The Good, the Bad, the Thyroid Gland
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Subacute Thyroiditis with Non-Toxic Hyperfunctioning Thyroid Nodules
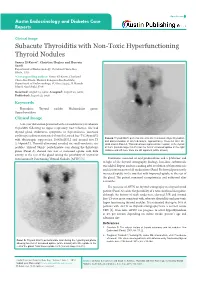
Open Access Austin Endocrinology and Diabetes Case Reports Clinical Image Subacute Thyroiditis with Non-Toxic Hyperfunctioning Thyroid Nodules Samer El-Kaissi*, Christine Hughes and Hussein Saadi Department of Endocrinology, Cleveland Clinic Abu Dhabi, UAE *Corresponding author: Samer El-Kaissi, Cleveland Clinic Abu Dhabi, Medical Subspecialties Institute, Department of Endocrinology, PO Box 112412, Al Maryah Island, Abu Dhabi, UAE Received: August 15, 2016; Accepted: August 22, 2016; Published: August 23, 2016 Keywords Thyroiditis; Thyroid nodule; Multinodular goitre; Hyperthyroidism Clinical Image A 46-year old woman presented with a 4-week history of subacute Thyroiditis following an upper respiratory tract infection. She had thyroid gland tenderness, symptoms of thyrotoxicosis, increased erythrocyte sedimentation rate [45mm/hr], raised free-T4 [29pmol/L] Panel B: Thyroid 99mTc pertechnetate scan after resolution of hyperthyroidism with thyrotropin suppression [0.005mIU/L] and normal free-T3 and discontinuation of all medications, approximately 10-weeks after the [5.64pmol/L]. Thyroid ultrasound revealed six small-moderate size initial scan in Panel A. This scan shows improved tracer uptake in the thyroid nodules. Thyroid 99mTc pertechnetate scan during the thyrotoxic at 0.6% (normal range 0.2-3%) but the foci of increased uptake in the right phase (Panel A) showed two foci of increased uptake with little midzone and left lower zone are still apparent (white arrows). activity in the rest of the gland raising the possibility of coexistent Autonomously Functioning Thyroid Nodules [AFTN] [1]. Treatment consisted of oral prednisolone and a β-blocker and in light of the thyroid scintigraphy findings, low-dose carbimazole was added. Repeat nuclear scanning after resolution of thyrotoxicosis and discontinuation of all medications (Panel B) showed persistently increased uptake in the two foci with improved uptake in the rest of the gland. -

The Subacute Thyroiditis, Since Its First Description by De Quervain (1904), Has Been Reported Under Many Synonyms
Endocrinol. Japon. 1964, 11 (2), 119~138 STUDIES ON SUBACUTE THYROIDITIS SHOZO SAITO Department of Radiology, School of Medicine, Gunma University, Maebashi The subacute thyroiditis, since its first description by de Quervain (1904), has been reported under many synonyms. Terms given with reference to the histo- logic features of this disease include "pseudotuberculous thyroiditis", "granulo- matous thyroiditis", "gaint-cell thyroiditis", "de Quervain's thyroiditis", "struma granulomatosa" or "struma fibrosa, giant cell variant". The clinical findings have given rise to such names as" acute and subacute nonsuppurative thyroiditis", "acute noninfectious thyroiditis"and"subacute thyroiditis" . In recent writings, the disease is most commonly referred to as subacute thyroiditis. Later, de Quervain and Giordanengo (1936) collected reports of 54 cases of the disease, appearing in the literature since de Quervain's original description, and clearly distinguished it from other forms of thyroiditis. Several years ago, the disease had been considered relatively rare, but with recent advance in endocrinology, more attentions have been drawn by it, and more reports published on it. For the past six years, the author has treated 51 cases of subacute thyroiditis, and obtained findings of interest, which are outlined in this paper. METHODS OF EXAMINATION The disease was confirmed by Silverman's needle biopsy (Crile and Rumsey, 1950; Crile and Hazard, 1951) of the thyroid in 36 of them, and the others were diagnosed by typical clinical symptoms, characteristic results of thyroidal function test and accelerated red cell sedimentation rate and its clinical course. Thyroid function test Basal metabolic rate (BMR) was examined by Knipping's method (normal range•}15%), and serum protein-bound iodine (PBI) by modification of Barker's method (Barker and Humphrey, 1950). -

Hypothyroidism
Hypothyroidism Alejandro Diaz, MD,*† Elizabeth G. Lipman Diaz, PhD, CPNP‡ *Miami Children’s Hospital, Miami, FL †The Herbert Wertheim College of Medicine, Florida International University, Miami, FL ‡University of Miami School of Nursing and Health Studies, Miami, FL Educational Gap Congenital hypothyroidism is one the most common causes of preventable intellectual disability. Awareness that not all cases are detected by the newborn screening is important, particularly because early diagnosis and treatment are essential in preserving cognitive abilities. Objectives After completing this article, readers should be able to: 1. Identify the causes of congenital and acquired hypothyroidism in infants and children. 2. Interpret an abnormal newborn screening result and understand indications for further evaluation and treatment. 3. Recognize clinical signs and symptoms of hypothyroidism. 4. Understand the importance of early diagnosis and treatment of congenital hypothyroidism. 5. Understand the presentation, diagnostic process, treatment, and prognosis of Hashimoto thyroiditis. 6. Differentiate thyroid-binding globulin deficiency from central hypothyroidism. AUTHOR DISCLOSURE Drs Diaz and Lipman Diaz have disclosed no financial relationships 7. Identify sick euthyroid syndrome and other causes of abnormal thyroid relevant to this article. This commentary does function test results. not contain a discussion of an unapproved/ investigative use of a commercial product/ device. ABBREVIATIONS CH congenital hypothyroidism BACKGROUND FT3 free triiodothyronine FT4 free thyroxine The thyroid gland produces hormones that have important functions related to energy HT Hashimoto thyroiditis metabolism, control of body temperature, growth, bone development, and maturation LT4 levothyroxine of the central nervous system, among other metabolic processes throughout the body. rT3 reverse triiodothyronine The thyroid gland develops from the endodermal pharynx. -

Hyperthyroidism
135 Review Article Hyperthyroidism Amanda R. Doubleday, Rebecca S. Sippel Division of Endocrine Surgery, Department of Surgery, University of Wisconsin School of Medicine and Public Health, Madison, WI, USA Contributions: (I) Conception and design: All authors; (II) Administrative support: None; (III) Provision of study materials or patients: None; (IV) Collection and assembly of data: All authors; (V) Data analysis and interpretation: All authors; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors. Correspondence to: Rebecca S. Sippel, MD. Division of Endocrine Surgery, Department of Surgery, University of Wisconsin School of Medicine and Public Health, Clinical Science Center-H4/722, Box 7375, 600 Highland Ave, Madison, WI 53792-3284, USA. Email: [email protected]; Amanda R. Doubleday, DO, MBA. Division of Endocrine Surgery, Department of Surgery, University of Wisconsin School of Medicine and Public Health, K4/739 Clinical Science Center, 600 Highland Ave, Madison, WI 53792-3284, USA. Email: [email protected]. Abstract: Hyperthyroidism is a condition where the thyroid gland produces and secretes inappropriately high amounts of thyroid hormone which can lead to thyrotoxicosis. The prevalence of hyperthyroidism in the United States is approximately 1.2%. There are many different causes of hyperthyroidism, and the most common causes include Graves’ disease (GD), toxic multinodular goiter and toxic adenoma. The diagnosis can be made based on clinical findings and confirmed with biochemical tests and imaging techniques including ultrasound and radioactive iodine uptake scans. This condition impacts many different systems of the body including the integument, musculoskeletal, immune, ophthalmic, reproductive, gastrointestinal and cardiovascular systems. It is important to recognize common cardiovascular manifestations such as hypertension and tachycardia and to treat these patients with beta blockers. -

Thyroiditis: an Integrated Approach LORI B
Thyroiditis: An Integrated Approach LORI B. SWEENEY, MD, Virginia Commonwealth University Health System, Richmond, Virginia CHRISTOPHER STEWART, MD, Bayne-Jones Army Community Hospital, Fort Polk, Louisiana DAVID Y. GAITONDE, MD, Dwight D. Eisenhower Army Medical Center, Fort Gordon, Georgia Thyroiditis is a general term that encompasses several clinical disorders characterized by inflammation of the thyroid gland. The most common is Hashimoto thyroiditis; patients typically present with a nontender goiter, hypothyroid- ism, and an elevated thyroid peroxidase antibody level. Treatment with levothyroxine ameliorates the hypothyroid- ism and may reduce goiter size. Postpartum thyroiditis is transient or persistent thyroid dysfunction that occurs within one year of childbirth, miscarriage, or medical abortion. Release of preformed thyroid hormone into the bloodstream may result in hyperthyroidism. This may be followed by transient or permanent hypothyroidism as a result of depletion of thyroid hormone stores and destruction of thyroid hormone–producing cells. Patients should be monitored for changes in thyroid function. Beta blockers can treat symptoms in the initial hyperthyroid phase; in the subsequent hypothyroid phase, levothyroxine should be considered in women with a serum thyroid-stimulating hormone level greater than 10 mIU per L, or in women with a thyroid-stimulating hormone level of 4 to 10 mIU per L who are symptomatic or desire fertility. Subacute thyroiditis is a transient thyrotoxic state characterized by anterior neck pain, suppressed thyroid-stimulating hormone, and low radioactive iodine uptake on thyroid scanning. Many cases of subacute thyroiditis follow an upper respiratory viral illness, which is thought to trigger an inflammatory destruction of thyroid follicles. In most cases, the thyroid gland spontaneously resumes normal thyroid hormone production after several months. -

Disease/Medical Condition
Disease/Medical Condition HYPOTHYROIDISM Date of Publication: January 27, 2017 (also known as “underactive thyroid disease”; includes congenital hypothyroidism [also known as “neonatal hypothyroidism”] and Hashimoto’s thyroiditis [also known as “autoimmune thyroiditis”]; may manifest as “cretinism” [if onsets during fetal or early life; also known as “congenital myxedema”] or “myxedema” [if onset occurs in older children and adults]) Is the initiation of non-invasive dental hygiene procedures* contra-indicated? No. ◼ Is medical consult advised? – Yes, if previously undiagnosed hypothyroidism or enlarged (or shrunken) thyroid gland is suspected1, in which case the patient/client should see his/her primary care physician. Detection early in childhood can prevent permanent intellectual impairment. – Yes, if previously diagnosed hypothyroidism is suspected to be undermedicated (with manifest signs/symptoms of hypothyroidism) or overmedicated (with manifest signs/symptoms of hyperthyroidism2), in which case the patient/client should see his/her primary care physician or endocrinologist. Major stress or illness sometimes necessitates an increase in prescribed thyroid hormone. Is the initiation of invasive dental hygiene procedures contra-indicated?** Possibly, depending on the certainty of diagnosis and level of control. ◼ Is medical consult advised? – See above. ◼ Is medical clearance required? – Yes, if undiagnosed or severe hypothyroidism is suspected. ◼ Is antibiotic prophylaxis required? – No. ◼ Is postponing treatment advised? – Yes, if undiagnosed hypothyroidism is suspected (necessitating medical assessment/management) or severe hypothyroidism is suspected (necessitating urgent medical assessment/management in order to avoid risk of myxedema coma). In general, the patient/client with mild symptoms of untreated hypothyroidism is not in danger when receiving dental hygiene therapy, and the well managed (euthyroid) patient/client requires no special regard. -

Management of Graves Disease:€€A Review
Clinical Review & Education Review Management of Graves Disease A Review Henry B. Burch, MD; David S. Cooper, MD Author Audio Interview at IMPORTANCE Graves disease is the most common cause of persistent hyperthyroidism in adults. jama.com Approximately 3% of women and 0.5% of men will develop Graves disease during their lifetime. Supplemental content at jama.com OBSERVATIONS We searched PubMed and the Cochrane database for English-language studies CME Quiz at published from June 2000 through October 5, 2015. Thirteen randomized clinical trials, 5 sys- jamanetworkcme.com and tematic reviews and meta-analyses, and 52 observational studies were included in this review. CME Questions page 2559 Patients with Graves disease may be treated with antithyroid drugs, radioactive iodine (RAI), or surgery (near-total thyroidectomy). The optimal approach depends on patient preference, geog- raphy, and clinical factors. A 12- to 18-month course of antithyroid drugs may lead to a remission in approximately 50% of patients but can cause potentially significant (albeit rare) adverse reac- tions, including agranulocytosis and hepatotoxicity. Adverse reactions typically occur within the first 90 days of therapy. Treating Graves disease with RAI and surgery result in gland destruction or removal, necessitating life-long levothyroxine replacement. Use of RAI has also been associ- ated with the development or worsening of thyroid eye disease in approximately 15% to 20% of patients. Surgery is favored in patients with concomitant suspicious or malignant thyroid nodules, coexisting hyperparathyroidism, and in patients with large goiters or moderate to severe thyroid Author Affiliations: Endocrinology eye disease who cannot be treated using antithyroid drugs. -

Myopathy in Acute Hypothyroidism
Postgrad Med J: first published as 10.1136/pgmj.63.742.661 on 1 August 1987. Downloaded from Postgraduate Medical Journal (1987) 63, 661-663 Clinical Reports Myopathy in acute hypothyroidism A.W.C. Kung, J.T.C. Ma, Y.L. Yu, C.C.L. Wang, E.K.W. Woo, K.S.L. Lam, C.Y. Huang and R.T.T. Yeung Department ofMedicine, University ofHong Kong, Queen Mary Hospital, Pokfulam Road, Hong Kong. Summary: Hypothyroid myopathy has so far been reported in long standing cases ofhypothyroidism. We describe two adult patients with myopathy associated with acute transient hypothyroidism. Both presented with severe muscle aches and cramps, stiffness and spasms. Muscle enzymes were markedly elevated and electromyography in one patient showed myopathic features. Histological changes were absent in muscle biopsy, probably because of the short duration of metabolic disturbance. The myopathy subsided promptly when the hypothyroid state was reversed. Introduction Hypothyroid myopathy has been described in patients however no muscle weakness or symptoms of hypo- with long-standing hypothyroidism.' 3 We report two thyroidism. She had no preceding viral infection. Chinese patients with muscle involvement in acute Examination revealed that the goitre had decreased in copyright. transient hypothyroidism, who improved after rever- size and she was clinically euthyroid. Motor and sal of the hypothyroid state, sensory functions were completely normal. Investigation showed a T4 of 44nmol/l, triiodo- thyronine (T3) 1.2 nmol/I (normal 0.77-2.97 nmol/1), Case reports and TSH 5.1 AIU/ml (normal up to 7). The serum creatine kinase level was 11,940ILmol/min.l (normal Case I 5-165) and the lactic dehydrogenase was 397;Lmol/ min.l (normal 130-275), and glutamic-oxalacetic A 42 year old woman presented at another hospital transaminase was 120limol/min.l (normal 28-32). -

Newborn Screening for Congenital Hypothyroidism: Recommended Guidelines
American Academy of Pediatrics American Thyroid Association Newborn Screening for Congenital Hypothyroidism: Recommended Guidelines During the past decade newborn screening for of identifying newborns with hyperthyroxinemia congenital hypothyroidism has become an impor- (1:20,000 to 40,000 newborns). tant health activity in most developed countries. On the other hand, this approach will miss in- These screening programs have not only benefited fants who have normal T4 values but elevated TSH patients and their families but also have produced values. Such infants are relatively commonplace in new information about the epidemiology, patho- European programs where initial screening is done physiology, diagnosis, and treatment of thyroid dis- by measurement of TSH. To identify such infants, ease in infancy and childhood. During this period the T4 concentration cutoff (for TSH testing) must of implementation and growth of the screening be increased well into the normal range. programs, a variety of issues and questions arose. Some of these have been resolved, and some have TSH not. The point has now been reached where colla- A majority of European and Japanese programs tion of the combined experiences of the North favor screening by means of primary TSH mea- American programs can address these issues. The surements, supplemented by T4 determinations on reader should understand that what follows reflects those infants with elevated TSH values. With this 0 current opinion and may require changes when the approach, infants with thyroxine-binding globulin results of the next decade of screening are reviewed. deficiency, hypo- or hyperthyroxinemia, or hypo- thalamic-pituitary hypothyroidism will be missed. SCREENING METHOD Until further advances are made in the state of the art of screening, the choice ofthe method should Thyroxine (T4) and Thyroid-Stimulating Hormone be based on the experience of the program, needs (TSH) of the population, and availability of resources. -

Hashimoto Thyroiditis
Hashimoto thyroiditis Description Hashimoto thyroiditis is a condition that affects the function of the thyroid, which is a butterfly-shaped gland in the lower neck. The thyroid makes hormones that help regulate a wide variety of critical body functions. For example, thyroid hormones influence growth and development, body temperature, heart rate, menstrual cycles, and weight. Hashimoto thyroiditis is a form of chronic inflammation that can damage the thyroid, reducing its ability to produce hormones. One of the first signs of Hashimoto thyroiditis is an enlargement of the thyroid called a goiter. Depending on its size, the enlarged thyroid can cause the neck to look swollen and may interfere with breathing and swallowing. As damage to the thyroid continues, the gland can shrink over a period of years and the goiter may eventually disappear. Other signs and symptoms resulting from an underactive thyroid can include excessive tiredness (fatigue), weight gain or difficulty losing weight, hair that is thin and dry, a slow heart rate, joint or muscle pain, and constipation. People with this condition may also have a pale, puffy face and feel cold even when others around them are warm. Affected women can have heavy or irregular menstrual periods and difficulty conceiving a child ( impaired fertility). Difficulty concentrating and depression can also be signs of a shortage of thyroid hormones. Hashimoto thyroiditis usually appears in mid-adulthood, although it can occur earlier or later in life. Its signs and symptoms tend to develop gradually over months or years. Frequency Hashimoto thyroiditis affects 1 to 2 percent of people in the United States. -

SUBACUTE THYROIDITIS by SELWYN TAYLOR, M.CH., F.R.C.S
Postgrad Med J: first published as 10.1136/pgmj.33.381.327 on 1 July 1957. Downloaded from 327 SUBACUTE THYROIDITIS By SELWYN TAYLOR, M.CH., F.R.C.S. Surgeon, King's College Hospital, Belgrave Hospitalfor Children, and Hammersmith Hospital; Lecturer in Surgery, Postgraduate Medical School of London The term ' thyroiditis ' implies inflammation of to become much more common in that particular the thyroid gland, but by long usage it has come clinic. I had never seen an example before I950, to be used for a number of conditions in which but saw six in the next three years and pro- infection or trauma play apparently no part. Sub- gressively more each year since then. The con- acute thyroiditis is the title given to a condition dition is much commoner in women than men in which was first clearly described by de Quervain the ratio of about six to one. It has not yet been in I904 and which has been rediscovered, or re- reported in a child and is commonest in the fourth described, on a number of occasions since then, and fifth decades, although I have seen it in a with the result that it now has a multiplicity of student teacher of twenty-one. In our own series different names: granulomatous thyroiditis, giant- there was a history of a pre-existing goitre in 50 cell thyroiditis, pseudotuberculous thyroiditis, per cent. of the patients. The incidence, compared creeping thyroiditis, struma granulomatosa, acute with that of Hashimoto's thyroiditis and Riedel's non-infectious thyroiditis, acute non-suppurative thyroiditis, varies widely in different clinics, but thyroiditis and de Quervain's thyroiditis. -

Hypothyroidism: Mimicker of Common Complaints Matthew C
Emerg Med Clin N Am 23 (2005) 649–667 Hypothyroidism: Mimicker of Common Complaints Matthew C. Tews, DOa, Sid M. Shah, MD, FACEPb,*, Ved V. Gossain, MD, FACP, FACEPc aCollege of Osteopathic Medicine, Emergency Medicine Residency Program, Michigan State University–Lansing, P.O. Box 30480, Lansing, MI 48909, USA bMichigan State University, Attending Physician Emergency Medicine, Ingham Regional Medical, Center 401 W. Greenlawn Avenue, Lansing, MI 48910, USA cDivision of Endocrinology, Department of Medicine, Michigan State University, Lansing, MI 48909, USA Patients with hypothyroidism may present with vague symptoms such as fatigue, arthralgias, myalgias, muscle cramps, headaches, and ‘‘not feeling well.’’ These are also among the more common complaints encountered by the emergency physicians. The disease spectrum of hypothyroidism ranges from an asymptomatic, subclinical condition to the rare, life-threatening myxedema coma, and thus can be a challenging diagnosis to make. A progressive and chronic disease, hypothyroidism results from diminished thyroid hormone production. It slows metabolic functions in every organ system in the body. Commonly, clinical presentation of hypothyroidism can be confused with effects of aging in the elderly, musculoskeletal or a psychiatric illness such as depression in the younger patients. Spontaneously occurring hypothyroidism is relatively common, with prevalence between 1% to 2%, and is 10 times more common in women than in men [1]. The probability of developing spontaneous hypothyroidism increases with age, with women having a mean age at diagnosis of around 60 years [2]. A recent survey showed that 9.5% out of nearly 26,000 visitors to a statewide health fair in Colorado had elevated circulating thyroid stimulating hormone (TSH) levels, indicating underlying hypothyroidism [3].