Chiropractic Terminology
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Patients with Cancer. Is There a Role for Chiropractic? Maria Tsampika Laoudikou, Mchiro1 Peter William Mccarthy, Phd1
ISSN 0008-3194 (p)/ISSN 1715-6181 (e)/2020/32–42/$2.00/©JCCA 2020 Patients with cancer. Is there a role for chiropractic? Maria Tsampika Laoudikou, MChiro1 Peter William McCarthy, PhD1 People who have a diagnosis of cancer may develop, Comme tout le monde, les personnes atteintes or already have musculoskeletal conditions, just d’un cancer peuvent développer des troubles like any other person. However, discussion about musculosquelettiques, si elles n’en ont pas déjà. En règle potential benefits of chiropractic treatment to this générale, on évite de discuter des éventuels bienfaits des group has generally been avoided related to the fear traitements chiropratiques pour ce groupe de personnes of misrepresentation. We aimed to derive a consensus de peur de faire de fausses déclarations. Nous avons from a group of experienced chiropractors regarding cherché à obtenir un consensus auprès d’un groupe their perception of what chiropractic care offered to de chiropraticiens d’expérience à qui on a demandé patients with cancer. An anonymous, two stage, on- ce qu’ils pensaient des traitements chiropratiques line, Delphi process was performed using experienced administrés aux patients cancéreux. On a mené une chiropractors (n=23: >10 yrs practice experience, who enquête Delphi anonyme, en deux étapes et en ligne, had treated patients with cancer) purposively selected auprès de chiropraticiens d’expérience (n =23 : >10 ans and recruited independently. One opted out of the study, d’exercice, ayant déjà traité des patients atteints d’un 13 actively engaged in two rounds of questions and cancer) choisis et recrutés de manière indépendante. verification; agreeing such patients gained benefit from L’un d’entre eux a abandonné l’étude, 13 ont répondu chiropractic care but use of spinal manipulation was à deux séries de questions et se sont soumis aux not essential. -

Chiropractic & Osteopathy
Chiropractic & Osteopathy BioMed Central Research Open Access Neuro Emotional Technique for the treatment of trigger point sensitivity in chronic neck pain sufferers: A controlled clinical trial Peter Bablis1, Henry Pollard*1,2 and Rod Bonello1 Address: 1Macquarie Injury Management Group, Macquarie University, Sydney, Australia and 2Director of Research, ONE Research Foundation, Encinitas, California, USA Email: Peter Bablis - [email protected]; Henry Pollard* - [email protected]; Rod Bonello - [email protected] * Corresponding author Published: 21 May 2008 Received: 12 May 2007 Accepted: 21 May 2008 Chiropractic & Osteopathy 2008, 16:4 doi:10.1186/1746-1340-16-4 This article is available from: http://www.chiroandosteo.com/content/16/1/4 © 2008 Bablis et al; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Abstract Background: Trigger points have been shown to be active in many myofascial pain syndromes. Treatment of trigger point pain and dysfunction may be explained through the mechanisms of central and peripheral paradigms. This study aimed to investigate whether the mind/body treatment of Neuro Emotional Technique (NET) could significantly relieve pain sensitivity of trigger points presenting in a cohort of chronic neck pain sufferers. Methods: Sixty participants presenting to a private chiropractic clinic with chronic cervical pain as their primary complaint were sequentially allocated into treatment and control groups. Participants in the treatment group received a short course of Neuro Emotional Technique that consists of muscle testing, general semantics and Traditional Chinese Medicine. -

Acupuncture, Chiropractic, Naturopathy, Massage Therapy)
All plans offered and underwritten by Kaiser Foundation Health Plan of the Northwest 500 NE Multnomah St., Suite 100, Portland, OR 97232 ©2019 Kaiser Foundation Health Plan of the Northwest 337643167_LBG_04-19 Oregon PPO Plus® alternative care benefit (acupuncture, chiropractic, naturopathy, massage therapy) This benefit covers self-referred acupuncture, chiropractic, naturopathic, and massage therapy services. You may choose providers from PPO providers or non-participating providers. Choose your benefit maximum, 3 options: Benefit maximum per year (all services combined, all tiers combined) $1,000 / $1,500 / $2,000 Non-Participating PPO Providers Providers (Tier 1) (Tier 2)2 Services You Pay1 Specialty office visit Specialty office visit Acupuncture services cost share cost share Specialty office visit Specialty office visit Chiropractic services cost share cost share Specialty office visit Specialty office visit Naturopathic medicine cost share cost share Massage therapy (12-visit limit) $25 $25 1If added to an HSA-qualified deductible plan, this benefit is subject to the deductible. 2You may need to file a claim for covered services at non-participating providers. Office visits You do not need a referral to make an appointment. There is no claim form to file for services from Tier 1 providers; you pay your copay or coinsurance directly to the provider when you receive care. Once your benefit limit has been reached, you pay 100% of the cost of services for the remainder of the calendar year. PPO provider You may contact Member Services for additional information or visit kp.org/ppoplus/nw for information on locating a PPO provider. Acupuncture services Acupuncturists influence the health of the body by the insertion of very fine needles. -
Learn More About Chiropractic
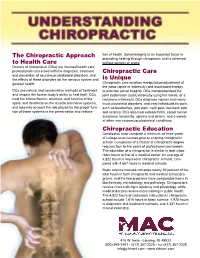
The Chiropractic Approach tion of health. Spinal integrity is an important factor in promoting healing through chiropractic and is achieved to Health Care without surgery or drugs. Doctors of Chiropractic (DCs) are licensed health care professionals concerned with the diagnosis, treatment Chiropractic Care and prevention of neuromusculoskeletal disorders, and the effects of these disorders on the nervous system and is Unique general health. Chiropractic care involves manipulation/adjustment of the joints (spine or extremity) and associated therapy DCs use natural and conservative methods of treatment to promote spinal integrity. DCs manipulate/treat the and respect the human body’s ability to heal itself. DCs joint dysfunction (subluxation) by using the hands, or a treat the biomechanics, structure, and function of the handheld instrument. DCs diagnose injuries and neuro- spine, and its effects on the muscle and nerve systems, musculoskeletal disorders, and treat individuals for pain, and take into account the role played by the proper func- such as headaches, joint pain, neck pain, low-back pain tion of these systems in the preservation and restora- and sciatica. DCs also treat osteoarthritis, carpal tunnel syndrome, tendonitis, sprains and strains, and a variety of other non-neuromusculoskeletal conditions. Chiropractic Education Candidates must complete a minimum of three years of college-level courses prior to entering chiropractic school. Completion of a Doctor of Chiropractic degree requires four to five years of professional coursework. The education of a chiropractor is similar in total class- room hours to that of a medical doctor. An average of 4,822 hours is required in chiropractic schools, com- pared with 4,667 hours in medical schools. -

Effectiveness of Dry Needling for Myofascial Trigger Points Associated with Neck and Shoulder Pain: a Systematic Review and Meta-Analysis
Archives of Physical Medicine and Rehabilitation journal homepage: www.archives-pmr.org Archives of Physical Medicine and Rehabilitation 2015;96:944-55 REVIEW ARTICLE (META-ANALYSIS) Effectiveness of Dry Needling for Myofascial Trigger Points Associated With Neck and Shoulder Pain: A Systematic Review and Meta-Analysis Lin Liu, MSc,a Qiang-Min Huang, MD, PhD,a,b Qing-Guang Liu, MSc,a Gang Ye, MCh,c Cheng-Zhi Bo, BSc,a Meng-Jin Chen, BSc,a Ping Li, PTb From the aDepartment of Sport Medicine and the Center of Rehabilitation, School of Sport Science, Shanghai University of Sport, Shanghai; bDepartment of Pain Rehabilitation, Shanghai Hudong Zhonghua Shipbuilding Group Staff-worker Hospital, Shanghai; and cDepartment of Pain Rehabilitation, Tongji Hospital, Tongji University, Shanghai, China. Abstract Objective: To evaluate current evidence of the effectiveness of dry needling of myofascial trigger points (MTrPs) associated with neck and shoulder pain. Data Sources: PubMed, EBSCO, Physiotherapy Evidence Database, ScienceDirect, The Cochrane Library, ClinicalKey, Wanfang Data Chinese database, China Knowledge Resource Integrated Database, Chinese Chongqing VIP Information, and SpringerLink databases were searched from database inception to January 2014. Study Selection: Randomized controlled trials were performed to determine whether dry needling was used as the main treatment and whether pain intensity was included as an outcome. Participants were diagnosed with MTrPs associated with neck and shoulder pain. Data Extraction: Two reviewers independently screened the articles, scored methodological quality, and extracted data. The results of the study of pain intensity were extracted in the form of mean and SD data. Twenty randomized controlled trials involving 839 patients were identified for meta-analysis. -

The Chiropractic Adjuster (1921)
THE CHIROPRACTIC ADJUSTER A Compilation of the Writings of D. D. PALMER by his son B. J. PALMER. D. C., Ph. C. President THE PALMER SCHOOL OF CHIROPRACTIC Davenport, Iowa, U. S. A. The Palmer School of Chiropractic Publishers Davenport, Iowa Copyright, 1921 B. J. PALMER, D. C., Ph. C. Davenport, Iowa, U. S. A. PREFACE My father was a prolific writer. He wrote much on many subjects. Some were directly apropos to chiropractic, many of them were foreign to it. He was very versatile in thinking, writing and speaking. He was a broad reader and a radical thinker. Away back in the years past, when I was but a boy, I recall going to his waste-basket each night, picking out the many sheets of long-hand, hand-written copies of his writings. I saved them. I saved them through the years, as much as I could. The compilation of these constituted my first step towards a scrapbook. Although chiropractic was not so named until 1895, yet the naming of “chiropractic” was much like the naming of a baby; it was nine months old before it was named. Chiropractic, in the beginning of the thoughts upon which it was named, dates back at least five years previous to 1895. During those five years, as I review many of these writings, I find they talk about various phases of that which now constitutes some of the phases of our present day philosophy, showing that my father was thinking along and towards those lines which eventually, suddenly crystallized in the accidental case of Harvey Lillard, after which it sprung suddenly into fire and produced the white hot blaze. -

Effectiveness of Laser Therapy in the Treatment of Myofascial Pain
American International Journal of Contemporary Research Vol. 6, No. 4; August 2016 Effectiveness of Laser Therapy in the Treatment of Myofascial Pain Lorena Marcelino Cardoso Durval Campos Kraychete Roberto Paulo Correia de Araújo Abstract Myofascial pain is a regional neuromuscular dysfunction of multifactorial etiology that is characterized by the presence of trigger points. It is a common cause of chronic pain and a frequent finding in clinical medicine. The proposed therapeutic procedures aim to reduce pain intensity, inactivate trigger points, rehabilitate muscles and preventively eliminate perpetuating factors. The search for effective treatments and non-invasive options is a topic of ongoing study and, among the proposed therapeutic modalities, laser therapy remains controversial. Objective: To analyze the history of laser therapy in the treatment of myofascial pain, the evolution of research on its effectiveness and the establishment of treatment protocols. Methodology: Analytical study of randomized and controlled clinical trials, double-blinded or single-blinded, describing the effects of laser therapy for myofascial pain or myofascial trigger points, published between 2009 and 2013, and available in the databases PUBMED, MEDLINE, LILACS, IBECS, Cochrane Library, KSCI and SciELO. Results: Regarding the effectiveness of laser therapy for the treatment in question, both positive results and results at the same level as the placebo were observed in the studies. The heterogeneity of the trials does not allow the determination of optimal laser parameters for treatment. Conclusion: According to the data from clinical trials conducted in the last five years, it is still not possible to provide definitive conclusions about the effects of laser therapy for myofascial pain or to establish correlations between the observed results and the parameters employed. -

WCN19 Journal Posters Part 2 Revised V1
JNS-0000116542; No. of Pages 131 ARTICLE IN PRESS Journal of the Neurological Sciences (2019) xxx–xxx Contents lists available at ScienceDirect Journal of the Neurological Sciences journal homepage: www.elsevier.com/locate/jns WCN19 Journal Posters Part 2 revised_V1 WCN19-2260 WCN19-2269 Poster shift 01 - Channelopathies /neuroethics /neurooncology / Poster shift 01 - Channelopathies /neuroethics /neurooncology / pain - Part I /sleep disorders - Part I /stem cells and gene therapy - pain - Part I /sleep disorders - Part I /stem cells and gene therapy - Part I /stroke /training in neurology - Part I and traumatic brain Part I /stroke /training in neurology - Part I and traumatic brain injury injury Numb chin syndrome- The first finding in metastatic malignancy Results of surgical treatment in patients with moyamoya disease considering CT-perfusion imaging study N. Mustafayev, A. Bayrakoglu, F. Ilgen Uslu, M. Kolukısa Bezmialem University, Neurology, Istanbul, Turkey O. Harmatinaa, V. Morozb, I. Skorokhodab, I. Tyshb, N. Shahinb,R. Hanemb, U. Maliarb a Numb chin syndrome (NCS) is a sensory neuropathy of the SI «Romodanov Institute of Neurosurgery of NAMS of Ukraine», mental nerve, which is accompanied by hypoesthesia and paresthe- Neuroradiology Department, Kyiv, Ukraine b sia of the jaw and lower lip. Although being well known in neurology SI «Romodanov Institute of Neurosurgery of NAMS of Ukraine», practice, most of the physicians who have not experienced this Emergency Department of Vascular Neurosurgery, Kyiv, Ukraine phenomenon are unaware of this phenomenon since it is rare and can be confused with somatic complaints. This case report aims to Aim point out that NCS may be the first sign and symptom of metastatic To improve the results of surgical treatment of patients with cancers in patients who are not diagnosed. -

Chiropractic Care Policy
Chiropractic Care Applies to: Blue Cross and Blue Shield of Nebraska Medicare Advantage Plans Chiropractic Care Chiropractic care focuses on disorders of the musculoskeletal system and the nervous system, and the effects of these disorders on general health. Chiropractic care is most often used to treat neuro-musculoskeletal complaints, including but not limited to back pain, neck pain, headaches, and pain in the joints of the arms or legs. Chiropractors utilize a drug-free, hands-on approach to health care that includes patient examination, diagnosis and treatment. The most common therapeutic procedure performed by doctors of chiropractic medicine is known as spinal manipulation. The purpose of manipulation is to restore joint mobility by manually applying a controlled force into joints that have become hypo mobile or restricted in their movement as a result of a tissue injury. Manipulation, or adjustment of the affected joint and tissues, restores mobility, thereby alleviating pain and muscle tightness, and allowing tissues to heal. Original Medicare Original Medicare only pays for chiropractic care services deemed to be medically necessary and reasonable. Under the Original Medicare program, coverage of chiropractic care is specifically limited to treatment by means of manual manipulation (by use of the hands) of the spine to correct a subluxation provided such treatment is legal in the state where performed. Additionally, manual devices (i.e., those that are hand-held with the thrust of the force of the device being controlled manually) may be used by chiropractors in performing manual manipulation of the spine. However, no additional payment is available for use of the device or for the device itself. -

Myofascial Trigger Points of the Shoulder
Johnson McEvoy and Jan Dommerholt Myofascial Trigger Points of the Shoulder Shoulder problems are common, with a 1-year prevalence in developing a more comprehensive approach to shoulder ranging from 4.7% to 46.7% and a lifetime prevalence of rehabilitation. Inclusion of MTrPs in the assessment and 6.7% to 66.7%.1 Many different structures give rise to shoulder management of shoulder pain and dysfunction does not pain, including the structures in the subacromial space, such necessarily replace other techniques and approaches, but it does as the subacromial bursa, the rotator cuff, and the long head of add an important dimension to the management plan. biceps,2,3 and are presented in various lessons. Muscle and spe- cifically myofascial trigger points (MTrPs), have been recog- nized to refer pain to the shoulder region and may be a source TRIGGER POINTS of peripheral nociceptive input that gives rise to sensitization and pain. MTrP referral patterns have been published for the A myofascial trigger point is defined as a hyperirritable spot in shoulder region.4-6 skeletal muscle, which is associated with a hypersensitive Often, little attention is paid to MTrPs as a primary or sec- palpable nodule in a taut band.4 When compressed, a MTrP ondary pain source. Instead, emphasis is placed only on muscle may give rise to characteristic referred pain, tenderness, motor mechanical properties such as length and strength.7,8 dysfunction, and autonomic phenomena.4 MTrPs have been The tendency in manual therapy is to consider muscle pain as described as active or latent. Active MTrPs are associated with secondary to joint or nerve dysfunctions. -
The Scientific Basis of Myofascial Trigger Points
The Scientific Basis of Myofascial Trigger Points Robert Gerwin MD, FAAN Johns Hopkins University, Baltimore, MD Etiology of Myofascial Trigger Points Acute Overuse Direct Trauma Persistent Muscular Contraction (emotional or physical cause), i.e,: poor posture, repetitive motions, stress response Prolonged Immobility Systemic Biochemical Imbalance Etiology of MTrPs (updated) low level muscle contractions Dommerholt J, Bron C, and Franssen J: Myofascial trigger points; an evidence-informed review. J Manual & Manipulative Ther, 2006:14(4):203-221. Gerwin RD, Dommerholt J, and Shah J: An expansion of Simons' integrated hypothesis of trigger point formation. Curr Pain Headache Rep, 2004. 8:468-475. uneven intramuscular pressure distribution direct trauma unaccustomed eccentric contractions eccentric contractions in unconditioned muscle maximal or submaximal concentric contractions Other Contributing Factors Associated MTrP Afferent Input from Joints Afferent Input from Internal Organs Stress / Tension Radiculopathy? MTrP referred pain? Both? Diagnostic criteria spot tenderness within the taut band Diagnostic criteria taut band Muscle Fiber Direction Palpation two palpation techniques: • Flat palpation • Pincer palpation Flat Palpation Scientific Basis of Trigger Points Myofascial Trigger Points exhibit a number of characteristics that require explanation: 1. Structural appearance (hardened muscle band) 2. Biochemical features 3. Nature of local and referred pain 4. Response to treatment The science of myofascial trigger points The anatomic basis of trigger points Electrical Activity of trigger points Sympathetic modulation Vascular changes Biochemical physiology of trigger points Sensitization Treatment effects Trigger Point Structure Motor End PLate Hypothesis: Hypercontracted sarcomeres forming dense, contracted band Sikdar S, et al. Novel Applications of Ultrasound Technology to Visualize and Characterize Myofascial Trigger Points and Surrounding Soft Tissue Arch Phys Med Rehabil. -

Page1/4 MackinzeKennedyLMT,LLC
page1/4 Mackinze Kennedy LMT, LLC Massage Therapy and Reflexology Client Intake Form Personal Information: Name:____________________________________________Phone(day)______________________Phone(eve)_________________________ Address:___________________________________________________________________________________________________________ City/State/Zip:_______________________________________________________________________________________________________ Email:__________________________________________Date of Birth:_____________ Occupation:__________________________________ Emergency Contact:____________________________________Relationship:_____________________Phone: _________________________ The following information will be used to plan safe and effective therapy sessions. Please answer the questions to the best of your knowledge. Date of Initial Visit:__________________ 1. Have you ever received professional massage or reflexology treatment before? Yes No If yes, how often do you receive massage therapy or reflexology ?______________________________________________________ 2. Do you have any difficulty lying on your front, back, or side? Yes No If yes, please explain___________________________________________________________________________________________