, 2020 Saturday, December 5, 2020 Saturday, November 21, 2020 Sunday, November 29, 2020 Wednesday, December 2, 2020 Sunday, December 6, 2020 Sunday, November 22, 2020 Monday, November 30, 2020 Thursday, December 3, 2020 Monday, December 7, 2020 Monday, November 23, 2020 Tuesday, December 1, 2020 Friday, December 4, 2020 Tuesday, December 8, 2020 Tuesday, November 24, 2020 Wednesday, December 2, 2020 Saturday, December 5, 2020 Wednesday, December 9, 2020 Wednesday, November 25, 2020 Thursday, December 3, 2020 Sunday, December 6, 2020 Thursday, December 10, 2020 Thursday, November 26, 2020 Friday, December 4, 2020 Monday, December 7, 2020 Friday, December 11, 2020 Friday, November 27, 2020 Saturday, December 5, 2020 Tuesday, December 8, 2020 Saturday, December 12, 2020 Saturday, November 28, 2020 Sunday, December 6, 2020 Wednesday, December 9, 2020 Sunday, December 13, 2020 Sunday, November 29, 2020 Monday, December 7, 2020 Thursday, December 10, 2020 Monday, December 14, 2020 Monday, November