Health and Wellbeing in Glasgow and the Gowell Areas – Deprivation Based Analyses
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Scotstoun Sports Campus
July 2014 Version 3 SCOTSTOUN SPORTS CAMPUS Essential Venue Guide Scotstoun Sports Campus’ brand new courts – six for Squash, with a glass-walled show court; eight plus two show courts for Table Tennis – will give audiences a fantastic view of the action. At Scotstoun Sports Campus For everyone’s safety and enjoyment of the event, all spectators will pass through an airport style screening process for prohibited and restricted items before being allowed into venues. Facilities Advice Regulations Important information – Spectator Information Point, including – Plan your journey now. Make sure – Bringing a bag may slow down your – Alchohol can be purchased from the induction hearing loop, wheelchair you know how to reach the venue entry. Each spectator is permitted food & drink kiosks, but may not be loan, wheelchair pushing service, and allow plenty of time for travel, one small bag no larger than 25 litres brought into the venue from outside. pushchair & wheelchair storage, queuing systems at transport hubs, (equivalent to 30 x 20 x 20 cm/12” x and Lost & Found service for people and security checks. 8” x 8”). It must be soft sided and fit – All containers of liquids, aerosols or and property. under your seat. gels – except sunscreen (200ml) and – Use public transport – do not non-alcoholic drinks (500ml) – must be – Accessible toilets and Changing drive to the venue. Except limited – Spectators with a wheelchair ticket 100ml or under in volume. Places toilet. pre-bookable facilities for Blue Badge can bring a wheelchair into the holders, there will be no parking or seating area. All other ticketholders – You can bring a plastic water bottle of – Assistance dog spending & water set-down/pick-up points for private with wheelchairs, prams or pushchairs 500ml or under. -
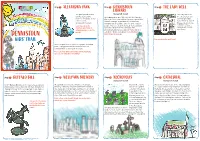
DENNISTOUN Stop 3 the LADY WELL LIBRARY the Park Opened in 1870 (Category B-Listed) the Lady Well Is on and Was Named After the Library Opened in 1905
Stop 1 ALEXANDRA PARK Stop 2 DENNISTOUN Stop 3 THE LADY WELL LIBRARY The park opened in 1870 (Category B-listed) The Lady Well is on and was named after The Library opened in 1905. It is called a Carnegie the site of an ancient Princess Alexandra. At the Library because it was built using money donated by well that provided entrance is the Andrew Carnegie, a man born in Scotland who water for the people of Cruikshank Fountain. moved to America and became one of the richest Glasgow before it was common to have Look closely at the people who ever lived. He donated money to build running water inside fountain, what kind of over 2000 libraries across the world. The your home. animal do you see on the Dennistoun Library has a special statue which is inside? called the “Dennistoun Angel”. Can you find it? DENNISTOUN Don’t forget to look up! KIDS’ TRAIL Can you draw the well here? Inside the park there is lots to see and do, including ponds, a playground and the beautiful Saracen Fountain which is over 12 metres tall! There are four different statues on the fountain, can you see what they’re holding? Stop 4 BUFFALO BILL Stop 5 WELLPARK BREWERY Stop 6 NECROPOLIS Stop 7 CATHEDRAL (Category A-listed) (Category A-listed) In 1891 Buffalo Bill, One of the most famous and well Wellpark Brewery was first known as the Drygate Glasgow Necropolis Glasgow Cathedral is one of the oldest buildings known figures of the American Old West, brought his Brewery, a brewery is a place where beer is made.It was the first garden in Glasgow and the only mediaeval cathedral in “Wild West Show” to the very spot where his statue is was founded in 1740 by Hugh and Robert Tennent but cemetery in Scotland. -

Glasgow City Community Health Partnership Service Directory 2014 Content Page
Glasgow City Community Health Partnership Service Directory 2014 Content Page About the CHP 1 Glasgow City CHP Headquarters 2 North East Sector 3 North West Sector 4 South Sector 5 Adult Protection 6 Child Protection 6 Emergency and Out-of-Hours care 6 Addictions 7 - 9 Asylum Seekers 9 Breast Screening 9 Breastfeeding 9 Carers 10 - 12 Children and Families 13 - 14 Dental and Oral Health 15 Diabetes 16 Dietetics 17 Domestic Abuse / Violence 18 Employability 19 - 20 Equality 20 Healthy Living 21 Health Centres 22 - 23 Hospitals 24 - 25 Housing and Homelessness 26 - 27 Learning Disabilities 28 - 29 Mental Health 30 - 40 Money Advice 41 Nursing 41 Physiotherapy 42 Podiatry 42 Respiratory 42 Rehabilitation Services 43 Sexual Health 44 Rape and Sexual Assault 45 Stop Smoking 45 Transport 46 Volunteering 46 Young People 47-49 Public Partnership Forum 50 Comments and Complaints 51-21 About Glasgow City Community Health Partnership Glasgow City Community Health Partnership (GCCHP) was established in November 2010 and provides a wide range of community based health services delivered in homes, health centres, clinics and schools. These include health visiting, health improvement, district nursing, speech and language therapy, physiotherapy, podiatry, nutrition and dietetic services, mental health, addictions and learning disability services. As well as this, we host a range of specialist services including: Specialist Children’s Services, Homeless Services and The Sandyford. We are part of NHS Greater Glasgow & Clyde and provide services for 584,000 people - the entire population living within the area defined by the LocalAuthority boundary of Glasgow City Council. Within our boundary, we have: 154 GP practices 136 dental practices 186 pharmacies 85 optometry practices (opticians) The CHP has more than 3,000 staff working for it and is split into three sectors which are aligned to local social work and community planning boundaries. -

North West Sector Profile
Appendix North West Sector Profile Contents 1. Introduction Page 1 2. Executive Summary Page 2 3. Demographic & Socio – Economic Page 8 4. Labour Market/Employment/Education Page 13 5. Health Page 23 6. Neighbourhood Management Page 29 1. Introduction 1.1 The profile provides comparative information on the North West Sector Community Planning Partnership (CPP) area, including demographic & socio economic, employment, health and neighbourhood management information. 1.2 North West Glasgow is diverse in socio economic terms, as illustrated by the map, as it contains Glasgow’s city centre/ business area, the more affluent west end of Glasgow but also localities with significant issues relating to employment, health and poverty. The North West is the academic centre of the City with the three Glasgow Universities located in the sector and also has many cultural & historical buildings of interest as well as large areas of green space. Table 1: North West Sector Summary Population (2011 Census) 206,483 (up 7.1%) Population (2011 Census) exc. communal establishments 197,419 Working Age Population 16-64 (2011 Census) 151,345 (73.3%) Electorate (2014) 165,009 Occupied Households (2011 Census) 101,884 (up 9.5%) Average Household Size (2011) exc. communal establishments 1.94 (2.07 in 2011) Housing Stock (2014) 105,638 No. of Dwellings per Hectare (2012) 22.28 Out Of Work Benefit Claimants (May 2014) 24,230 (16.0%) Job Seekers Allowance (February 2015) 5,141 (3.4%) 2. Executive Summary Demographic Information 2.1 Population According to the 2011 Census, The North West sector population was 206,483. The population in the North West Sector increased by 13,773 (7.1%) from 2001 Census. -

Life Expectancy Trends Within Glasgow, 2001-2009
Glasgow: health in a changing city a descriptive study of changes in health, demography, housing, socioeconomic circumstances and environmental factors in Glasgow over the last 20 years Bruce Whyte March 2016 Contents Acknowledgements 3 Abbreviations/glossary 3 Executive summary 7 1. Introduction 9 2. Background 10 3. Aims and methods 14 4. An overview of changes in demography, housing, socioeconomic circumstances and environmental factors in Glasgow 17 5. Changes in life expectancy in Glasgow 38 6. Discussion 52 7. Policy implications 57 8. Conclusions 61 Appendices 62 References 65 2 Acknowledgements I would like to thank Craig Waugh and Lauren Schofield (both of ISD Scotland) who helped produce the GCPH’s local health profiles for Glasgow. Much of the data shown or referred to in this report has been drawn from the profiles. Thank you also to Ruairidh Nixon who summarised trends in key health and social indicators in an internal GCPH report; some of that work is incorporated in this report. I would also like to thank Alan MacGregor (DRS, Glasgow City Council), who provided data on housing tenure, completions and demolitions. I am grateful to my colleagues at the GPCH who have commented on this work as it has developed, in particular, Carol Tannahill, David Walsh, Sara Dodds, Lorna Kelly and Joe Crossland. I would also like to thank Jan Freeke (DRS, Glasgow City Council) who commented on drafts of the report. Members of the GCPH Management Board have also provided useful advice and comments at various stages in the analysis. 3 Abbreviations/glossary Organisations DRS Development and Regeneration Services. -

Glasgow City Health and Social Care Partnership Health Contacts
Glasgow City Health and Social Care Partnership Health Contacts January 2017 Contents Glasgow City Community Health and Care Centre page 1 North East Locality 2 North West Locality 3 South Locality 4 Adult Protection 5 Child Protection 5 Emergency and Out-of-Hours care 5 Addictions 6 Asylum Seekers 9 Breast Screening 9 Breastfeeding 9 Carers 10 Children and Families 12 Continence Services 15 Dental and Oral Health 16 Dementia 18 Diabetes 19 Dietetics 20 Domestic Abuse 21 Employability 22 Equality 23 Health Improvement 23 Health Centres 25 Hospitals 29 Housing and Homelessness 33 Learning Disabilities 36 Maternity - Family Nurse Partnership 38 Mental Health 39 Psychotherapy 47 NHS Greater Glasgow and Clyde Psychological Trauma Service 47 Money Advice 49 Nursing 50 Older People 52 Occupational Therapy 52 Physiotherapy 53 Podiatry 54 Rehabilitation Services 54 Respiratory Team 55 Sexual Health 56 Rape and Sexual Assault 56 Stop Smoking 57 Volunteering 57 Young People 58 Public Partnership Forum 60 Comments and Complaints 61 Glasgow City Community Health & Care Partnership Glasgow Health and Social Care Partnership (GCHSCP), Commonwealth House, 32 Albion St, Glasgow G1 1LH. Tel: 0141 287 0499 The Management Team Chief Officer David Williams Chief Officer Finances and Resources Sharon Wearing Chief Officer Planning & Strategy & Chief Social Work Officer Susanne Miller Chief Officer Operations Alex MacKenzie Clincial Director Dr Richard Groden Nurse Director Mari Brannigan Lead Associate Medical Director (Mental Health Services) Dr Michael Smith -

Reopening of Selected Venues for Essential Services
REOPENING OF SELECTED VENUES FOR ESSENTIAL SERVICES Updated Wednesday 12 August to include revised reopening dates for selected venues. All dates below are based on the Scottish Government’s route map. They are indicative and subject to change. PROPOSED DATE VENUE PURPOSE OF REOPENING JULY Childcare provision (tenant) and Education Barlanark Community Centre use of sports hall Bellcraig Community Centre Childcare provision Week beginning Monday Castlemilk Community Centre Childcare provision (tenant) 20 July Easterhouse Campus Food distribution programme (tenant) Glasgow Museums Resource Staff access Centre Kelvin Hall Key tenant access Week beginning Monday 27 July Scotstoun Stadium Key tenant access AUGUST Glasgow Life Head Office, Staff access Albion Street Geoff Shaw Community Centre Staff access and childcare provision Week beginning Monday Govanhill Community Centre Childcare provision 3 August Darnley Community Centre Childcare provision Maryhill Community Centre Childcare provision Penilee Community Centre Childcare provision (tenant) Ruchazie Community Centre Childcare provision Week beginning Monday Glasgow Royal Concert Hall Staff and key tenant access 3 August cont. City Halls and Old Fruitmarket Staff and key tenant access Kelvingrove Art Gallery and Staff access Museum Essential staff supporting the GSOS student Glasgow School of Sport programme Tramway Staff access Glasgow Club Drumoyne Education use Week beginning Monday Glasgow Club Haghill Education use 10 August Glasgow Club Holyrood Education use Glasgow Club John Paul Education use Milton Community Campus Education use Riverside Museum Staff access Week beginning Monday 17 August Emirates Arena Staff access SEPTEMBER Week beginning Monday Gallery of Modern Art Staff access 14 September Week beginning Monday Mitchell Library Staff access 21 September . -

Greater Glasgow & the Clyde Valley
What to See & Do 2013-14 Explore: Greater Glasgow & The Clyde Valley Mòr-roinn Ghlaschu & Gleann Chluaidh Stylish City Inspiring Attractions Discover Mackintosh www.visitscotland.com/glasgow Welcome to... Greater Glasgow & The Clyde Valley Mòr-roinn Ghlaschu & Gleann Chluaidh 01 06 08 12 Disclaimer VisitScotland has published this guide in good faith to reflect information submitted to it by the proprietor/managers of the premises listed who have paid for their entries to be included. Although VisitScotland has taken reasonable steps to confirm the information contained in the guide at the time of going to press, it cannot guarantee that the information published is and remains accurate. Accordingly, VisitScotland recommends that all information is checked with the proprietor/manager of the business to ensure that the facilities, cost and all other aspects of the premises are satisfactory. VisitScotland accepts no responsibility for any error or misrepresentation contained in the guide and excludes all liability for loss or damage caused by any reliance placed on the information contained in the guide. VisitScotland also cannot accept any liability for loss caused by the bankruptcy, or liquidation, or insolvency, or cessation of trade of any company, firm or individual contained in this guide. Quality Assurance awards are correct as of December 2012. Rodin’s “The Thinker” For information on accommodation and things to see and do, go to www.visitscotland.com at the Burrell Collection www.visitscotland.com/glasgow Contents 02 Glasgow: Scotland with style 04 Beyond the city 06 Charles Rennie Mackintosh 08 The natural side 10 Explore more 12 Where legends come to life 14 VisitScotland Information Centres 15 Quality Assurance 02 16 Practical information 17 How to read the listings Discover a region that offers exciting possibilities 17 Great days out – Places to Visit 34 Shopping every day. -
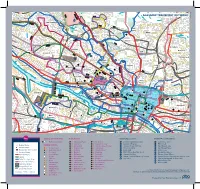
Campus Travel Guide Final 08092016 PRINT READY
Lochfauld V Farm ersion 1.1 27 Forth and 44 Switchback Road Maryhill F C Road 6 Clyde Canal Road Balmore 1 0 GLASGOW TRANSPORT NETWORK 5 , 6 F 61 Acre0 A d Old Blairdardie oa R Drumchapel Summerston ch lo 20 til 23 High Knightswood B irkin e K F 6 a /6A r s de F 15 n R F 8 o Netherton a High d 39 43 Dawsholm 31 Possil Forth and Clyde Canal Milton Cadder Temple Gilshochill a 38 Maryhill 4 / 4 n F e d a s d /4 r a 4 a o F e River Lambhill R B d Kelvin F a Anniesland o 18 F 9 0 R 6 n /6A 1 40 r 6 u F M 30 a b g Springburn ry n h 20 i ill r R Ruchill p Kelvindale S Scotstounhill o a Balornock 41 d Possil G Jordanhill re Park C at 19 15 W es 14 te rn R 17 37 oa Old Balornock 2 d Forth and D um Kelvinside 16 Clyde b North art 11 Canal on Kelvin t Ro Firhill ad 36 ee 5 tr 1 42 Scotstoun Hamiltonhill S Cowlairs Hyndland 0 F F n e 9 Broomhill 6 F ac 0 r Maryhill Road V , a ic 6 S Pa tor Dowanhill d r ia a k D 0 F o S riv A 8 21 Petershill o e R uth 8 F 6 n F /6 G r A a u C 15 rs b R g c o u n Whiteinch a i b r 7 d e Partickhill F 4 p /4 S F a River Kelvin F 9 7 Hillhead 9 0 7 River 18 Craighall Road Port Sighthill Clyde Partick Woodside Forth and F 15 Dundas Clyde 7 Germiston 7 Woodlands Renfrew Road 10 Dob Canal F bie' 1 14 s Loa 16 n 5 River Kelvin 17 1 5 F H il 7 Pointhouse Road li 18 5 R n 1 o g 25A a t o Shieldhall F 77 Garnethill d M 15 n 1 14 M 21, 23 10 M 17 9 6 F 90 15 13 Alexandra Parade 12 0 26 Townhead 9 8 Linthouse 6 3 F Govan 33 16 29 Blyt3hswood New Town F 34, 34a Anderston © The University of Glasgo North Stobcross Street Cardonald -

Glasgow to Easterhouse and Coatbridge Cycle Route the Monkland Cycle Route
GLASGOW TO EASTERHOUSE AND COATBRIDGE CYCLE ROUTE THE MONKLAND CYCLE ROUTE (Updated June 2009) EXECUTIVE SUMMARY • Buchanan Bus Station to Coatbridge Fountain without cycling on any main roads! • Serves Glasgow City Centre, Caledonian University, Buchanan Bus Station, Strathclyde University, Royal Infirmary, Alexandra Park, Cranhill Park, Blairtummock Industrial Estate, Glasgow Fort Shopping Centre, Blairtummock Park, Monkland Canal, Drumpellier Country Park, The Time Capsule, Coatbridge Town Centre, plus numerous schools and local shopping areas • Large catchment area serving North East Glasgow, not presently served by any cycle route • Links Glasgow City Centre, Roystonhill, North Dennistoun, North Carntyne, Cranhill, Queenslie, Garthamlock, Easthall, Easterhouse, North Bargeddie, Drumpellier, Coatbridge Town Centre • Connects with existing Colleges Cycle Route, Glasgow to Cumbernauld Cycle Route, National Cycle Network Route 75, the Garthamlock ramp (currently under design), plus potential links to various communities near route • Potential candidate for Sustrans “Regional Cycle Network” route status, thus allowing route to be marked on Ordnance Survey maps • Utilises existing paths and quiet roads over most of route • Limited construction work required to link up existing infrastructure • Caters for those cyclists not catered for by Quality Bus Corridor (Streamline) routes • Reasonably direct route, parallel to M8 motorway Go Bike! Strathclyde Cycle Campaign • PO Box 15175 • Glasgow • G4 9LP • www.gobike.org GLASGOW TO EASTERHOUSE AND COATBRIDGE CYCLE ROUTE THE MONKLAND CYCLE ROUTE Route description: Starting at George Square in Glasgow City Centre, the route proceeds via Townhead, Roystonhill, North Dennistoun, Alexandra Park, North Carntyne, Cranhill, Queenslie, Easthall, Blairtummock Park, North Bargeddie, and the Monkland Canal to Coatbridge Town Centre. There are also links to Greenfield Park from North Carntyne, and to the Glasgow Fort and Easterhouse Shopping Centres. -

Download Download
Scottish Tradition Vol. 27 2002 WORKING CLASS CULTURE, FAMILY LIFE AND DOMESTIC VIOLENCE ON CLYDESIDE, C 1918-1939: A VIEW FROM BELOW. ‘People have no idea how the poor lived in those days. They seemed to be at loggerheads all the time.’ 1 he inter-war years were distinguished by marked changes that affected the lives and neighbourhoods of Tmany working class men and women. These changes would prove to have positive and negative implications for working-class family life. New employment opportunities extended the breadth of jobs open to working class people, espe- cially in the new consumer industries that employed significant numbers of women. Correspondingly, the commercialisation of leisure expanded the possibilities of pleasure. Information on birth control and the greater ease of availability of contraceptives also offered a better potential to postpone marriage and reduce family size. Yet, the new employment opportunities did little to alter the ‘pin money’ wages of women and women’s economic dependency on marriage. Marriage was still seen as an attractive alternative to employment in the longer term.2 Marriage and motherhood were actively promoted as the natural and fulfilling aspirations for women by the state, state agencies, the clergy, religious organisations and the media. Adding to the appeal was the ideal of the ‘companionate marriage’ in which husbands were expected to share chores, child-care, leisure and provide love and companionship. It seems that this was a ‘fairly norma- tive’ aspiration amongst many sectors of the working class between the wars, at least amongst women. Change, however, was not just ideological.3 After World War I, the building of ‘homes fit for heroes’ and the growth of ‘new garden cities’, were linked with ideals of the companionate marriage, maternalism, privacy, respectable domesticity and the growth of male home- centred pastimes. -

Hillington SPZ Landscape & Visual Appraisal 2014
HILLINGTON PARK LANDSCAPE AND VISUAL APPRAISAL MEPC FEBRUARY 2014 Hillington Park: Landscape and Visual Appraisal MEPC Ltd Document Control Sheet Project Title HILLINGTON PARK SIMPLIFIED PLANNING ZONE Document Title Landscape and Visual Appraisal Revision Status FINAL Control Date February 2014 Document Reference 199304/Doc1 © Terence O’Rourke Ltd 2014. All rights reserved. No part of this document may be reproduced in any form or stored in a retrieval system without the prior written consent of the copyright holder. Hillington Park: Landscape and Visual Appraisal MEPC Ltd Contents 1. Introduction 2. Legislation and policy 3. SPZ area context 4. Landscape appraisal 5. Development parameters 6. Landscape strategy 7. Effects on landscape character and views 8. Summary Figures Figure 1. Topography Figure 2. Environmental designations Figure 3. Landscape character areas Figure 4. Zone of visual influence Figure 5. Viewpoint locations Figure 6. Viewpoint 1 Figure 7. Viewpoint 2 Figure 8. Viewpoint 3 Figure 9. Viewpoint 4 Figure 10. Viewpoint 5 Figure 11. Viewpoint 6 Figure 12. Viewpoint 7 Figure 13. Viewpoint 8 Figure 14. Viewpoint 9 Figure 15. Viewpoint 10 Figure 16. Viewpoint 11 Figure 17. Viewpoint 12 Hillington Park: Landscape and Visual Appraisal MEPC Ltd 1 Introduction 1. Terence O’Rourke Ltd has been instructed by MEPC Hillington Park to undertake a Landscape and Visual Appraisal for Hillington Park, Glasgow to inform the preparation of a Simplified Planning Zone for the industrial estate. The Hillington Park Simplified Planning Zone (SPZ) is a partnership between Renfrewshire Council and Glasgow City Council, as the local planning authorities, and MEPC Hillington Park as the majority landowner.