General Characters of Apicomplexa
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Non-Invasive Surveillance for Plasmodium in Reservoir Macaque
Siregar et al. Malar J (2015) 14:404 DOI 10.1186/s12936-015-0857-2 METHODOLOGY Open Access Non‑invasive surveillance for Plasmodium in reservoir macaque species Josephine E. Siregar1, Christina L. Faust2*, Lydia S. Murdiyarso1, Lis Rosmanah3, Uus Saepuloh3, Andrew P. Dobson2 and Diah Iskandriati3 Abstract Background: Primates are important reservoirs for human diseases, but their infection status and disease dynamics are difficult to track in the wild. Within the last decade, a macaque malaria, Plasmodium knowlesi, has caused disease in hundreds of humans in Southeast Asia. In order to track cases and understand zoonotic risk, it is imperative to be able to quantify infection status in reservoir macaque species. In this study, protocols for the collection of non-invasive samples and isolation of malaria parasites from naturally infected macaques are optimized. Methods: Paired faecal and blood samples from 60 Macaca fascicularis and four Macaca nemestrina were collected. All animals came from Sumatra or Java and were housed in semi-captive breeding colonies around West Java. DNA was extracted from samples using a modified protocol. Nested polymerase chain reactions (PCR) were run to detect Plasmodium using primers targeting mitochondrial DNA. Sensitivity of screening faecal samples for Plasmodium was compared to other studies using Kruskal Wallis tests and logistic regression models. Results: The best primer set was 96.7 % (95 % confidence intervals (CI): 83.3–99.4 %) sensitive for detecting Plasmo- dium in faecal samples of naturally infected macaques (n 30). This is the first study to produce definitive estimates of Plasmodium sensitivity and specificity in faecal samples= from naturally infected hosts. -

Malaria History
This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike License. Your use of this material constitutes acceptance of that license and the conditions of use of materials on this site. Copyright 2006, The Johns Hopkins University and David Sullivan. All rights reserved. Use of these materials permitted only in accordance with license rights granted. Materials provided “AS IS”; no representations or warranties provided. User assumes all responsibility for use, and all liability related thereto, and must independently review all materials for accuracy and efficacy. May contain materials owned by others. User is responsible for obtaining permissions for use from third parties as needed. Malariology Overview History, Lifecycle, Epidemiology, Pathology, and Control David Sullivan, MD Malaria History • 2700 BCE: The Nei Ching (Chinese Canon of Medicine) discussed malaria symptoms and the relationship between fevers and enlarged spleens. • 1550 BCE: The Ebers Papyrus mentions fevers, rigors, splenomegaly, and oil from Balantines tree as mosquito repellent. • 6th century BCE: Cuneiform tablets mention deadly malaria-like fevers affecting Mesopotamia. • Hippocrates from studies in Egypt was first to make connection between nearness of stagnant bodies of water and occurrence of fevers in local population. • Romans also associated marshes with fever and pioneered efforts to drain swamps. • Italian: “aria cattiva” = bad air; “mal aria” = bad air. • French: “paludisme” = rooted in swamp. Cure Before Etiology: Mid 17th Century - Three Theories • PC Garnham relates that following: An earthquake caused destruction in Loxa in which many cinchona trees collapsed and fell into small lake or pond and water became very bitter as to be almost undrinkable. Yet an Indian so thirsty with a violent fever quenched his thirst with this cinchona bark contaminated water and was better in a day or two. -

Download the Abstract Book
1 Exploring the male-induced female reproduction of Schistosoma mansoni in a novel medium Jipeng Wang1, Rui Chen1, James Collins1 1) UT Southwestern Medical Center. Schistosomiasis is a neglected tropical disease caused by schistosome parasites that infect over 200 million people. The prodigious egg output of these parasites is the sole driver of pathology due to infection. Female schistosomes rely on continuous pairing with male worms to fuel the maturation of their reproductive organs, yet our understanding of their sexual reproduction is limited because egg production is not sustained for more than a few days in vitro. Here, we explore the process of male-stimulated female maturation in our newly developed ABC169 medium and demonstrate that physical contact with a male worm, and not insemination, is sufficient to induce female development and the production of viable parthenogenetic haploid embryos. By performing an RNAi screen for genes whose expression was enriched in the female reproductive organs, we identify a single nuclear hormone receptor that is required for differentiation and maturation of germ line stem cells in female gonad. Furthermore, we screen genes in non-reproductive tissues that maybe involved in mediating cell signaling during the male-female interplay and identify a transcription factor gli1 whose knockdown prevents male worms from inducing the female sexual maturation while having no effect on male:female pairing. Using RNA-seq, we characterize the gene expression changes of male worms after gli1 knockdown as well as the female transcriptomic changes after pairing with gli1-knockdown males. We are currently exploring the downstream genes of this transcription factor that may mediate the male stimulus associated with pairing. -

Extra-Intestinal Coccidians Plasmodium Species Distribution Of
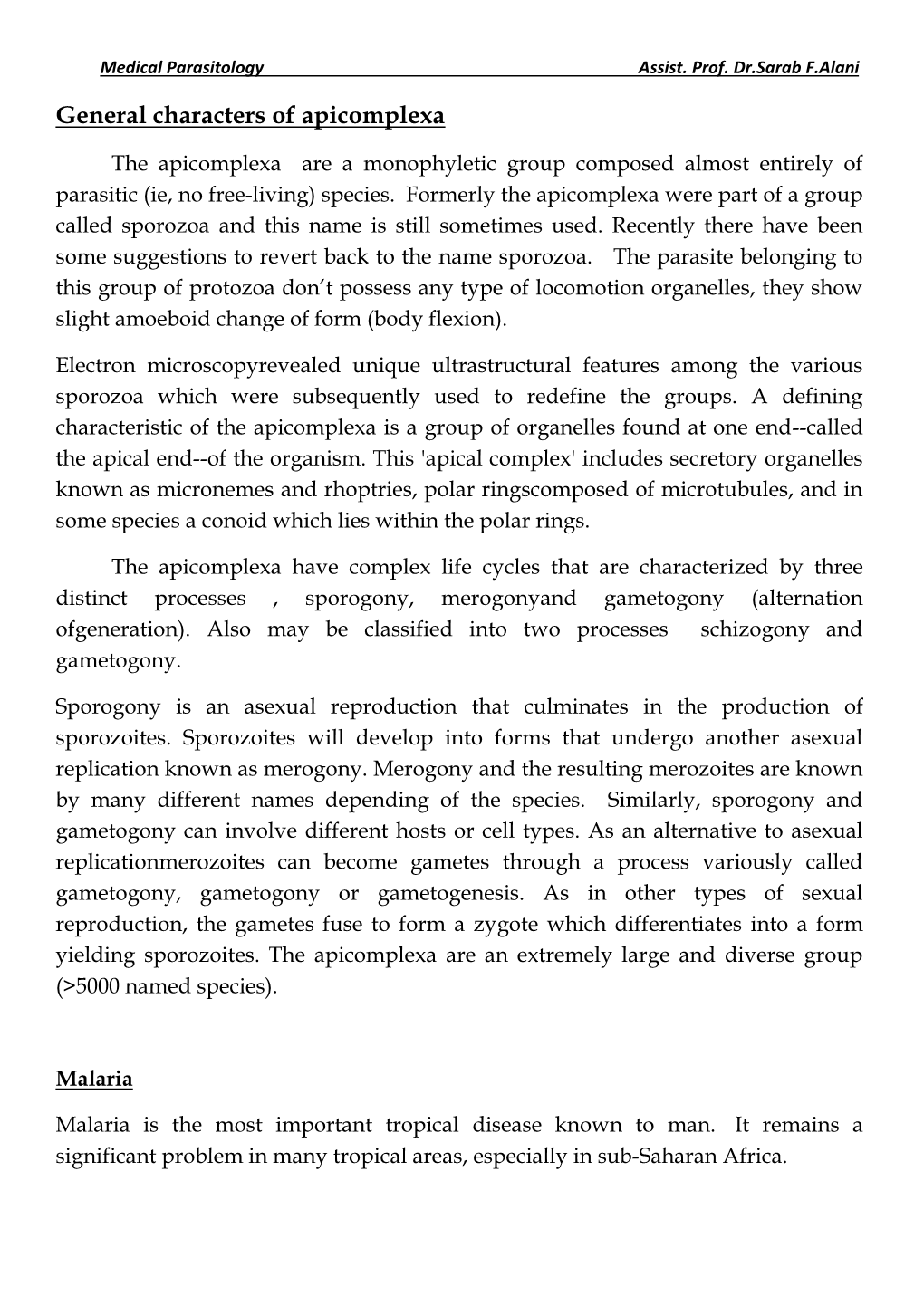
Extra-intestinal coccidians Apicomplexa Coccidia Gregarinea Piroplasmida Eimeriida Haemosporida -Eimeriidae -Theileriidae -Haemosporiidae -Cryptosporidiidae - Babesiidae (Plasmodium) -Sarcocystidae (Sacrocystis) Aconoid (Toxoplasmsa) Plasmodium species Causitive agent of Malaria ~155 species named Infect birds, reptiles, rodents, primates, humans Species is specific for host and •P. falciparum vector •P. vivax 4 species cause human disease •P. malariae No zoonoses or animal reservoirs •P. ovale Transmission by Anopheles mosquito Distribution of Malarial Parasites P. vivax most widespread, found in most endemic areas including some temperate zones P. falciparum primarily tropics and subtropics P. malariae similar range as P. falciparum, but less common and patchy distribution P. ovale occurs primarily in tropical west Africa 1 Distribution of Malaria US Army, 1943 300 - 500 million cases per year 1.5 to 2.0 million deaths per year #1 cause of infant mortality in Africa! 40% of world’s population is at risk Malaria Atlas Map Project http://www.map.ox.ac.uk/index.htm 2 Malaria in the United States Malaria was quite prevalent in the rural South It was eradicated after world war II in an aggressive campaign using, treatment, vector control and exposure control Time magazine - 1947 (along with overall improvement of living Was a widely available, conditions) cheap insecticide This was the CDCs initial DDT resistance misssion Half-life in mammals - 8 years! US banned use of DDT in 1973 History of Malaria Considered to be the most -

Sexual Development in Plasmodium Parasites: Knowing When It’S Time to Commit
REVIEWS VECTOR-BORNE DISEASES Sexual development in Plasmodium parasites: knowing when it’s time to commit Gabrielle A. Josling1 and Manuel Llinás1–4 Abstract | Malaria is a devastating infectious disease that is caused by blood-borne apicomplexan parasites of the genus Plasmodium. These pathogens have a complex lifecycle, which includes development in the anopheline mosquito vector and in the liver and red blood cells of mammalian hosts, a process which takes days to weeks, depending on the Plasmodium species. Productive transmission between the mammalian host and the mosquito requires transitioning between asexual and sexual forms of the parasite. Blood- stage parasites replicate cyclically and are mostly asexual, although a small fraction of these convert into male and female sexual forms (gametocytes) in each reproductive cycle. Despite many years of investigation, the molecular processes that elicit sexual differentiation have remained largely unknown. In this Review, we highlight several important recent discoveries that have identified epigenetic factors and specific transcriptional regulators of gametocyte commitment and development, providing crucial insights into this obligate cellular differentiation process. Trophozoite Malaria affects almost 200 million people worldwide and viewed under the microscope, it resembles a flat disc. 1 A highly metabolically active and causes 584,000 deaths annually ; thus, developing a After the ring stage, the parasite rounds up as it enters the asexual form of the malaria better understanding of the mechanisms that drive the trophozoite stage, in which it is far more metabolically parasite that forms during development of the transmissible form of the malaria active and expresses surface antigens for cytoadhesion. the intra‑erythrocytic developmental cycle following parasite is a matter of urgency. -

Phylogeny of the Malarial Genus Plasmodium, Derived from Rrna Gene Sequences (Plasmodium Falciparum/Host Switch/Small Subunit Rrna/Human Malaria)
Proc. Natl. Acad. Sci. USA Vol. 91, pp. 11373-11377, November 1994 Evolution Phylogeny of the malarial genus Plasmodium, derived from rRNA gene sequences (Plasmodium falciparum/host switch/small subunit rRNA/human malaria) ANANIAS A. ESCALANTE AND FRANCISCO J. AYALA* Department of Ecology and Evolutionary Biology, University of California, Irvine, CA 92717 Contributed by Francisco J. Ayala, August 5, 1994 ABSTRACT Malaria is among mankind's worst scourges, is only remotely related to other Plasmodium species, in- affecting many millions of people, particularly in the tropics. cluding those parasitic to birds and other human parasites, Human malaria is caused by several species of Plasmodium, a such as P. vivax and P. malariae. parasitic protozoan. We analyze the small subunit rRNA gene sequences of 11 Plasmodium species, including three parasitic to humans, to infer their evolutionary relationships. Plasmo- MATERIALS AND METHODS dium falciparum, the most virulent of the human species, is We have investigated the 18S SSU rRNA sequences ofthe 11 closely related to Plasmodium reiehenowi, which is parasitic to Plasmodium species listed in Table 1. This table also gives chimpanzee. The estimated time of divergence of these two the known host and geographical distribution. The sequences Plasmodium species is consistent with the time of divergence are for type A genes, which are expressed during the asexual (6-10 million years ago) between the human and chimpanzee stage of the parasite in the vertebrate host, whereas the SSU lineages. The falkiparun-reichenowi lade is only remotely rRNA type B genes are expressed during the sexual stage in related to two other human parasites, Plasmodium malariae the vector (12). -

The Historical Ecology of Human and Wild Primate Malarias in the New World
Diversity 2010, 2, 256-280; doi:10.3390/d2020256 OPEN ACCESS diversity ISSN 1424-2818 www.mdpi.com/journal/diversity Article The Historical Ecology of Human and Wild Primate Malarias in the New World Loretta A. Cormier Department of History and Anthropology, University of Alabama at Birmingham, 1401 University Boulevard, Birmingham, AL 35294-115, USA; E-Mail: [email protected]; Tel.: +1-205-975-6526; Fax: +1-205-975-8360 Received: 15 December 2009 / Accepted: 22 February 2010 / Published: 24 February 2010 Abstract: The origin and subsequent proliferation of malarias capable of infecting humans in South America remain unclear, particularly with respect to the role of Neotropical monkeys in the infectious chain. The evidence to date will be reviewed for Pre-Columbian human malaria, introduction with colonization, zoonotic transfer from cebid monkeys, and anthroponotic transfer to monkeys. Cultural behaviors (primate hunting and pet-keeping) and ecological changes favorable to proliferation of mosquito vectors are also addressed. Keywords: Amazonia; malaria; Neotropical monkeys; historical ecology; ethnoprimatology 1. Introduction The importance of human cultural behaviors in the disease ecology of malaria has been clear at least since Livingstone‘s 1958 [1] groundbreaking study describing the interrelationships among iron tools, swidden horticulture, vector proliferation, and sickle cell trait in tropical Africa. In brief, he argued that the development of iron tools led to the widespread adoption of swidden (―slash and burn‖) agriculture. These cleared agricultural fields carved out a new breeding area for mosquito vectors in stagnant pools of water exposed to direct sunlight. The proliferation of mosquito vectors and the subsequent heavier malarial burden in human populations led to the genetic adaptation of increased frequency of sickle cell trait, which confers some resistance to malaria. -

New Insights Into Clonality and Panmixia in Plasmodium and Toxoplasma
UC Irvine UC Irvine Previously Published Works Title New insights into clonality and panmixia in Plasmodium and toxoplasma. Permalink https://escholarship.org/uc/item/5vs7c363 Journal Advances in parasitology, 84 ISSN 0065-308X Authors Tibayrenc, Michel Ayala, Francisco J Publication Date 2014 DOI 10.1016/b978-0-12-800099-1.00005-3 Peer reviewed eScholarship.org Powered by the California Digital Library University of California CHAPTER FIVE New Insights into Clonality and Panmixia in Plasmodium and Toxoplasma Michel Tibayrenc*,1, Francisco J. Ayala† *Maladies Infectieuses et Vecteurs Ecologie, Ge´ne´tique, Evolution et Controˆle, MIVEGEC (IRD 224-CNRS 5290-UM1-UM2), IRD Center, Montpellier, France †Department of Ecology and Evolutionary Biology, University of California, Irvine, California, USA 1Correponding author: e-mail address: [email protected] Contents 1. Introduction 254 2. Initial Proposals 255 3. Indispensable Recalls 255 4. Recent Developments 256 5. Population Structure of Plasmodium and Toxoplasma in the Light of the PCE Model 258 5.1 Plasmodium 258 5.2 Toxoplasma 259 6. Passive Clonality (Starving Sex) Versus In-Built Clonality in Plasmodium 260 7. Are Clonality and Near-Clading in Plasmodium and Toxoplasma Mainly Due to Natural Selection? 262 8. Are the New Plasmodium “Species” Not Mere Near-Clades? 262 9. Concluding Remarks 263 Acknowledgement 264 References 264 Abstract Until the 1990s, Plasmodium and Toxoplasma were widely considered to be potentially panmictic species, because they both undergo a meiotic sexual cycle in their definitive hosts. We have proposed that both parasites are able of clonal (nonrecombining) prop- agation, at least in some cycles. Toxoplasma was soon shown to be a paradigmatic case of clonal population structure in North American and in European cycles. -

Plasmodium Malariae and P. Ovale Genomes Provide Insights Into Malaria Parasite Evolution Gavin G
OPEN LETTER doi:10.1038/nature21038 Plasmodium malariae and P. ovale genomes provide insights into malaria parasite evolution Gavin G. Rutledge1, Ulrike Böhme1, Mandy Sanders1, Adam J. Reid1, James A. Cotton1, Oumou Maiga-Ascofare2,3, Abdoulaye A. Djimdé1,2, Tobias O. Apinjoh4, Lucas Amenga-Etego5, Magnus Manske1, John W. Barnwell6, François Renaud7, Benjamin Ollomo8, Franck Prugnolle7,8, Nicholas M. Anstey9, Sarah Auburn9, Ric N. Price9,10, James S. McCarthy11, Dominic P. Kwiatkowski1,12, Chris I. Newbold1,13, Matthew Berriman1 & Thomas D. Otto1 Elucidation of the evolutionary history and interrelatedness of human parasite P. falciparum than in its chimpanzee-infective relative Plasmodium species that infect humans has been hampered by a P. reichenowi8. In both cases, the lack of diversity in human-infective lack of genetic information for three human-infective species: P. species suggests recent population expansions. However, we found malariae and two P. ovale species (P. o. curtisi and P. o. wallikeri)1. that a species that infects New World primates termed P. brasilianum These species are prevalent across most regions in which malaria was indistinguishable from P. malariae (Extended Data Fig. 2b), as is endemic2,3 and are often undetectable by light microscopy4, previously suggested9. Thus host adaptation in the P. malariae lineage rendering their study in human populations difficult5. The exact appears to be less restricted than in P. falciparum. evolutionary relationship of these species to the other human- Using additional samples to calculate standard measures of molecular infective species has been contested6,7. Using a new reference evolution (Methods; Supplementary Information), we identified a genome for P. -

Prevalence of Malaria, Typhoid, Toxoplasmosis and Rubella Among Febrile Children in Cameroon Olivia A
Achonduh-Atijegbe et al. BMC Infectious Diseases (2016) 16:658 DOI 10.1186/s12879-016-1996-y RESEARCH ARTICLE Open Access Prevalence of malaria, typhoid, toxoplasmosis and rubella among febrile children in Cameroon Olivia A. Achonduh-Atijegbe1,2*, Kenji O. Mfuh3, Aristid H. E. Mbange1, Jean P. Chedjou1, Diane W. Taylor2,3, Vivek R. Nerurkar2,3, Wilfred F. Mbacham1 and Rose Leke1,2 Abstract Background: The current roll-out of rapid diagnostic tests (RDTs) in many endemic countries has resulted in the reporting of fewer cases of malaria-attributed illnesses. However, lack of knowledge of the prevalence of other febrile illnesses and affordable diagnostic tests means that febrile patients are not managed optimally. This study assessed the prevalence of commonly treatable or preventable febrile illnesses in children between 6 months and 15 years using rapid diagnostic tests at the point-of-care. Methods: Febrile children were enrolled between February-April 2014 at a health facility after obtaining informed consent from parent. Eligible participants were aged 6 months-15 years with a history of fever in the last 24 h or axillary temperature ≥38 °C at consultation. All participants were tested using RDTs for malaria, typhoid, toxoplasmosis and rubella. Malaria parasites were further identified by microscopy and PCR. Clinical and household characteristics were recorded and association with pathogens determined. Results: Of the 315 children enrolled, the mean age was 5.8 ± 3.8 years. Stomach pain (41.2 %) was the most reported symptom. Prior to attending the health facility, 70.8 % had taken antipyretics, 27.9 % antimalarials, 11.4 % antibiotics and 13.3 % antifungal drugs. -

"Plasmodium". In: Encyclopedia of Life Sciences (ELS)
Plasmodium Advanced article Lawrence H Bannister, King’s College London, London, UK Article Contents . Introduction and Description of Plasmodium Irwin W Sherman, University of California, Riverside, California, USA . Plasmodium Hosts Based in part on the previous version of this Encyclopedia of Life Sciences . Life Cycle (ELS) article, Plasmodium by Irwin W Sherman. Asexual Blood Stages . Intracellular Asexual Blood Parasite Stages . Sexual Stages . Mosquito Asexual Stages . Pre-erythrocytic Stages . Metabolism . The Plasmodium Genome . Motility . Recent History of Plasmodium Research . Evolution of Plasmodium . Conclusion Online posting date: 15th December 2009 Plasmodium is a genus of parasitic protozoa which infect Introduction and Description of erythrocytes of vertebrates and cause malaria. Their life cycle alternates between mosquito and vertebrate hosts. Plasmodium Parasites enter the bloodstream after a mosquito bite, Parasites of the genus Plasmodium are protozoans which and multiply sequentially within liver cells and erythro- invade and multiply within erythrocytes of vertebrates, and cytes before becoming male or female sexual forms. When are transmitted by mosquitoes. The motile invasive stages ingested by a mosquito, these fuse, then the parasite (merozoite, ookinete and sporozoite) are elongate, uni- multiplies again to form more invasive stages which are nucleate cells able to enter cells or pass through tissues, transmitted back in the insect’s saliva to a vertebrate. All using specialized secretory and locomotory organelles. -

Classification and Nomenclature of Human Parasites Lynne S
C H A P T E R 2 0 8 Classification and Nomenclature of Human Parasites Lynne S. Garcia Although common names frequently are used to describe morphologic forms according to age, host, or nutrition, parasitic organisms, these names may represent different which often results in several names being given to the parasites in different parts of the world. To eliminate same organism. An additional problem involves alterna- these problems, a binomial system of nomenclature in tion of parasitic and free-living phases in the life cycle. which the scientific name consists of the genus and These organisms may be very different and difficult to species is used.1-3,8,12,14,17 These names generally are of recognize as belonging to the same species. Despite these Greek or Latin origin. In certain publications, the scien- difficulties, newer, more sophisticated molecular methods tific name often is followed by the name of the individual of grouping organisms often have confirmed taxonomic who originally named the parasite. The date of naming conclusions reached hundreds of years earlier by experi- also may be provided. If the name of the individual is in enced taxonomists. parentheses, it means that the person used a generic name As investigations continue in parasitic genetics, immu- no longer considered to be correct. nology, and biochemistry, the species designation will be On the basis of life histories and morphologic charac- defined more clearly. Originally, these species designa- teristics, systems of classification have been developed to tions were determined primarily by morphologic dif- indicate the relationship among the various parasite ferences, resulting in a phenotypic approach.