Health Care ’99 a Guide to Health Care in Alberta
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Road Construction Further Divides Highway 43
June 27, 2005 Road construction further divides Highway 43 Edmonton... Another 50 kilometres of four-lane road on Highway 43 will open to traffic by the end of this year's construction season, beginning with a 14-kilometre stretch that will open this month. Highway 43 forms the northwest leg of Alberta's North-South Trade Corridor and runs 432 kilometres from its junction with Highway 16 west of Edmonton to Grande Prairie. The Alberta government will invest approximately $52 million in the highway in 2005, bringing the total investment in Highway 43 to $450 million over the past six years. The federal government is also investing $29 million in the highway under the Strategic Highway Infrastructure Program. "The twinning of Highway 43 will improve the safety and efficiency of this important North American trade corridor," said Deputy Prime Minister and Minister of Public Safety and Emergency Preparedness, Anne McLellan on behalf of Jean-C. Lapierre, federal Minister of Transport. "It demonstrates the Government of Canada's commitment to working with its provincial partners to strengthen highway infrastructure across the country." A 14-kilometre segment of newly twinned highway will open to traffic by the end of June, between Cherhill and Glenevis, followed by another 36 kilometres by the end of the 2005 construction season. That will leave only 56 kilometres of two-lane road along the 432-kilometre highway. Work will continue this year on four-laning these remaining 56 kilometres and will be complete by the fall of 2007. "Continuing to twin Highway 43 is a major step toward completing the North-South Trade Corridor," said Dr. -

Latest Twinned Section on Highway 43 Improves Safety for Motorists Divided Roadway Between Green Court and Sangudo Opens to Traffic
Managing growth pressures September 20, 2007 Latest twinned section on Highway 43 improves safety for motorists Divided roadway between Green Court and Sangudo opens to traffic Mayerthorpe... Motorists travelling between Green Court and Sangudo will enjoy 18.5 kilometres of newly divided highway, as the province officially opens the latest twinned section on Highway 43 at a cost of $22.3 million. “Twinning Highway 43 between Edmonton and Grande Prairie is nearly complete, providing a safer and more efficient highway for one of Alberta’s major economic corridors,” said Luke Ouellette, Minister of Infrastructure and Transportation. “By twinning this important stretch of the North-South Trade Corridor, Alberta is investing in the economic future of the province.” Highway 43 forms the northwest leg of Alberta’s North-South Trade Corridor and runs 432 kilometres from its junction with Highway 16 west of Edmonton to Grande Prairie. The Alberta government has invested $1.3 billion to develop the North-South Trade Corridor since 1998, including $566 million since 1998 to twin Highway 43. “As a long-time supporter of the twinning of Highway 43, I’m pleased this very busy section of highway will be safer for motorists and will help support economic development throughout the region,” said George VanderBurg, MLA for Whitecourt-Ste. Anne. Two additional Highway 43 projects are currently underway. Final paving of 34 kilometres of previously twinned Highway 43 between Sangudo and Glenevis is expected to be finished by the end of September at a cost of $9.5 million. An additional 35 kilometres of Highway 43 twinning will also open to traffic later this fall, weather permitting, between Asplund Creek and Iosegun Lake at a cost of $46 million. -
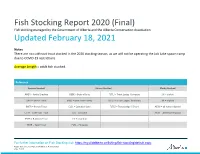
Fish Stocking Report, 2020 (Final)
Fish Stocking Report 2020 (Final) Fish stocking managed by the Government of Alberta and the Alberta Conservation Association Updated February 18, 2021 Notes There are no cutthroat trout stocked in the 2020 stocking season, as we will not be operating the Job Lake spawn camp due to COVID-19 restrictions. Average Length = adult fish stocked. Reference Species Stocked Strains Stocked Ploidy Stocked ARGR = Arctic Grayling BEBE = Beity x Beity TLTLJ = Trout Lodge / Jumpers 2N = diploid BKTR = Brook Trout BRBE = Bow River x Beity TLTLK = Trout Lodge / Kamloops 3N = triploid BNTR = Brown Trout CLCL = Campbell Lake TLTLS = Trout Lodge / Silvers AF2N = all female diploid CTTR = Cutthroat Trout JLJL = Job Lake AF3N = all female triploid RNTR = Rainbow Trout LYLY = Lyndon TGTR = Tiger Trout PLPL = Pit Lakes For further information on Fish Stocking visit: https://mywildalberta.ca/fishing/fish-stocking/default.aspx ©2021 Government of Alberta | Published: February 2021 Page 1 of 24 Waterbody Waterbody ATS Species Strain Genotype Average Number Stocking Official Name Common Name Length Stocked Date (2020) ALFORD LAKE SW4-36-8-W5 RNTR Campbell Lake 3N 18 3000 18-May-20 BEAR POND NW36-14-4-W5 RNTR Trout Lodge/Jumpers AF3N 19.7 750 22-Jun-20 BEAUVAIS LAKE SW29-5-1-W5 RNTR Trout Lodge/Jumpers AF3N 16.3 23000 11-May-20 BEAVER LAKE NE16-35-6-W5 RNTR Trout Lodge/Jumpers AF3N 21.3 2500 21-May-20 BEAVER LAKE NE16-35-6-W5 TGTR Beitty/Bow River 3N 16.9 500 02-Sep-20 BEAVER LAKE NE16-35-6-W5 TGTR Beitty/Bow River 3N 20 500 02-Sep-20 BEAVER MINES LAKE NE11-5-3-W5 -
Final-Alberta-Loss-Factors-For-2009
2009 Loss Factors TABLE OF CONTENTS 1.0 PURPOSE ................................................................................................. 3 2.0 INTRODUCTION ....................................................................................... 3 3.0 2009 LOSS FACTORS.............................................................................. 3 4.0 2009 AND 2008 LOSS FACTORS CALCULATION ................................. 6 5.0 2009 OVERALL LOSS FACTOR RESULTS ............................................ 8 6.0 LOSS FACTOR MAP ................................................................................ 9 7.0 CONCLUSION........................................................................................... 9 APPENDIX I. CASE COMPARISON .................................................................... 10 ii Alberta Electric System Operator 2009 Loss Factors 1.0 Purpose The purpose of this document is to present the 2009 loss factors complete with a brief explanation of changes. A loss factor map is included. The loss factors published in this document will be effective from January 01, 2009 to December 31, 2009. 2.0 Introduction The AESO has completed the final analysis of 2009 loss factors and the results are attached. The analysis includes the application of the 2009 Generic Stacking Order (GSO) results published earlier this summer and the 2009 Base Cases published in October on the AESO web site. Both the GSO and the Base Cases have been updated during the course of the final calculations and reposted. The requirements -
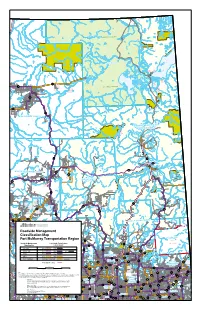
Roadside Management Classification
I.R. I.R. 196A I.R. 196G 196D I.R. 225 I.R. I.R. I.R. 196B 196 196C I.R. 196F I.R. 196E I.R. 223 WOOD BUFFALO NATIONAL PARK I.R. Colin-Cornwall Lakes I.R. 224 Wildland 196H Provincial Park I.R. 196I La Butte Creek Wildland P. Park Ca ribou Mountains Wildland Provincial Park Fidler-Greywillow Wildland P. Park I.R. 222 I.R. 221 I.R. I.R. 219 Fidler-Greywillow 220 Wildland P. Park Fort Chipewyan I.R. 218 58 I.R. 5 I.R. I.R. 207 8 163B 201A I.R . I.R. I.R. 201B 164A I.R. 215 163A I.R. WOOD BU I.R. 164 FFALO NATIONAL PARK 201 I.R Fo . I.R. 162 rt Vermilion 163 I.R. 173B I.R. 201C I.R. I.R. 201D 217 I.R. 201E 697 La Crete Maybelle Wildland P. Park Richardson River 697 Dunes Wildland I.R. P. Park 173A I.R. 201F 88 I.R. 173 87 I.R. 201G I.R. 173C Marguerite River Wildland Provincial Park Birch Mountains Wildland Provincial Park I.R. 174A I.R. I.R. 174B 174C Marguerite River Wildland I.R. Provincial Park 174D Fort MacKay I.R. 174 88 63 I.R. 237 686 Whitemud Falls Wildland FORT Provincial Park McMURRAY 686 Saprae Creek I.R. 226 686 I.R. I.R 686 I.R. 227 I.R. 228 235 Red Earth 175 Cre Grand Rapids ek Wildland Provincial Park Gipsy Lake I.R. Wildland 986 238 986 Cadotte Grand Rapids Provincial Park Lake Wildland Gregoire Lake Little Buffalo Provincial Park P. -

Location and History Profile Cardston County
Location and History Profile Created on 9/24/2021 12:49:39PM Cardston County Municipal Code: 0053 Location Description View Location Map (url to the pdf location map) Twp Rge Mer Longitude Latitude 4 24 W4 113°10' 49°17' Urban municipalities within the municipal boundary Town of Cardston Town of Magrath Village of Glenwood Village of Hill Spring Hamlets/urban service areas within the municipal boundary Aetna Beazer Carway Del Bonita Kimball Leavitt Mountain View Spring Coulee Welling Welling Station Woolford Incorporation History Municipal Boundary Document Search (url to search results page of Annexation PDF's) Status: Municipal District Effective Date: January 01, 2000 Authority: Order in Council 504/99 Authority Date: December 08, 1999 Gazette: Dec 31, 1999, p. 2442 Comments: The name of the Municipal District of Cardston No. 6 was changed to Cardston County. Status: Municipal District Effective Date: January 01, 1954 Authority: Mininsterial Order Authority Date: January 01, 1954 Gazette: Dec 31, 1953, p. 2085 Comments: Formed the Municipal District of Cardston No. 6 by merging part of Municipal District of Sugar City No. 5 and part of the Municipal District of Cochrane No. 6. Status: Municipal District Effective Date: January 01, 1946 Authority: Ministerial Order Authority Date: Gazette: Dec 15, 1945, p. 1266 Comments: Erected as the Municipal District of Cochrane No. 6 by merging the Municipal District of Cochrane No. 7 and Improvement District No. 6 into one new Municipal District. Status: Improvement District Effective Date: April 01, 1945 Authority: Ministerial Order Authority Date: February 15, 1945 Gazette: Feb 28, 1945, p. 177 Comments: Improvement Districts No. -
Published Local Histories
ALBERTA HISTORIES Published Local Histories assembled by the Friends of Geographical Names Society as part of a Local History Mapping Project (in 1995) May 1999 ALBERTA LOCAL HISTORIES Alphabetical Listing of Local Histories by Book Title 100 Years Between the Rivers: A History of Glenwood, includes: Acme, Ardlebank, Bancroft, Berkeley, Hartley & Standoff — May Archibald, Helen Bircham, Davis, Delft, Gobert, Greenacres, Kia Ora, Leavitt, and Brenda Ferris, e , published by: Lilydale, Lorne, Selkirk, Simcoe, Sterlingville, Glenwood Historical Society [1984] FGN#587, Acres and Empires: A History of the Municipal District of CPL-F, PAA-T Rocky View No. 44 — Tracey Read , published by: includes: Glenwood, Hartley, Hillspring, Lone Municipal District of Rocky View No. 44 [1989] Rock, Mountain View, Wood, FGN#394, CPL-T, PAA-T 49ers [The], Stories of the Early Settlers — Margaret V. includes: Airdrie, Balzac, Beiseker, Bottrell, Bragg Green , published by: Thomasville Community Club Creek, Chestermere Lake, Cochrane, Conrich, [1967] FGN#225, CPL-F, PAA-T Crossfield, Dalemead, Dalroy, Delacour, Glenbow, includes: Kinella, Kinnaird, Thomasville, Indus, Irricana, Kathyrn, Keoma, Langdon, Madden, 50 Golden Years— Bonnyville, Alta — Bonnyville Mitford, Sampsontown, Shepard, Tribune , published by: Bonnyville Tribune [1957] Across the Smoky — Winnie Moore & Fran Moore, ed. , FGN#102, CPL-F, PAA-T published by: Debolt & District Pioneer Museum includes: Bonnyville, Moose Lake, Onion Lake, Society [1978] FGN#10, CPL-T, PAA-T 60 Years: Hilda’s Heritage, -

2003 Report on the Environment
Report on the Environment 2003 Message to the Citizens of St. Albert In the last year, the City of St. Albert has had some significant accomplishments: Why should we report on the environment? If the City of St. Albert is to achieve sustainability, then the corporation of the City of St. Albert and the citizens of the City of St. • We have adapted a system for information dissemination and the delegation of Albert must be in a position to accurately measure environmental performance, and regular environmental responsibilities among members of City Council by establishing the reporting on the state of the environment is the best way to track corporate performance. Environmental Advisory Committee. • Council adopted a set of corporate environmental policies and will delegate the This is the City of St. Albert’s first annual report on the environment. We have taken some implementation of the policies to the Senior Leadership Team of the City. significant steps toward establishing a reporting system that will allow St. Albertan’s to have • City Council authorized the Senior Leadership Team to proceed with the development of a a clear understanding about what this corporation is doing to protect the environment of St. pilot environmental management system conforming to a set of international standards. The Albert. City’s Transit Department has been selected to lead the way in this initiative. Some key initiatives undertaken this year include: Hopefully, in the years ahead, readers will be in a position to judge whether our efforts to • Commencement of a city-wide Stormwater Management Master Plan maintain and enhance the environmental conditions have been effective. -

Guide and Resource
Alberta Prenatal Care Documentation Guide and Resource for Prenatal Care Providers Acknowledgements The Alberta Perinatal Health Disclaimer Although significant effort has been Program (APHP) acknowledges the contribution made to ensure the accuracy of information of APHP committee members, individual presented in these and supporting materials, practitioners, Toward Optimized Practice (TOP), neither the authors nor any other parties make any the Southern Alberta Child and Youth Health presentations or warranties (express, implied or Network (SACYHN), the Physician Office Support statutory) as to accuracy, reliability or completeness Program (POSP), Alberta Health and Wellness of the information. In no event will the authors or (AHW) and Service Alberta in the development of any other parties be responsible or liable for any the Alberta Prenatal Record (APR) and supporting errors or any consequences arising from the use documentation. or misuse of these materials or the information in these materials. These materials should not be considered a substitute for clinical judgment and The Healthy Mother, Healthy Baby Questionnaire clinical advice. (HMHB-Q) and the User Guide were produced by the Southern Alberta Child and Youth Health Permission is granted for the reproduction of Network (SACYHN) in collaboration with the these materials solely for non-commercial and Chinook, Calgary, Palliser, and David Thompson educational purposes, no part of this publication Health Regions, and Treaty No. 7. The Alberta may be reproduced, stored in a retrieval system, or Perinatal Health Program and Toward Optimized transmitted in any form or by any means, without the Practice collaborated in the development. prior written permission of the Fund Administrator for the Alberta Prenatal Health Program. -

Distribution Alberta, North West Territories, British Columbia And
D IS TRIBUTI ON ALBERTA N ORTH E TERRITORI S BRITI S , W S T E , H COLUMB IA AN D YUKON TERRITORY CONTAINING m 1 . of Ofli The na es the Post ces alphabetically arranged . Th m o 2 . e f of C na es the Postal Car Routes , Sections Postal ar Routes or Distribution m for Offices through which atter the several offices should pass . m of m 3 . The na es the Offices to which the atter is forwarded by the Railway Mail Clerks m i di . or Distributing Offi ces when not ailed direct . (D rect Mails are in cated by dotted lines ) o 4 . The names f the Mail Routes by whi ch the offices are served when not situated on a o m line of Railway . Wh en an office is served by two or more routes the hours f departure fro the several terminal points are given . -O . m 5 ffices . Nixie List closed, na es changed — 6 . Offices in Northwest Territories Page 137 . INSTRUCTIONS for w i m l f 1 . Matter any office hich is suppl ed by ore than one route shou d be orwarded by m the one by which it will ost speedily reach its destination . i m 2 . Wh en any doubt ex sts as to the proper railway route by which atter should be f m c . orwarded, application should be ade to the District Director or Superintendent, Postal Servi e O m 3 . fli c es hi newly established, and offi ces to w ch new na es have been given , should be written in the List of Offices having the same initial letter . -

2017 Municipal Codes
2017 Municipal Codes Updated December 22, 2017 Municipal Services Branch 17th Floor Commerce Place 10155 - 102 Street Edmonton, Alberta T5J 4L4 Phone: 780-427-2225 Fax: 780-420-1016 E-mail: [email protected] 2017 MUNICIPAL CHANGES STATUS CHANGES: 0315 - The Village of Thorsby became the Town of Thorsby (effective January 1, 2017). NAME CHANGES: 0315- The Town of Thorsby (effective January 1, 2017) from Village of Thorsby. AMALGAMATED: FORMATIONS: DISSOLVED: 0038 –The Village of Botha dissolved and became part of the County of Stettler (effective September 1, 2017). 0352 –The Village of Willingdon dissolved and became part of the County of Two Hills (effective September 1, 2017). CODE NUMBERS RESERVED: 4737 Capital Region Board 0522 Metis Settlements General Council 0524 R.M. of Brittania (Sask.) 0462 Townsite of Redwood Meadows 5284 Calgary Regional Partnership STATUS CODES: 01 Cities (18)* 15 Hamlet & Urban Services Areas (396) 09 Specialized Municipalities (5) 20 Services Commissions (71) 06 Municipal Districts (64) 25 First Nations (52) 02 Towns (108) 26 Indian Reserves (138) 03 Villages (87) 50 Local Government Associations (22) 04 Summer Villages (51) 60 Emergency Districts (12) 07 Improvement Districts (8) 98 Reserved Codes (5) 08 Special Areas (3) 11 Metis Settlements (8) * (Includes Lloydminster) December 22, 2017 Page 1 of 13 CITIES CODE CITIES CODE NO. NO. Airdrie 0003 Brooks 0043 Calgary 0046 Camrose 0048 Chestermere 0356 Cold Lake 0525 Edmonton 0098 Fort Saskatchewan 0117 Grande Prairie 0132 Lacombe 0194 Leduc 0200 Lethbridge 0203 Lloydminster* 0206 Medicine Hat 0217 Red Deer 0262 Spruce Grove 0291 St. Albert 0292 Wetaskiwin 0347 *Alberta only SPECIALIZED MUNICIPALITY CODE SPECIALIZED MUNICIPALITY CODE NO. -

An Integrated Geological and Geophysical Analysis of the Hydrocarbon Potential of the Spring Coulee, Alberta Area
Hydrocarbon Potential of Spring Coulee An integrated geological and geophysical analysis of the hydrocarbon potential of the Spring Coulee, Alberta area Lauren A. Ostridge and Robert R. Stewart ABSTRACT The University of Calgary holds the mineral rights to two sections of land in southern Alberta (sections 14 and 23, township 4, range 23 west of the fourth meridian) in the Spring Coulee Area. CREWES was given the opportunity to analyze the hydrocarbon potential of the area. The geological potential of the area was examined, and it was determined that there is a potential to find oil in the structurally high areas of the Madison zone, of Mississippian age, with the possibility of a potential of finding hydrocarbons in younger sand and shale zones, along with deeper carbonates. In January 2008, CREWES, in conjunction with ARAM, Outsource and CGGVeritas shot a 2D-3C seismic survey over the area, looking mainly at the Madison Zone. It was discovered that there are at least two structural highs in the Mississippian zone and more work is being done to model this reservoir. From the information at hand, we have chosen two potential well locations in the south-central portion of section 23 and the north-northwestern side of section 14. INTRODUCTION In July of 2004, the University of Calgary hired a new land administrator. Upon searching for the titles for the University of Calgary, he discovered that there were two sections of mineral rights owned by ‘The Board of Directors of the University of Calgary’. The land is sections 14 and 23, township 4, range 23, west of the fourth meridian.