Introduction
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Framatome in Latin America Strong History and Partnerships
SEN – Semana da Engenharia Nuclear UFRJ 17/10/2019 Framatome– 2019 1 © Framatome All right reserved Framatome– 2019 2 © Framatome All right reserved Framatome at a glance 60 years of experience, alongside our customers, in developing safe and competitive nuclear power worldwide Design Supply Manufacture Integrate Maintain Framatome– 2019 3 © Framatome All right reserved Framatome at a glance High-performing people and technologies for safe and competitive nuclear plants worldwide 92 14 000 250 3.3 NPPs PEOPLE REACTORS € BILLION As OEM Servicing … All over the world 2017 turnover Framatome– 2019 4 © Framatome All right reserved Our values More than principles, our values guide our actions and describe how we work each other, with our customers and business partners Safety Future Performance Integrity Passion Framatome– 2019 5 © Framatome All right reserved Framatome worldwide presence Germany 4 sites France 17 sites USA 7 sites China 8 sites 58 locations Argentina Japan Sweden 21 Belgium Republic of South Switzerland countries Others Brazil Africa The Netherlands locations Bulgaria Russia Ukraine Canada Slovakia United Arab Emirates Framatome– 2019 Czech Republic Slovenia United Kingdom 6 Finland South Korea © Framatome Hungary Spain All right reserved Our customers Asia CNNC Nawah CGN Tepco North & South America Doosan Hitachi Bruce Power Exelon OPG KHNP Dominion Corporation PSEG Africa MHI Duke Energy Luminant TVA Entergy NA-SA Eskom ETN NextEra Europe ANAV EDF Energy Skoda CNAT Engie TVO CEA EPZ Vattenfall CEZ Iberdrola DCNS KKG EnBW NEK Framatome– 2019 7 EDF RWE © Framatome All right reserved Framatome shareholder structure 19,5% 75,5% 5% • Stock-listed company • Majority shareholder: French state 100% Framatome Inc. -
RIL AMT Workshop Summary
RIL 2021-03 NRC WORKSHOP ON ADVANCED MANUFACTURING TECHNOLOGIES FOR NUCLEAR APPLICATIONS Part I – Workshop Summary Date Published: Draft April 2021 Prepared by: A. Schneider M. Hiser M. Audrain A. Hull Research Information Letter Office of Nuclear Regulatory Research Disclaimer This report was prepared as an account of work sponsored by an agency of the U.S. Government. Neither the U.S. Government nor any agency thereof, nor any employee, makes any warranty, expressed or implied, or assumes any legal liability or responsibility for any third party’s use, or the results of such use, of any information, apparatus, product, or process disclosed in this publication, or represents that its use by such third party complies with applicable law. This report does not contain or imply legally binding requirements. Nor does this report establish or modify any regulatory guidance or positions of the U.S. Nuclear Regulatory Commission and is not binding on the Commission. EXECUTIVE SUMMARY Advanced manufacturing technologies (AMTs) are defined by the U.S. Nuclear Regulatory Commission (NRC) as those techniques and material processing methods that have not been traditionally used or formally standardized/codified by the nuclear industry. In June 2020, the NRC released Revision 1 to the Agency Action Plan for AMTs (AMT AP) (Agencywide Documents Access and Management System Accession No. ML19333B980 (package)). The AMT AP is a strategic plan that responds to the rapid pace of developments in respective AMTs and industry implementation plans. The NRC’s AMT activities are driven by industry interest in implementing specific AMTs and ensuring that the NRC staff are prepared to review potential AMT applications efficiently and effectively. -

ITER Project Garching for the Fusion Community an Historic Milestone Was Achieved at the Eighth ITER Negotiations Meeting on February 18-19, 2003 in St
newsletternewsletter Vol 2003 / 2 April 5, 2003 EUROPEAN FUSION DEVELOPEMENT AGREEMENT News Issued by the EFDA Close Support Unit China and the US as New Partners in the ITER Project Garching For the fusion community an historic milestone was achieved at the Eighth ITER Negotiations Meeting on February 18-19, 2003 in St. Petersburg (Russian Federation), when delega- tions from the People’s Republic of China and the United States of America joined those from Canada, the European Union, Japan and the Russian Federation in their efforts to reach agreement on the implementation of the ITER pro- ject. The Head of the Chinese Delegation indicated that Contents China, as the largest developing country in the world, has a great need to pursue alternative energy sources. China . Interview: believes that ITER can potentially lead to new forms of ener- Dr. Joseph V. Minervini gy and contribute to the peaceful and sustainable development page 2 of the world in the long-term. China expressed its strong wishes to be a valuable member of the ITER family, to make joint efforts with . Interview: other partners to the successful exploitation of fusion energy. Prof. Huo Yuping At their St. Petersburg meeting the ITER Negotiators approved the Report on the page 3 Joint Assessment of Specific Sites (JASS). The JASS Report provided as a main con- clusion and despite the differences between the candidate sites (Clarington in Canada, . ITER: Cadarache in France, Vandellos in Spain and Rokkasho-mura in Japan) that the JASS First Full Scale Primary assessment ascertained that all four sites are sound and fully capable to respond to all First Wall Panel ITER Site Requirements and Design Assumptions, as approved by the ITER Council in its January 2000 meeting. -

Olkiluoto 3: Framatome Teams All Set for Fuel Loading
PRESS RELEASE March 26, 2021 Olkiluoto 3: Framatome teams all set for fuel loading March 26, 2021 – The Olkiluoto 3 EPR reactor completes a decisive stage of its commissioning. The Finnish safety authority (STUK) has authorized the fuel load for the Olkiluoto 3 EPR reactor. Loading operations led by plant operator TVO, with the support from AREVA and Framatome, can begin. "Fuel loading is a major milestone for the project. Reaching this milestone illustrates the expertise and know-how of our teams," said Bernard Fontana, CEO of Framatome. "Framatome's teams are fully mobilized alongside AREVA and TVO to finalize and deliver the nuclear power plant while meeting the highest safety and security standards. I thank them for their engagement.” To carry out the loading operations, an integrated team made up of approximately 40 employees from TVO, AREVA and Framatome has been formed. It includes around 15 fuel handlers, employees specializing in the fuel handling operations, and four neutronics engineers in charge of monitoring the core during loading. A total of 241 fuel assemblies manufactured in Framatome's plants in Germany and in France will be loaded in the reactor vessel to constitute the first core. The Areva NP and Areva NP GmbH Olkiluoto 3 project teams, who will later join Framatome, are supported by over 110 Framatome employees permanently based on the site, and by Framatome engineering teams located in France and in Germany. Completion of the fuel loading will be followed by a new series of hot functional tests before the first criticality and commissioning for commercial operation. -

Specials Steels and Superalloys for Nuclear Industry
Specials Steels and Superalloys for Nuclear Industry Enhancing your performance or almost 60 years Aubert & Duval has been a key partner for the development Aubert & Duval: Your partner F of forged and rolled products, especially those customized for the nuclear market. to energize your success With full vertical integration from melting, to remelting, hot converting and machining (rough machining through to near-net-shape parts), Aubert & Duval offers wide-ranging cutting edge capabilities for nuclear application. Equipment Process flow . MELTING Melting furnaces (EAF, AOD, LF) Melting up to 60 tons Vacuum Induction Melting (VIM) HPS NiSA up to 20 tons Remelting furnaces (ESR, VAR) up to 30 tons powder atomization (Gaz, VIM) . FORGING Open-die forging presses Remelting Powder atomization from 1,500 to 10,000 tons Closed-die forging presses from 4,500 to 65,000 tons . ROLLING MILL HPS 7-200 mm diameter bars High Performance Steels: Conversion . HEAT TREATMENT A range of alloyed steels with Solution and ageing furnaces tightly controlled characteristics HPS Ti NiSA AL PM Horizontal and vertical quenching offering optimum value for equipment customers. TESTING Forging Closed-die Hot Isostatic Immersion UT up to 13 tons and/or rolling Forging Forging Pressing (HIP) ©Valinox-Franck Dunouau (28,000 lbs) Automated contact UT up to 20 tons NiSA Aubert & Duval has also put in place over many decades dedicated skills to co-design re-engineered Nickel-base Superalloys: Nickel-based superalloys: materials metallurgical solutions with our clients. keeping high surface integrity while Sales of alloys and superalloys have progressively expanded across a broad spectrum of primary withstanding severe mechanical circuit contractors and their subcontractors. -

Press Kit Inauguration of the Conversion Orano Tricastin BP 16 26 701 Pierrelatte Plant 10 September 2018
Press kit Inauguration of the conversion Orano Tricastin BP 16 26 701 Pierrelatte plant 10 September 2018 Contacts Presse Nathalie Bonnefoy +33 (0)6 23 17 24 24 [email protected] Gilles Crest +33 (0)6 71 08 11 54 [email protected] www.orano.group Oranogroup EDITORIAL The plant we are opening today is a major industrial investment for Orano, for the French nuclear industry and for the industry of our country. ith the Georges Besse II enrichment plant on the same site, it is probably the largest industrial investment made in France in recent years. The Comurhex W II project was launched to give France an industrial facility offering cutting- edge safety, security, and environmental and industrial performance. A facility that gives us a global competitive advantage and guarantees an uninterrupted electricity supply for our markets. A tool integrating technological innovations in terms of safety, environment, and improvement of industrial performance: recycling of chemical reagents, reduction by 90% of water consumption, automated control-command system to improve the process control. It is an exceptional project that has required the best of our expertise from the teams of Orano Chemistry and Enrichment as well as Orano Projets, and throughout our group alongside our industrial partners. The project successfully completed at the same time as our group was reinventing itself to create a new flagship technology business to give nuclear materials all their value. While an important debate is taking place on France's multi-year energy program, the investment we have made in the Tricastin site and its plants shows the confidence we have in the future of nuclear energy. -

The Jules Horowitz Reactor Core and Cooling System Design
The Jules Horowitz Reactor core and cooling system design M. Boyard*, JM. Cherel**, C. Pascal*, B. Guigon*** * AREVA-Technicatome, 1100 rue Jean René Guillibert Gautier de la Lauzière 13100 Aix en Provence, FRANCE ** AREVA-Framatome-ANP, 9-10 rue Juliette Récamier 69006 Lyon, FRANCE *** Commissariat à l’Energie Atomique, 13108 Saint-Paul-lez-Durance cedex, FRANCE ABSTRACT The CEA (Commissariat à l’Energie Atomique) is planning to build a new MTR called the Jules Horowitz Reactor (JHR). JHR at Cadarache will become by 2014 and for decades a major research infrastructure in Europe for supporting existing power plants operation and lifetime extension as well as future reactor developments [1]. AREVA (Technicatome and Framatome- ANP) and EDF are performing the design studies. The JHR will be a tank pool type reactor using light water as coolant and moderator. The reactor has been designed to provide a neutron flux strong enough to carry out irradiation relevant for generations 2, 3 and 4 power plants: flexibility and adaptability, high neutron flux, instrumented experiments, loops to reproduce environments representatives of the different power plant technologies . Updated safety requirements and LEU fuel elements have been taken into account in the design of this high flux reactor. This paper presents the guidelines for the design of the main items, the various options considered and the choices made at the end of the detailed studies phase regarding: − Core shape, − Fuel element and core pitch, − Reflector and core-reflector interface, − Normal and emergency cooling systems, − Reactivity control system. MAIN OBJECTIVES OF THE REACTOR The “Jules Horowitz Reactor” (JHR) will be a structuring infrastructure of the European research area. -

Operational and Decommissioning Experience with Fast Reactors
IAEA-TECDOC-1405 Operational and decommissioning experience with fast reactors Proceedings of a technical meeting held in Cadarache, France, 11–15 March 2002 August 2004 IAEA-TECDOC-1405 Operational and decommissioning experience with fast reactors Proceedings of a technical meeting held in Cadarache, France, 11–15 March 2002 August 2004 The originating Section of this publication in the IAEA was: Nuclear Power Technology Development Section International Atomic Energy Agency Wagramer Strasse 5 P.O. Box 100 A-1400 Vienna, Austria OPERATIONAL AND DECOMMISSIONING EXPERIENCE WITH FAST REACTORS IAEA, VIENNA, 2004 IAEA-TECDOC-1405 ISBN 92–0–107804–8 ISSN 1011–4289 © IAEA, 2004 Printed by the IAEA in Austria August 2004 FOREWORD The fast reactor, which can generate electricity and breed additional fissile material for future fuel stocks, is a resource that will be needed when economic uranium supplies for the advanced water cooled reactors or other thermal-spectrum options diminish. Further, the fast-fission fuel cycle in which material is recycled offers the flexibility needed to contribute decisively towards solving the problem of growing ‘spent’ fuel inventories by greatly reducing the volume of high level waste that must be disposed of in long term repositories. This is a waste management option that also should be retained for future generations. The fast reactor has been the subject of research and development programmes in a number of countries for more than 50 years. Now, despite early sharing and innovative worldwide research and development, ongoing work is confined to China, France, India, Japan, the Republic of Korea, and the Russian Federation. Information generated worldwide will be needed in the future. -
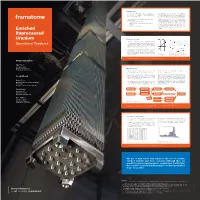
Operational Feedback Ventional Enriched FA
Background › Starting in 2009, Framatome has been supplying Size- › Totally Framatome has delivered more than 1000 FAs to well B* with fuel assemblies (FAs) with Enriched Re- Sizewell B, approximately half of them containing ERU. processed Uranium (ERU). The enrichment process of the reprocessed uranium is completed in Russia with an objective of minimizing even › Reprocessed uranium is understood as a secondary uranium isotopes such as 232U and 236U. The even isoto- uranium supply pes do not contribute to fi ssion; they are considered – by direct enrichment services to be an absorber and therefore, their presence needs to be minimized, which improves overall fuel utilization. – by blending with other feed material of a higher The low residual fraction of these parasitic isotopes is enrichment compensated by having slightly higher enrichment of 235U – by a combination of both to achieve equivalent reactivity to conventional enriched Enriched uranium.1,2 Reprocessed Uranium Neutronic Design › T he neutronic design of ERU FAs is designed for having the same reactivity characteristic as the equivalent con- Operational Feedback ventional enriched FA. This is achieved by the compen- sation of the 236U and other isotopes content through higher 235U enrichment (see fi g. 1 and 2). › Figure 2 shows the kinf versus the FA burn up of up to 80 MWd/kgU. Since the kinf values are very similar for ENU (enriched natural uranium) and ERU (enriched re- Fig. 2 Fig. 1 k comparison of ENU and ERU fuel versus processed uranium) fuel, the delta is shown as well in inf 235U compensation burn up – for neutronic FA design, upper the lower section. -

Jules Horowitz Reactor General Layout, Main Design Options Resulting from Safety Options, Technical Performances and Operating Constraints
TRTR-2005/IGORR-10 Joint meeting 12-16 September 2005 Gaithersburg, Maryland, USA Jules Horowitz Reactor General layout, main design options resulting from safety options, technical performances and operating constraints JP. Dupuy1, G. Perotto2 , G. Ithurralde3, C. Leydier1, X. Bravo4 1 AREVA-Technicatome, JHR Project, 1100 Av. JR Guillibert Gauthier de la Lauzière – 13791 Aix-en-Provence 2AREVA-Framatome, JHR Project, 1100 Av. JR Guillibert de la Lauzière 13791 Aix-en-Provence 3 EDF, JHR Project, 1100 Av. JR Guillibert de la Lauzière 13791 Aix-en-Provence 4COMMISSARIAT A L’ENERGIE ATOMIQUE, 13108 Saint-Paul-lez-Durance cedex, FRANCE Page 1 of 25 ABSTRACT CEA is planning to set up a new Material Testing Reactor (MTR) named the Jules Horowitz Reactor (JHR) at Cadarache (France) by 2014, as a user-facility open to European and international collaboration. The design studies of the Jules Horowitz Reactor have been subcontracted to a group which includes Technicatome (Areva Group), Framatome (Areva Group) and EDF. The JHR will be a tank pool type reactor using water as coolant and moderator. The reactor has been designed to allow irradiation with a large thermal and fast neutron fluxes required to support generation 2 and 3 reactors and to develop generation 4 technologies. It will offer large possibilities for technological irradiation needs (provisions to facilitate adaptability of reactor configuration to experimental programmes evolution, flexible experimental capacities, radio- isotopes production). A high level of safety, based on a defence-in-depth approach under best current practices, is implemented with special attention to experimental constraints. This paper presents the JHR general layout and focuses on the main design options of reactor building and nuclear auxiliaries building, resulting from technical performances, safety options and operating constraints. -

CONSOLIDATED FINANCIAL STATEMENTS Orano December 31
CONSOLIDATED FINANCIAL STATEMENTS Orano December 31, 2019 Consolidated statement of income December December (in millions of euros) Note 31, 2018 31, 2019 (*) (**) REVENUE 3,787 3,623 Cost of sales (2,991) (3,007) GROSS MARGIN 796 617 Research and development expenses (101) (97) Marketing and sales expenses (39) (38) General expenses (112) (103) Other operating income 5 107 344 Other operating expenses 5 (183) (206) OPERATING INCOME 468 517 Share in net income of joint ventures and associates 14 (19) (10) Operating income after share in net income of joint ventures and 449 506 associates Income from cash and cash equivalents 24 24 Gross borrowing costs (222) (176) Net borrowing costs 7 (198) (152) Other financial income 865 191 Other financial expenses (627) (1,017) Other financial income and expenses 7 238 (826) NET FINANCIAL INCOME 40 (978) Income tax 8 (36) (70) NET INCOME FOR THE PERIOD 452 (542) NET INCOME ATTRIBUTABLE TO OWNERS OF THE PARENT 408 (544) NET INCOME ATTRIBUTABLE TO NON-CONTROLLING 44 2 INTERESTS (*) Application of IFRS 16 as of January 1, 2019 (see Note 1.3.1). (**) The comparative figures as of December 31, 2018 have been restated to take into account the change in the presentation of end-of-lifecycle operations (see Notes 1.3.1 and 36). Orano consolidated financial statements December 31, 2019 2 Comprehensive income December December (in millions of euros) Note 31, 2019 31, 2018 (*) Net income 452 (542) Other items not recyclable to the statement of income (57) 26 Actuarial gains and losses on employee benefits (54) -
AREVA's Technology for Safety Improvement 1. INTRODUCTION 2. USEFUL TECHNICAL SOLUTIONS in CASE of SEVERE ACCIDENT
AREVA’s Technology for Safety Improvement Marina Welker Company: AREVA GmbH Address: Henri-Dunant-Str. 50, 91058 Erlangen, Germany Phone: +49 (0) 9131 900-95606 Email: [email protected] Summary – Mitigation of severe accidents in nuclear power plants (NPPs) focuses on protection of the public, the operators and plant structures/ systems. Apart from pressure reduction in the containment, also monitoring systems are required to provide the status of the plant and its equipment / systems. In addition, during severe accidents monitoring systems support the operator and authorities in making the right decisions and timely initiate the appropriate measures to mitigate the impact of a severe accident. Based on more than 30 years of experience in this field AREVA offers nuclear operators high-performance products and services to guarantee the safety of their plants. 1. INTRODUCTION Severe accidents in NPPs are linked with serious impacts on the plant itself, plant operators, the environment and the public. As Fukushima showed, they could lead to political decisions impacting the macroeconomic situation. This is another reason to pay special attention to measures which improve the safety of the plant and mitigate possible implications. In the unlikely case of a severe accident, the ability to monitor critical plant parameters and manage events becomes essential for plant operators and authorities. AREVA has developed and installed a number of dedicated technical solutions to address this need. 2. USEFUL TECHNICAL SOLUTIONS IN CASE OF SEVERE ACCIDENT 2.1. Hydrogen in the containment: generation and control In 1979 the nuclear accident of Three Miles Island directed the attention to the adverse effect on containment integrity by high H2-concentration after DBA.