Practice Guidelines for Central Venous Access a Report by the American Society of Anesthesiologists Task Force on Central Venous Access
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Central Venous Access with Accelerated Seldinger Technique Versus Modified Seldinger Technique
Central Venous Access with Accelerated Seldinger Technique versus Modified Seldinger Technique L A N E THAUT , D O , CAPT , M C , USAF SAN ANTONIO MILITARY MEDICAL CENTER CO- AUTHORS: WELLS WEYMOUTH, MD, DANIEL RESCHKE, MD, BRANDEN HUNSAKER,MD Disclosures Expired POWERWAND™ combination device kits were donated by Access Scientific for the express purpose to be used in this study; however, no other contributions were made. We approached Access Scientific to obtain the devices to conduct this study. No financial relationship with Access Scientific. Background Techniques Research and Outcomes Questions Background Air Force SAMMC San Antonio, TX Level 1 Trauma Center 85,000+ patients annually Central Access Common Procedure Approximately 8% of hospitalized patients Multiple indications Large volume fluid or blood product resuscitation Administration of central acting medications Multiple medications simultaneously Trans venous pacing Difficult peripheral access Quick Story What if there was a simpler/quicker way? Intra-osseous? Complications Slower Flow Rate Labs Traditional Central Line Multiple steps/parts Midlines Usually used for extended dwelling lines. Self contained, all in one device. Equivalent and sometimes superior flow rate. Question Will the use of combination devices (midline/POWERWAND™) and the associated accelerated technique reduce the time of CVC placement? VS What is Accelerated Seldinger Technique? Needle, guidewire, dilator, and sheath into one. The device needle is inserted into the target vein under ultrasound guidance and a flash is observed The internal guidewire is then advanced into the vein and snapped into the needle hub. Dilator collar is turned and the dilator and sheath are advanced The dilator hub is disengaged from the needle hub, and the guidewire, dilator, and needle are all removed as a single unit. -

59 Arterial Catheter Insertion (Assist), Care, and Removal 509
PROCEDURE Arterial Catheter Insertion 59 (Assist), Care, and Removal Hillary Crumlett and Alex Johnson PURPOSE: Arterial catheters are used for continuous monitoring of blood pressure, assessment of cardiovascular effects of vasoactive drugs, and frequent arterial blood gas and laboratory sampling. In addition, arterial catheters provide access to blood samples that support the diagnostics related to oxygen, carbon dioxide, and bicarbonate levels (oxygenation, ventilation, and acid-base status). PREREQUISITE NURSING aortic valve closes, marking the end of ventricular systole. KNOWLEDGE The closure of the aortic valve produces a small rebound wave that creates a notch known as the dicrotic notch. The • Knowledge of the anatomy and physiology of the vascu- descending limb of the curve (diastolic downslope) repre- lature and adjacent structures is needed. sents diastole and is characterized by a long declining • Knowledge of the principles of hemodynamic monitoring pressure wave, during which the aortic wall recoils and is necessary. propels blood into the arterial network. The diastolic pres- • Understanding of the principles of aseptic technique is sure is measured as the lowest point of the diastolic needed. downslope, which should be less than 80 mm Hg in • Conditions that warrant the use of arterial pressure moni- adults. 21 toring include patients with the following: • The difference between the systolic and diastolic pres- ❖ Frequent blood sampling: sures is the pulse pressure, with a normal value of about Respiratory conditions requiring arterial blood gas 40 mm Hg. monitoring (oxygenation, ventilation, acid-base • Arterial pressure is determined by the relationship between status) blood fl ow through the vessels (cardiac output) and the Bleeding, actual or potential resistance of the vessel walls (systemic vascular resis- Electrolyte or glycemic abnormalities, actual or tance). -

Sepsis: a Guide for Patients & Relatives
SEPSIS: A GUIDE FOR PATIENTS & RELATIVES CONTENTS ABOUT SEPSIS ABOUT SEPSIS: INTRODUCTION P3 What is sepsis? In the UK, at least 150,000* people each year suffer from serious P4 Why does sepsis happen? sepsis. Worldwide it is thought that 3 in a 1000 people get sepsis P4 Different types of sepsis P4 Who is at risk of getting sepsis? each year, which means that 18 million people are affected. P5 What sepsis does to your body Sepsis can move from a mild illness to a serious one very quickly, TREATMENT OF SEPSIS which is very frightening for patients and their relatives. P7 Why did I need to go to the Critical Care Unit? This booklet is for patients and relatives and it explains sepsis P8 What treatment might I have had? and its causes, the treatment needed and what might help after P9 What other help might I have received in the Critical Care Unit? having sepsis. It has been written by the UK Sepsis Trust, a charity P10 How might I have felt in the Critical Care Unit? which supports people who have had sepsis and campaigns to P11 How long might I stay in the Critical Care Unit and hospital? raise awareness of the illness, in collaboration with ICU steps. P11 Moving to a general ward and The Outreach Team/Patient at Risk Team If a patient cannot read this booklet for him or herself, it may be helpful for AFTER SEPSIS relatives to read it. This will help them to understand what the patient is going through and they will be more able to support them as they recover. -
Reducing Arterial Catheters
Reducing the Risk of Catheter-Related Bloodstream Infections: Peripheral Arterial Catheters Amy Bardin Spencer, EdD(c), MS, RRT, VA-BC™ Manager, Clinical Marketing – Strategic Programs – Teleflex Russ Olmsted, MPH, CIC Director, Infection Prevention & Control, Trinity Health Paid consultant, Ethicon, BIOPATCH products Disclosure • This presentation reflects the technique, approaches and opinions of the individual presenters. This Ethicon sponsored presentation is not intended to be used as a training guide. The steps demonstrated may not be the complete steps of the procedure. Before using any medical device, review all relevant package inserts with particular attention to the indications, contraindications, warnings and precautions, and steps for use of the device(s). • Amy Bardin Spencer and Russ Olmsted are compensated by and presenting on behalf of Ethicon and must present information in accordance with applicable regulatory requirements. 0.8% of arterial lines become infected Maki DG et al., Mayo Clinic Proc 2006;81:1159-1171. Are You Placing Arterial Catheters? 16,438 per day 6,000,000 arterial catheters 680 every hour Maki DG et al., Mayo Clinic Proc 2006;81:1159-1171. 131 per day 48,000 arterial catheter-related bloodstream infections 5 patients every hour Maki DG et al., Mayo Clinic Proc 2006;81:1159-1171. Risk Factors • Lack of insertion compliance • No surveillance procedure • No bundle specific to arterial device insertion or maintenance • Multiple inserters with variations in skill set Maki DG et al., Mayo Clinic Proc 2006;81:1159-1171. -

Arterial Line
Arterial Line An arterial line is a thin catheter inserted into an artery. Arterial line placement is a common procedure in various critical care settings. It is most commonly used in intensive care medicine and anesthesia to monitor blood pressure directly and in real time (rather than by intermittent and indirect measurement, like a blood pressure cuff) and to obtain samples for arterial blood gas analysis. There are specific insertion sites, trained personnel and procedures for arterial lines. There are also specific techniques for drawing a blood sample from an A-Line or arterial line. An arterial line is usually inserted into the radial artery in the wrist, but can also be inserted into the brachial artery at the elbow, into the femoral artery in the groin, into the dorsalis pedis artery in the foot, or into the ulnar artery in the wrist. In both adults and children, the most common site of cannulation is the radial artery, primarily because of the superficial nature of the vessel and the ease with which the site can be maintained. Additional advantages of radial artery cannulation include the consistency of the anatomy and the low rate of complications. After the radial artery, the femoral artery is the second most common site for arterial cannulation. One advantage of femoral artery cannulation is that the vessel is larger than the radial artery and has stronger pulsation. Additional advantages include decreased risk of thrombosis and of accidental catheter removal, though the overall complication rate remains comparable. There has been considerable debate over whether radial or femoral arterial line placement more accurately measures blood pressure and mean arterial pressure, however, both approaches seem to perform well for this function. -

Practice Parameter for the Use of Ultrasound to Guide Vascular Access Procedures
PRACTICE GUIDELINES AIUM Practice Parameter for the Use of Ultrasound to Guide Vascular Access Procedures I. Introduction he clinical aspects of this parameter were developed collaboratively among the AIUM and other organizations whose members use ultrasound for guidance in vascular T “ ” access procedures (see Acknowledgments ). Recommendations for practitioner requirements, the written request for the examination, procedure documentation, and quality control vary among the organizations and are addressed by each separately. This parameter has been developed by and for clinicians from diverse specialties and practitioner levels who perform vascular access. While vascular access may be performed using external landmarks, point-of-care ultrasound is now increasingly available.1 Appropriately used, ultrasound guidance for vascular access has been shown to improve success rates while reducing iatrogenic injury, the number of needle passes, and infection rates.2 Addition- ally, it may improve patient comfort and satisfaction. This parameter is intended to be evidence based when possi- ble and to include selected references of importance, but it is not meant to be a comprehensive or rigorous literature review, as this has been accomplished elsewhere.3 The intent of this document is to highlight appropriate evidence while also providing a practical, real-world expert consensus from clinicians with diverse back- grounds on the best use and techniques for incorporating ultra- sound into vascular access procedures with the ultimate goal of improving the care of our patients. II. Indications/Contraindications Ultrasound should be used to aid in central venous, peripheral venous, and arterial access procedures.4 When used appropriately by qualified personnel, there are no absolute contraindications to using ultrasound as a procedural adjunct for vascular guidance. -

Vein Preservation and Alternative Venous Access Exploring the Options for Patients with Chronic Kidney Disease
AV/DIALYSIS ACCESS UPDATE Vein Preservation and Alternative Venous Access Exploring the options for patients with chronic kidney disease. BY THEODORE F. SAAD, MD ince the inception of chronic hemodialysis and the in most cases, although some patients with adequate collat- introduction of the Brescia-Cimino arteriovenous fis- eral venous outflow may develop a functional arteriovenous tula,1 there has been a strong culture favoring vein fistula despite ipsilateral central vein stenosis or occlusion. preservation in the nephrology and hemodialysis Nondominant versus dominant arm: The nondominant Scommunity. During the past 3 decades, there has been con- arm is generally preferred for construction of arteriovenous tinuous growth in the patient population with chronic kid- access. However, depending upon individual patient anato- ney disease (CKD), as well as advances in many medical my and circumstance, the dominant arm is frequently used therapies requiring venous access devices. Many alternatives for hemodialysis access. Therefore, all the same considera- for venous access now exist, including conventional periph- tions apply. eral intravenous catheters, peripherally inserted central catheters (PICCs), nontunneled central venous catheters, DAMAGE CONTROL tunneled central venous catheters (with or without a subcu- Venous access devices damage veins. This is true for any taneous cuff), and subcutaneously implanted ports utilizing intravenous device that is introduced into any peripheral or either central or peripheral veins. As a result, there is consid- central vein. This damage may involve direct trauma to the erable pressure on the limited venous “real estate” available actual puncture site of the vessel, or there may be damage for placement of these devices and creation of arteriove- induced by contact of the device and the vein wall at points nous access. -

Too Many Twos in One Patient: Two Central Venous Catheters, Two
& Experim l e ca n i t in a l l C Journal of Clinical and Experimental C f a o r d l i a o Chalwade, J Clin Exp cardiolog 2018, 9:9 n l o r g u y o Cardiology DOI: 10.4172/2155-9880.1000605 J ISSN: 2155-9880 Case Report Open Access Too Many Twos in One Patient: Two Central Venous Catheters, Two Routes, Two Hospitals, Two Lost Guidewires, Two Vascular Systems, One Patient Rahul Chalwade* Department of Cardiology, Felix Health Care, Noida, Uttar Pradesh, India *Corresponding author: Rahul Chalwade, Department of Cardiology, Felix Health Care, Noida, Uttar Pradesh, India, Phone: +919717053558; E-mail: [email protected] Received date: September 05, 2018; Accepted date: September 10, 2018; Published date: September 17, 2018 Copyright: © 2018 Chalwade R. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Abstract Central venous catheter insertion by Seldinger's technique is a very common procedure nowadays. The technique though considered safe, is associated with potential dreaded complications. One such complication is intravascular loss of guidewire during insertion. We describe one unusual case of two chronically lost guidewires in venous and arterial system with successful retrieval by innovative interventional techniques. Keywords: Lost guidewire; Interventional cardiology; Interventionl AORTA-ARCH OF AORTA-LOOPING IN DESCENDING AORTA- radiology; Central venous catheter complications; Anaesthesiology; OPENING OF LT SCA (straight tip of guidewire). Snare We did routine blood evaluation, all were normal, venous and arterial Doppler and echo was done to rule out thrombus. -

Characteristics and Risk Factors for Intensive Care Unit Cardiac Arrest in Critically Ill Patients with COVID-19—A Retrospective Study
Journal of Clinical Medicine Article Characteristics and Risk Factors for Intensive Care Unit Cardiac Arrest in Critically Ill Patients with COVID-19—A Retrospective Study Kevin Roedl 1,* , Gerold Söffker 1, Dominic Wichmann 1 , Olaf Boenisch 1, Geraldine de Heer 1 , Christoph Burdelski 1, Daniel Frings 1, Barbara Sensen 1, Axel Nierhaus 1 , Dirk Westermann 2, Stefan Kluge 1 and Dominik Jarczak 1 1 Department of Intensive Care Medicine, University Medical Centre Hamburg-Eppendorf, 20246 Hamburg, Germany; [email protected] (G.S.); [email protected] (D.W.); [email protected] (O.B.); [email protected] (G.d.H.); [email protected] (C.B.); [email protected] (D.F.); [email protected] (B.S.); [email protected] (A.N.); [email protected] (S.K.); [email protected] (D.J.) 2 Department of Interventional and General Cardiology, University Heart Centre Hamburg, 20246 Hamburg, Germany; [email protected] * Correspondence: [email protected]; Tel.: +49-40-7410-57020 Abstract: The severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) causing the coron- avirus disease 2019 (COVID-19) led to an ongoing pandemic with a surge of critically ill patients. Very little is known about the occurrence and characteristic of cardiac arrest in critically ill patients Citation: Roedl, K.; Söffker, G.; with COVID-19 treated at the intensive care unit (ICU). The aim was to investigate the incidence Wichmann, D.; Boenisch, O.; de Heer, and outcome of intensive care unit cardiac arrest (ICU-CA) in critically ill patients with COVID-19. G.; Burdelski, C.; Frings, D.; Sensen, This was a retrospective analysis of prospectively recorded data of all consecutive adult patients B.; Nierhaus, A.; Westermann, D.; with COVID-19 admitted (27 February 2020–14 January 2021) at the University Medical Centre et al. -

First Simulator for Seldinger Technique and Angiography Training
This is a repository copy of ImaGiNe Seldinger: first simulator for Seldinger Technique and Angiography Training. White Rose Research Online URL for this paper: http://eprints.whiterose.ac.uk/79950/ Version: Accepted Version Article: Luboz, V, Zhang, Y, Johnson, S et al. (20 more authors) (2013) ImaGiNe Seldinger: first simulator for Seldinger Technique and Angiography Training. Computer Methods and Programs in Biomedicine, 111 (2). 419 - 434. ISSN 0169-2607 https://doi.org/10.1016/j.cmpb.2013.05.014 Reuse Unless indicated otherwise, fulltext items are protected by copyright with all rights reserved. The copyright exception in section 29 of the Copyright, Designs and Patents Act 1988 allows the making of a single copy solely for the purpose of non-commercial research or private study within the limits of fair dealing. The publisher or other rights-holder may allow further reproduction and re-use of this version - refer to the White Rose Research Online record for this item. Where records identify the publisher as the copyright holder, users can verify any specific terms of use on the publisher’s website. Takedown If you consider content in White Rose Research Online to be in breach of UK law, please notify us by emailing [email protected] including the URL of the record and the reason for the withdrawal request. [email protected] https://eprints.whiterose.ac.uk/ ImaGiNe Seldinger: first simulator for Seldinger technique and angiography training V. Luboz, Y. Zhang, S. Johnson, Y. Song, C. Kilkenny, C. Hunt, H. Woolnough, S. Guediri, J. Zhai, T. Odetoyinbo, P. Littler, A. -

Development of a Large Animal Model of Lethal Polytrauma and Intra
Open access Original research Trauma Surg Acute Care Open: first published as 10.1136/tsaco-2020-000636 on 1 February 2021. Downloaded from Development of a large animal model of lethal polytrauma and intra- abdominal sepsis with bacteremia Rachel L O’Connell, Glenn K Wakam , Ali Siddiqui, Aaron M Williams, Nathan Graham, Michael T Kemp, Kiril Chtraklin, Umar F Bhatti, Alizeh Shamshad, Yongqing Li, Hasan B Alam, Ben E Biesterveld ► Additional material is ABSTRACT abdomen and pelvic contents. The same review published online only. To view, Background Trauma and sepsis are individually two of showed that of patients with whole body injuries, please visit the journal online 1 (http:// dx. doi. org/ 10. 1136/ the leading causes of death worldwide. When combined, 37.9% had penetrating injuries. The abdomen is tsaco- 2020- 000636). the mortality is greater than 50%. Thus, it is imperative one area of the body which is particularly suscep- to have a reproducible and reliable animal model to tible to penetrating injuries.2 In a review of patients Surgery, Michigan Medicine, study the effects of polytrauma and sepsis and test novel in Afghanistan with penetrating abdominal wounds, University of Michigan, Ann treatment options. Porcine models are more translatable the majority of injuries were to the gastrointes- Arbor, Michigan, USA to humans than rodent models due to the similarities tinal tract with the most common injury being to 3 Correspondence to in anatomy and physiological response. We embarked the small bowel. While this severe constellation Dr Glenn K Wakam; gw akam@ on a study to develop a reproducible model of lethal of injuries is uncommon in the civilian setting, med. -
IVUS Imaging Catheters Reference Guide
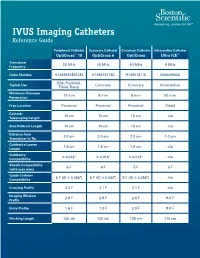
IVUS Imaging Catheters Reference Guide Peripheral Catheter Coronary Catheter Coronary Catheter Intracardiac Catheter OptiCross™ 18 OptiCross 6 OptiCross Ultra ICE™ Transducer 30 MHz 40 MHz 40 MHz 9 MHz Frequency Order Number H7493932800180 H7495181160 H749518110 M00499000 SFA, Popliteal, Typical Use Coronary Coronary Intracardiac Tibial, Renal Maximum Diameter 12 mm 6 mm 6 mm 50 mm Penetration Prep Location Proximal Proximal Proximal Distal Catheter 15 cm 15 cm 15 cm n/a Telescoping Length Sled Pullback Length 10 cm 10 cm 10 cm n/a Distance from 2.0 cm 2.0 cm 2.0 cm 1.0 cm Transducer to Tip Guidewire Lumen 1.6 cm 1.6 cm 1.6 cm n/a Length Guidewire ≤ 0.018" ≤ 0.014" ≤ 0.014" n/a Compatibility Sheath Compatibility 6 F 6 F 5 F 9 F (with max wire) Guide Catheter 6 F (ID ≥ 0.068") 6 F (ID ≥ 0.064") 5 F (ID ≥ 0.058") n/a Compatibility Crossing Profile 3.5 F 3.1 F 3.1 F n/a Imaging Window 2.9 F 2.9 F 2.6 F 9.0 F Profile Entry Profile 1.6 F 1.3 F 2.0 F 9.0 F Working Length 135 cm 135 cm 135 cm 110 cm OPTICROSS™ 18 CATHETER AND MDU5 PLUS BAG OPTICROSS 6 40 MHZ CORONARY IMAGING CATHETER CAUTION Federal law (USA) restricts this device to sale by or on the order of a physician. Rx only. Prior to use, please see the CAUTION: Federal law (USA) restricts this device to sale by or on the order of a physician.