Monitoring Report for the State of Jharkhand (April-June 2013)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Booth Name and Location
BOOTH NAME AND LOCATION id PC BLK_NAME BOOTH_NO build_name BOOTH_LOC SENSITIVE build_id m_VOTERS f_VOTERS VOTERS 1 BARKATHA CHANDWARA 1 AAGANBADI KENDRA HARLI AAGANBADI KENDRA HARLI NORMAL 1 282 276 558 2 BARKATHA CHANDWARA 2 U.P.S. BIRSODIH U.P.S. BIRSODIH NORMAL 2 376 350 726 3 BARKATHA CHANDWARA 3 U.M.S. CHAMGUDOKHURD U.M.S. CHAMGUDOKHURD NORMAL 3 325 290 615 4 BARKATHA CHANDWARA 4 N.P.S. CHAMGUDOKALA N.P.S. CHAMGUDOKALA NORMAL 4 280 257 537 5 BARKATHA CHANDWARA 5 U.M.S. CHARKIPAHRI U.M.S. CHARKIPAHRI NORMAL 5 493 420 913 6 BARKATHA CHANDWARA 6 U.M.S. DIGTHU GAIDA U.M.S. DIGTHU GAIDA NORMAL 6 539 470 1009 7 BARKATHA CHANDWARA 7 SAMUDAYIK BHAWAN POKDANDA SAMUDAYIK BHAWAN POKDANDA NORMAL 7 337 341 678 8 BARKATHA CHANDWARA 8 U.M.S. PIPRADIH U.M.S. PIPRADIH NORMAL 8 605 503 1108 9 BARKATHA CHANDWARA 9 U.P.S. ARNIYAO U.P.S. ARNIYAO NORMAL 9 139 120 259 10 BARKATHA CHANDWARA 10 U.P.S. BANDACHAK U.P.S. BANDACHAK NORMAL 10 246 217 463 11 BARKATHA CHANDWARA 11 U.P.S. GARAYANDIH U.P.S. GARAYANDIH NORMAL 11 409 404 813 12 BARKATHA CHANDWARA 12 M.S. KANKO EAST PART M.S. KANKO EAST PART NORMAL 12 498 436 934 13 BARKATHA CHANDWARA 13 M.S. KANKO WEST PART M.S. KANKO WEST PART NORMAL 13 594 507 1101 14 BARKATHA CHANDWARA 14 U.P.S. KURMIDIH U.P.S. KURMIDIH NORMAL 14 195 159 354 15 BARKATHA CHANDWARA 15 U.M.S. -

Hazaribagh, District Census Handbook, Bihar
~ i ~ € :I ':~ k f ~ it ~ f !' ... (;) ,; S2 ~'" VI i ~ ~ ~ ~ -I fI-~;'~ci'o ;lO 0 ~~i~~s. R m J:: Ov c V\ ~ -I Z VI I ~ =i <; » -< HUm N 3: ~: ;;; » ...< . ~ » ~ :0: OJ ;: . » " ~" ;;; C'l ;!; I if G' l C!l » I I .il" '" (- l' C. Z (5 < ..,0 :a -1 -I ~ o 3 D {If J<' > o - g- .,. ., ! ~ ~ J /y ~ ::.,. '"o " c z '"0 3 .,.::t .. .. • -1 .,. ... ~ '" '"c ~ 0 '!. s~ 0 c "v -; '"z ~ a 11 ¥ -'I ~~ 11 CENSUS 1961 BIHAR DISTRICT CENSUS HANDBOOK 14 HAZARIBAGH PART I-INTRODUCTORY NOTE, CENSUS TABLES AND OFFICIAL STATISTICS -::-_'" ---..... ..)t:' ,'t" -r;~ '\ ....,.-. --~--~ - .... .._,. , . /" • <":'?¥~" ' \ ........ ~ '-.. "III' ,_ _ _. ~ ~~!_~--- w , '::_- '~'~. s. D. PRASAD 0 .. THE IlQ)IAJr AD:uJlIfISTBA'X'lVB SEBVlOE Supwtnundent 01 Oen.ua Operatio1N, B'h4r 1961 CENSUS PUBLICATIONS, BIHAR (All the Census Publications of this State will bear Vol. no. IV) Central Government Publications PART I-A General Report PART I-B Report on Vital Statistics of Bihar, 1951-60 PART I-C Subsidiary Tables of 1961. PART II-A General Population Tables· PART II-B(i) Economic Tables (B-1 to B-IV and B-VU)· PAR't II-B(ii) Economic Tables (B-V, B-VI, B-VIII and B-IX)* PART II-C Social and Cultural Tables* PART II-D Migration Tables· PART III (i) Household Economic Tables (B-X to B-XIV)* PART III (ii) Household Economic Tables (B-XV to B-XVII)* PART IV-A Report on Housing and Establishments· PART IV-B Housing and Establishment Table:,* PART V-A Special Tables for Scheduled Castes and Scheduled Tribe&* PART V-B Ethnographic Notes on Scheduled Castes and Scheduled Tribes PART VI Village Surveys •• (Monoglaphs on 37 selected villages) PART VII-A Selected Crafts of Bihar PART VII-B Fairs and Festivals of Bihar PART VIII-A Administration Report on Enumeration * } (Not for sale) PART VIII-B Administration Report on Tabulation PART IX Census Atlas of Bihar. -

Water Supply System in Jhumri Telaiya
Jharkhand Urban Water Supply Improvement Project (RRP IND 52028-004) Initial Environmental Examination Document Stage: Draft Project Number: 52028-004 April 2021 IND: Jharkhand Urban Water Supply Improvement Project – Water Supply System in Jhumri Telaiya Package No: JUWSIP/05 Prepared by Jharkhand Urban Infrastructure Development Co. Ltd. under guidance of the Urban Development and Housing Department, Government of Jharkhand for the Asian Development Bank. CURRENCY EQUIVALENTS (as of 6 April 2021) Currency Unit = Indian rupees (₹) ₹1.00 = $0.013 $1.00 = ₹73.27 ABBREVIATIONS ADB - Asian Development Bank ASI - Archeological Survey of India CPCB - Central Pollution Control Board CPHEEO - Central Public Health and Environmental Engineering Organization CTE - Consent to establish CTO - Consent to Operation EAC - Expert Appraisal Committee EHS - Environmental Health and Safety EIA - Environmental impact assessment EMP - Environmental management plan GLSR - Ground Level Service Reservoir GOI - Government of India GOJ - Government of Jharkhand IEE - initial environmental examination IBA - Important bird area KBA - Key biodiversity area MOHUA - Ministry of Housing and Urban Affairs MOEFCC - Ministry of Environment, Forests and Climate Change MPN - most probable number NOC - no objection certificate O&M - operation and maintenance PIU - project implementation unit PMU - project management unit REA - rapid environmental assessment SEIAA - State Environmental Impact Assessment Authority SPS - Safeguard Policy Statement, 2009 JSPCB - Jharkhand State Pollution Control Board JUWSIP - Jharkhand Urban Water Supply Improvement Project JUIDCO - Jharkhand Urban Infrastructure Development Company Limited WHO - World Health Organization ULB - urban local body WTP - water treatment plant WEIGHTS AND MEASURES m3 – cubic meter °C – degree Celsius Ha – hectare km – kilometer kWh – kilowatt hours L – liters LPCD – liters per capita per day m – meter mps – meters per second MT – metric ton MCM – million cubic meters MLD – million liters per day mm – millimeter nos. -

Sr. No. Branch ID Branch Name City Branch Address Branch Timing Weekly Off Micrcode Ifsccode
Sr. No. Branch ID Branch Name City Branch Address Branch Timing Weekly Off MICRCode IFSCCode Ground Floor, Holiday Inn Plaza, Plot No. C-2/8 & C-2/13, Adityapur - Kandra Main Road, 1 3703 Adityapur Adityapur 9:30 a.m. to 3:30 p.m. 2nd & 4th Saturday and Sunday 833211103 UTIB0003703 Adityapur Pin code 831013 2 3535 Baraon Baranwa 156 A, Madhudih Tola, PS: Chainpur, Baranwa, Garhwa Road Palamu 822110 9:30 a.m. to 3:30 p.m. 2nd & 4th Saturday and Sunday 822211501 UTIB0003535 Premises at Ground and First Floor at Kalabati Market , Barhi Chowk , Gaya Road , PO & 3 3790 Barhi Barhi 9:30 a.m. to 3:30 p.m. 2nd & 4th Saturday and Sunday 825211601 UTIB0003790 PS : Barhi , Dist: Hazarabagh , Jharkhand - 825405 Hotel Blue Diamond, 15 D/1, Western Avenue, Bokaro Steel City, Bokaro 827 001, 4 171 Bokaro Bokaro Steel City 9:30 a.m. to 3:30 p.m. 2nd & 4th Saturday and Sunday 827211002 UTIB0000171 Jharkhand L. D. House, Opposite Hanuman Mandir, Amlatola, PS. Sadar Thana, Chaibasa, 5 1172 Chaibasa Chaibasa 9:30 a.m. to 3:30 p.m. 2nd & 4th Saturday and Sunday 833211002 UTIB0001172 Jharkhand, Pin 833201 First Floor, Ranchi Main Road, Kedia Petrol Pump, PO & PS: Chakradharpur, Dist: West 6 3222 Chakradharpur Chakardharpur 9:30 a.m. to 3:30 p.m. 2nd & 4th Saturday and Sunday 833211202 UTIB0003222 Singhbhum , Jharkhand, Pin Code: 833012 Ground Floor, Rajdoot Hotel, Near K M Memorial Hospital, Bye Pass Road, Chas, Dist. 7 2069 Chas Chas 9:30 a.m. to 3:30 p.m. -

2019021687.Pdf
Marks Weightage Pattern for Assistant Technology Manager (ATM), District Koderma ~ 15/02/2019 q;t ~ c5t GTCIT/~ c5t f.'I~lqHUI·~ ~ lJ1'fTUT-W c5t \il"Rr (~ ~) SL Rese. Name of Corres Add. Date of Birth Educational Qualification (60% weightage) (60 Marks) Computer Knowledge Special weightage (I 0%) Total Home Remarks No. Categor Applicant (30% wei htage) (30 Marks) (10 Marks) marks Distt. y Intermediate (Max. I 0 Marks) Graduate in Agril/Horti !Economics. PG in Excel Power Word Candidates worked 2 or obtained IMarketing Neterinary Science Agril/Horti/Economics.lMarketing (Max 10 point (Max 15 more than 2 yrs. In (Max.IOO IAHD/Fisheries (Max.35 Marks) Neterinary Science IAHD/Fisheries Marks) (Max 5 Marks) (ATMNSAMETI) marks) ) (Max.15 Marks) Marks) (Max 10 Marks) Total Marks Marks Weightage Total Marks Marks obtain Weightage Total Marks Marks Weightage 2 or more Marks obtain obtain in than 2 vr I 2 3 4 5 6 7 8 9 10 11 12 13 14 IS 16 17 18 19 20 21 22 I UR PINKY KUMARI C/O-INDRA NARAYAN 06-09-92 500 257 5.14 1500 873 20.37 1100 885 12.06 - 37.57 Koderrna Eligible SINGH by pass road- koderma 2 UR VIKASH KUNAL S/O- KRISHNA RAJAK 07-06-92 500 304 6.08 100 62.5 21.875 - - - - - - - 27.955 Koderrna Eligible VIDYAPURI NEAR RAMESHWER MODI MANDIR JHUMRI TELAIYA KODERMA JHARKHAND 3 BC1 PINTU KUMAR VILL POST PS 05-11-84 900 464 5.15 1500 753 17.57 - - - - - - 22.72 Koderrna Eligible RANA CHANDWARA DIST Iv"neo" 4 BC1 HARISHCHANDR AT - KAKARCHOU PQ+PS- 13/04/1986 900 449 4.98 1500 722 16.84 - - 21.82 Kodenna Eligible ARANA JAINAGAR I nO<T_ .nneo". -
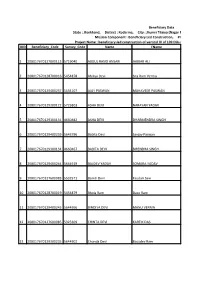
IDD Beneficiary Code Survey Code Name Fname 1
Beneficiary Data State : Jharkhand, District : Kodarma, City : Jhumri Tilaiya (Nagar Parishad), Financial Year : All Financial Year Mission Component : Beneficiary Led Construction, Project Status : All Project Status Project Name : beneficiary-led construction of vertical IV of 109 DUs under PMAY of Jhumritiliya ULB , Jharkhand IDD Beneficiary_Code Survey_Code Name FName 1 208017670127800113 5719040 ABDUL RASID ANSARI JABBAR ALI 2 208017670128700016 5454878 Ahiliya Devi Sita Ram Verma 3 208017670129400237 5634107 AJAY PASWAN MAHAVEER PASWAN 4 208017670129200122 5725803 ASHA DEVI NARAYAN YADAV 5 208017670129300131 4660482 ASHA DEVI DHARMENDRA SINGH 6 208017670129400239 5643796 Babita Devi Sanjay Paswan 7 208017670129300134 4660467 BABITA DEVI BIRENDRA SINGH 8 208017670129400244 5644919 BALDEV YADAV SOMARA YADAV 9 208017670127600083 5532571 Basnti Devi Faudari Saw 10 208017670128700019 5454879 Bhola Ram Daso Ram 11 208017670129400245 5644966 BINDIYA DEVI MANU VERMA 12 208017670127600085 5325309 CHINTA DEVI KARTIK DAS 13 208017670129300235 5644902 Chunda Devi Basudev Ram 14 208017670128700018 5454856 Damodar Saw Bachan Saw 15 208017670129300237 5644906 DAMODAR THAKUR AMRIT THAKUR 16 208017670129400238 5643808 Devnath Misra Ramdas Misra 17 208017670127400298 5596969 Durga Prasad Shahi Kali Prasad Shahi 18 208017670128200010 5471081 Durga Saw Mishri Saw 19 208017670129400218 4637979 GIRIJA DEVI LAKHAN PASWAN 20 208017670127700200 5730520 JAYDIP KUMAR RAM NAGESHWAR RAM 21 208017670127600088 5325633 Jira Devi Manoj Das 22 208017670127400323 -

State District City Address Type Jharkhand Bokaro
STATE DISTRICT CITY ADDRESS TYPE AXIS BANK ATM, KHATA NO.211 POLO NO. 1445 MOZA NO. 28 JHARKHAND BOKARO BOKARO THANA NO 108, AGARWAL MEDICINE STORE, BANK MORE CHOWK, OFFSITE GOMIA BOKARO JHARKHAND. 829111. AXIS BANK ATM, MAIN ROAD CHAS, P.O+P.S- CHAS, DIST- BOKARO, JHARKHAND BOKARO BOKARO OFFSITE JHARKHAND - 827013 AXIS BANK ATM, MAIN ROAD CHAS NEAR PETROL PUMP,PO- JHARKHAND BOKARO BOKARO OFFSITE CHAS,DIST-BOKARO,PIN-827013, JHARKHAND AXIS BANK LTD, GROUND FLOOR , THE RAJDOOT HOTEL, NEAR JHARKHAND BOKARO BOKARO K.M.MEMORIAL HOSPITAL,BYE PASS ROAD, CHAS – ONSITE BOKARO,JHARKHAND,PIN CODE: 827013. AXIS BANK LTD, GROUND FLOOR , NEAR HOTEL URVARSHI, MAIN JHARKHAND BOKARO BOKARO ONSITE ROAD PHUSRO BAZAR, JHARKHAND. 829144 AXIS BANK ATM CENTRE MARKET SECTOR 9 PLOT NO C2 BOKARO JHARKHAND BOKARO BOKARO OFFSITE STEEL CITY BOKARO JHARKHAND 827009 AXIS BANK LTD OPPOSITE KALI MANDIR POST OFFICE MORE PO JHARKHAND BOKARO BOKARO ONSITE GOMIA DIST BOKARO JHARKHAND 829111 AXIS BANK ATM KHATA NO 350 PLOT NO 4709 RAKWA 38 DISMIL JHARKHAND BOKARO BOKARO THANA NO 123 MOUJA HOSIR MAIN ROAD SADAM PO HOSIR PS OFFSITE GOMIA DIST BOKARO JHARKHAND 829111 AXIS BANK ATM, HOLDING NO:-148, WARD NO:-17, P.O:-CHATRA, JHARKHAND CHATRA CHATRA P.S:-CHATRA, NEAR OLD PETROL PUMP , MAIN ROAD CHATRA, DIST:- OFFSITE CHATRA, JHARKHAND, PIN-825401 AXIS BANK ATM, KHATA NO:- 117, PLOT NO:- 574, WARD NO;-21, HOLDING NO:- 156A OLD/ 05 NEW, RAKWA:- 2.75 DISMIL, THANA JHARKHAND CHATRA CHATRA NO:- 005, HALKA- 6B, MOUZA:- NAGWA, ANCHAL:- CHATRA, OPP. DC OFFSITE OFFICE NEAR COLLEGE ROAD CHATRA, DIST- CHATRA, JHARKHAND, PIN-825401 AXIS BANK LTD, GROUND & FIRST FLOOR MAIN ROAD PO & PS JHARKHAND CHATRA CHATRA ONSITE CHATRA DIST CHATRA 825401 JHARKHAND AXIS BANK ATM, CIRCULAR ROAD NEAR SATSANG CHOWK,PO- JHARKHAND DEOGHAR BELABAGAN OFFSITE BELABAGAN,DIST-DEOGHAR, 814112 AXIS BANK ATM, AT: ECL, CHITRA, OPP. -
Bandi Dighu, PO-Chandwara, Jhumritelaiya, Dist- Koderma
Techno Economic Feasibility Report of M/s Shivam Iron & steel Co Ltd At: Bandi Dighu, P.O-Chandwara, Jhumritelaiya, Dist- Koderma, Jharkhand 1 Global Tech Enviro Experts Pvt. Ltd. Techno Economic Feasibility Report of M/s Shivam Iron & steel Co Ltd At: Bandi Dighu, P.O-Chandwara, Jhumritelaiya, Dist- Koderma, Jharkhand TABLE OF CONTENTS CHAPTER-1 ........................................................................................................................ 4 EXECUTIVE SUMMARY ................................................................................................... 4 CHAPTER-2 ........................................................................................................................ 8 INTRODUCTION OF THE PROJECT ............................................................................... 8 2.1 IDENTIFICATION OF PROJECT & PROJECT PROPONENT ......................... 8 2.2 BRIEF DESCRIPTION OF NATURE OF THE PROJECT ................................. 8 2.3 IMPORTANCE OF THE PROJECT TO THE COUNTRY AND REGION .......... 8 2.3.1 DOMESTIC SCENARIO ..................................................................................... 9 2.3.2 GLOBAL STEEL SCENARIO ...................................................................... 12 2.4 EMPLOYMENT GENERATION DUE TO PROJECT ....................................... 12 2.5 METHODOLOGY OF THE STUDY ................................................................... 12 2.6 ENVIRONMENTAL MANAGEMENT PLAN: ................................................... 14 2.7 LITIGATION/COURT -
Koderma District, Jharkhand State
भूजल सूचना पुस्तिका कोडरमा स्जला, झारखंड Ground Water Information Booklet Koderma District, Jharkhand State केन्द्रीय भसू मजल बोडड Central Ground water Board जल संसाधन मंत्रालय Ministry of Water Resources (भारि सरकार) (Govt. of India) State Unit Office, रा煍य एकक कायाडलय, रााँची - Ranchi मध्य पूर्वी क्षेत्र Mid-Eastern Region पटना Patna ससिंबर 2013 September 2013 1 भूजल सूचना पस्ु तिका कोडरमा स्जला, झारखंड Ground Water Information Booklet Koderma District, Jharkhand State Prepared By K.Lakshmi Narayan (Scientist-B) Supervised By हﴂ टी बी एन स (वैज्ञाननक ग ) T. B. N. Singh (Scientist C) रा煍य एकक कायाडलय, रााँची मध्य-पूर्वी क्षेत्र,पटना State Unit Office, Ranchi Mid Eastern Region, Patna 2 Contents Serial no. Contents 1.0 Introduction 1.1 Administration 1.2 Drainage 1.3 Land use, Irrigation and Cropping pattern 1.4 Studies, activities carried out by C.G.W.B. 2.0 Climate 2.1 Rainfall 2.2 Temperature 3.0 Physiography and Drainage 4.0 Ground water scenario 4.1 Geology and Hydrogeology Aquifer systems Exploratory Drilling Well design Water levels (Pre-monsoon, post-monsoon) 4.2 Ground water Resources 4.3 Ground water quality 4.4 Status of ground water development 5.0 Ground water management strategy 6.0 Ground water related issues and problems 7.0 Awareness and training activity 8.0 Area notified by CGWA/SCGWA 9.0 Recommendations 3 List of Tables Table 1 Geological succession of Koderma Mica Belt Table 2 Exploratory wells drilled in Koderma district Table 3 Block-wise Ground water Resources of Koderma district (2009) Table 4 Range of chemical quality of Deeper aquifer in Koderma district Table 5 Range of chemical quality of Shallow aquifer in Koderma district Table 6 Block wise Results of Chemical Quality of Koderma district List of Figures Fig. -

College ID State University College Name Road City District Pin
College ID State University College name Road City District Pin Payable at IFSC No AC No MICR No BBA2-001 Bihar BBA Bihar Awadh Bihari Singh Mahavidyalaya Lalganj Vaishali Canara Bank,Lalganj Vaishali CNRB 0001252 125220150212 BBA2-003 Bihar BBA Bihar Braj Mohan Das College Dayalpur, Vaishali 844502 Allahabad Bank, Dyalpur Vaishali ALLA0210006 20263644708 844010002 BBA2-004 Bihar BBA Bihar Chandradeo Narain College Sahebganj Muzaffarpur 843125 Central Bank of India, Sahebganj Muzaffarpur CBIN0280026 2195891667 26 BBA2-005 Bihar BBA Bihar Dr S K Sinha Women's College Motihari 845401 State Bank of India, Motihari SBIN0001231 10953148213 845002003 BBA2-006 Bihar BBA Bihar Dr Ram Manohar Lohia Smarak Mahavidyalaya Muzaffarpur 842001 Canara Bank, Motijheel,Muzaffarpur CNRB0000258 0258201001285 842015002 BBA2-007 Bihar BBA Bihar Deo Chand College Hajipur, Vaishali 844101 Hajipur SBIN0012572 31505518429 844002004 BBA2-008 Bihar BBA Bihar Dr Jagannath Mishra College Muzaffarpur 842001 United bank of India, Motijheel, Muzaffarpur UTBIOMTJJ07 0825010102000 8420270002 BBA2-010 Bihar BBA Bihar Jagannath Singh College Chandauli Sitamarhi 843316 State Bank of India, Sitamarhi SBIN0004654 11621131845 843002503 BBA2-011 Bihar BBA Bihar Jamunilal Mahavidyalaya Hajipur Vaishali 844101 Punjab National Bank, Hajipur Vaishali PUNB0403700 4037000100062968 844024002 BBA2-013 Bihar BBA Bihar Jeewachh Mahavidyalaya Motipur, Muzaffarpur 843111 Punjab National Bank, Muzaffarpur PUNB0033400 0334000100194870 842024002 BBA2-015 Bihar BBA Bihar Khem Chand Tara Chand -
Sl No. Workshop Name Cashless
Cashless/ Type of Sl No. Workshop Name Address Pin Code City State Zone CSO Contact Person Mobile No. Email id Segment Manufacturer Preferred Repairer SOUMENDRA ` ULTRACRAFT Cashless 103/1B, Raja Dinendra Street 700006 Kolkata West Bengal East Kolkata 9830741255 [email protected] Four Wheeler MARUTI ASC GHOSAL MAHANSARIA & SONS PVT. General 2 Preferred 109,N S Road, Mahinagar, Rajpur 700145 Kolkata West Bengal East Kolkata ARUP ROY 9831553520 [email protected] Four Wheeler MULTI BRAND LTD. Platform 3 CAMAC Cashless 2E & F, Camac Street 700016 Kolkata West Bengal East Kolkata ARUP ROY 9831553520 [email protected] Four Wheeler MARUTI ASC ANANTA LAL General 4 PRIME MOTORS Preferred 9, Gurusaday Road 700019 Kolkata West Bengal East Kolkata 9831955441 Four Wheeler MULTI BRAND SHARMA Platform 5 DELUX SERVICE STATION Cashless 110, Hem Chandra Naskar Road 700010 Kolkata West Bengal East Kolkata BIPLAB DAS 9836490084 Four Wheeler MARUTI ASC General 6 AUTO BOD Preferred 8C/1P, JAGODYAN LANE 700054 Kolkata West Bengal East Kolkata BIPLAB DAS 9836490084 Four Wheeler MULTI BRAND Platform BENGAL MOTOR SERVICES 7 Cashless 242/2A, Satin Sen Sarani 700054 Kolkata West Bengal East Kolkata MAMUN MANDAL 9748887131 [email protected] Four Wheeler HYUNDAI Dealer PVT. LTD. DEBIJYOTI 8 K B MOTORS PVT. LTD. Cashless 7A, Rameshwar Shaw Road 700014 Kolkata West Bengal East Kolkata 9831959916 [email protected] Four Wheeler TATA Dealer MUKHERJEE BAGARIA MOTORS PVT. DEBIJYOTI 9 Cashless 7A, Rameshwar Shaw Road 700014 Kolkata West Bengal East Kolkata 9831959916 [email protected] Four Wheeler RENAULT Dealer LTD. MUKHERJEE General 10 BALAJI AUTO CENTER Preferred 10, Paschim Chowbhaga, Dhalenda 700105 Kolkata West Bengal East Kolkata NARAYAN DHELIA 9830919887 [email protected] Four Wheeler MULTI BRAND Platform SHREE AUTOMOTIVE PVT. -

Download Article (PDF)
CITATION Chakraborty, Rina 2011. Mammalian and Avian Faunal Diversity in Damodar Valley under DVC Project Area, Rec. zool. Surv. India, Occ. Paper No., 328 1-38, (Published by the Director, Zool. Surv. India, Kolkata) Published: May, 2011 ISBN 978-81-8171-289-9 © Gout. of India, 2011 ALL RIGHTS RESERVED • No Part of this publication may be reproduced, stored in a retrieval system or transmitted in any form or by any means, electronic, mechanical, photocopying, recording or otherwise without the prior permission of the publisher. • This book is sold subject to the condition that it shall not, by way of trade, be lent, resold, hired out or otherwise disposed off without the publisher's consent, in a form of binding or cover other than that in which, it is published. • The correct price of this publication is the price printed on this page. Any revised price indicated by a rubber stamp or by a sticker, or by any other means is incorrect and should be unacceptable. PRICE Indian ~ 150.00 Foreign $ 9 £ 6 Published at the Publication Division, by the Director, Zoological Survey of India, 234/4 A.J.e. Bose Road, 2nd MSO Building, Nizam Palace (13th floor), Kolkata 700 020 and printed at Typographia, Kolkata 700 012. KI!;~~~RENCE NOT FOR ISSUE RECORDS OF THE ZOOLOGICAL SURVEY OF INDIA OCCASIONAL PAPER No. 328 2011 Page 1-38 CONTENTS INTRODUCTION .................................................................................................................. 1 TOPOGRAPHY ....................................................................................................................