The Microbiology of Respiratory System Infections
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Redalyc.Significance of Specific Igg Against Sensitizing Antigens In
Revista Portuguesa de Pneumología ISSN: 0873-2159 [email protected] Sociedade Portuguesa de Pneumologia Portugal Sterclova, M.; Vasakova, M.; Metlicka, M. Significance of specific IgG against sensitizing antigens in extrinsic allergic alveolitis: Serological methods in EAA Revista Portuguesa de Pneumología, vol. 17, núm. 6, noviembre-diciembre, 2011, pp. 253-259 Sociedade Portuguesa de Pneumologia Lisboa, Portugal Available in: http://www.redalyc.org/articulo.oa?id=169722769004 How to cite Complete issue Scientific Information System More information about this article Network of Scientific Journals from Latin America, the Caribbean, Spain and Portugal Journal's homepage in redalyc.org Non-profit academic project, developed under the open access initiative Documento descarregado de http://www.elsevier.pt el 21/05/2012. Cópia para uso pessoal, está totalmente proibida a transmissão deste documento por qualquer meio ou forma. Rev Port Pneumol. 2011;17(6):253---259 www.revportpneumol.org ORIGINAL ARTICLE Significance of specific IgG against sensitizing antigens in extrinsic allergic alveolitis: Serological methods in EAA M. Sterclova a,∗, M. Vasakova b, M. Metlicka b a Department of Respiratory Diseases, Thomayer’s University Hospital, Videnska, Prague, Czech Republic b Department of Immunology, Thomayer’s University Hospital, Videnska, Prague, Czech Republic Received 23 December 2010; accepted 20 June 2011 Available online 16 September 2011 KEYWORDS Abstract The aim of our study is to find differences in IgG in sera of potentially exposed and Aeroallergen; nonexposed individuals and to detect differences in concentrations of specific serum IgG among Hypersensitivity subjects with and without EAA. pneumonitis; Seventy-two patients being followed for suspected interstitial lung disease were included. -

Enteric Viruses Nucleic Acids Distribution Along the Digestive Tract of Rhesus Macaques with Idiopathic Chronic Diarrhea
bioRxiv preprint doi: https://doi.org/10.1101/2021.06.24.449827; this version posted June 24, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. Enteric viruses nucleic acids distribution along the digestive tract of rhesus macaques with idiopathic chronic diarrhea Eric Delwart1,2*, David Merriam3,4, Amir Ardeshir3, Eda Altan1,2, Yanpeng Li1,2, Xutao Deng,1,2, J. Dennis Hartigan-O’Connor3 1. Vitlant Research Institute, 270 Masonic Ave, San Francisco CA94118 2. Dept of Laboratory Medicine, UCSF, San Francisco CA94118 3. California National Primate Research Center, University of California, Davis, CA 95616 4. Department of Pediatric Infectious Diseases, University of Colorado School of Medicine, Aurora, CO, USA. * Communicating author: [email protected] Abstract: Idiopathic chronic diarrhea (ICD) is a common clinical condition in captive rhesus macaques, claiming 33% of medical culls (i.e. deaths unrelated to research). Using viral metagenomics we characterized the eukaryotic virome in digestive tract tissues collected at necropsy from nine animals with ICD. We show the presence of multiple viruses in the Parvoviridae and Picornaviridae family. We then compared the distribution of viral reads in the stomach, duodenum, jejunum, ileum, and the proximal, transverse, and distal colons. Tissues and mucosal scraping from the same locations showed closely related results while different gut tissues from the same animal varied widely. Picornavirus reads were generally more abundant in the lower digestive tract, particularly in the descending (distal) colon. -

Diversity and Evolution of Viral Pathogen Community in Cave Nectar Bats (Eonycteris Spelaea)
viruses Article Diversity and Evolution of Viral Pathogen Community in Cave Nectar Bats (Eonycteris spelaea) Ian H Mendenhall 1,* , Dolyce Low Hong Wen 1,2, Jayanthi Jayakumar 1, Vithiagaran Gunalan 3, Linfa Wang 1 , Sebastian Mauer-Stroh 3,4 , Yvonne C.F. Su 1 and Gavin J.D. Smith 1,5,6 1 Programme in Emerging Infectious Diseases, Duke-NUS Medical School, Singapore 169857, Singapore; [email protected] (D.L.H.W.); [email protected] (J.J.); [email protected] (L.W.); [email protected] (Y.C.F.S.) [email protected] (G.J.D.S.) 2 NUS Graduate School for Integrative Sciences and Engineering, National University of Singapore, Singapore 119077, Singapore 3 Bioinformatics Institute, Agency for Science, Technology and Research, Singapore 138671, Singapore; [email protected] (V.G.); [email protected] (S.M.-S.) 4 Department of Biological Sciences, National University of Singapore, Singapore 117558, Singapore 5 SingHealth Duke-NUS Global Health Institute, SingHealth Duke-NUS Academic Medical Centre, Singapore 168753, Singapore 6 Duke Global Health Institute, Duke University, Durham, NC 27710, USA * Correspondence: [email protected] Received: 30 January 2019; Accepted: 7 March 2019; Published: 12 March 2019 Abstract: Bats are unique mammals, exhibit distinctive life history traits and have unique immunological approaches to suppression of viral diseases upon infection. High-throughput next-generation sequencing has been used in characterizing the virome of different bat species. The cave nectar bat, Eonycteris spelaea, has a broad geographical range across Southeast Asia, India and southern China, however, little is known about their involvement in virus transmission. -

Molecular Epidemiology of Human Bocavirus in Children with Acute Gastroenteritis from North Region of Brazil
RESEARCH ARTICLE Soares et al., Journal of Medical Microbiology 2019;68:1233–1239 DOI 10.1099/jmm.0.001026 Molecular epidemiology of human bocavirus in children with acute gastroenteritis from North Region of Brazil Luana S. Soares*, Ana Beatriz F. Lima, Kamilla C. Pantoja, Patrícia S. Lobo, Jonas F. Cruz, Sylvia F. S. Guerra, Delana A. M. Bezerra, Renato S. Bandeira and Joana D. P. Mascarenhas Abstract Purpose. Human bocavirus (HBoV) is a DNA virus that is mostly associated with respiratory infections. However, because it has been found in stool samples, it has been suggested that it may be a causative agent for human enteric conditions. This under- pins the continuous search for HBoVs, especially after the introduction of the rotavirus vaccine due to acute gastroenteritis cases related to emergent viruses, as HBoVs are more likely to be found in this post-vaccine scenario. Therefore, the aim of this study is to demonstrate the prevalence of HBoV in children aged less than 10 years with acute gastroenteritis in Brazil from November 2011 to November 2012. Methodology. Stool samples from hospitalized children ≤10 years old who presented symptoms of acute gastroenteritis were analysed for the presence of rotavirus A (RVA) by an enzyme-linked immunosorbent assay (ELISA), and for HBoV DNA by nested PCR. Results. HBoV positivity was detected in 24.0 % (54/225) of samples. Two peaks of HBoV detection were observed in Novem- ber 2011 and from July to September 2012. Co-infections between HBoV and rotavirus A were identified in 50.0 % (27/54) of specimens. Phylogenetic analysis identified the presence of HBoV-1 (94.8 %), HBoV-2 (2.6 %) and HBoV-3 (2.6 %) species, with only minor variations among them. -

Statistical Analysis Plan
Non-Interventional Study Protocol Study Code << DXXXRXXX >> Version V1.4 Date 14 July 2017 Decline In lung-function Among Patients with chronic obstructive Lung disease On maintenance therapy (DIAPLO) An observational study evaluating the benefits of early intervention with maintenance therapies to prevent or slow down rapid lung function decline in patients who are at high risk at the time of COPD diagnosis in the combined Optimum Patient Care Research Database and Clinical Practice Research Datalink databases TITLE PAGE Non-Interventional Study Protocol Study Code << DXXXRXXX >> Version 14 July 2017 Date 14 July 2017 TABLE OF CONTENTS PAGE TITLE PAGE ........................................................................................................... 1 TABLE OF CONTENTS ......................................................................................... 2 LIST OF ABBREVIATIONS .................................................................................. 5 RESPONSIBLE PARTIES ...................................................................................... 6 PROTOCOL SYNOPSIS DIAPLO STUDY ........................................................... 7 AMENDMENT HISTORY ................................................................................... 12 MILESTONES ....................................................................................................... 13 1. BACKGROUND AND RATIONALE .................................................................. 14 1.1 Background ........................................................................................................... -

Two Novel Bocaparvovirus Species Identified in Wild Himalayan
SCIENCE CHINA Life Sciences SPECIAL TOPIC: Emerging and re-emerging viruses ............................. December 2017 Vol.60 No. 12: 1348–1356 •RESEARCH PAPER• ...................................... https://doi.org/10.1007/s11427-017-9231-4 Two novel bocaparvovirus species identified in wild Himalayan marmots Yuanyun Ao1†, Xiaoyue Li2†, Lili Li1, Xiaolu Xie3, Dong Jin4, Jiemei Yu1*, Shan Lu4* & Zhaojun Duan1* 1National Institute for Viral Diseases Control and Prevention, Chinese Center for Disease Control and Prevention, Beijing 100052, China; 2Laboratory Department, the First People’s Hospital of Anqing, Anqing 246000, China; 3Peking Union Medical College Hospital, Beijing 100730, China; 4National Institute for Communicable Disease Control and Prevention, Chinese Center for Disease Control and Prevention, Beijing 102206, China Received September 10, 2017; accepted September 16, 2017; published online December 1, 2017 Bocaparvovirus (BOV) is a genetically diverse group of DNA viruses and a possible cause of respiratory, enteric, and neuro- logical diseases in humans and animals. Here, two highly divergent BOVs (tentatively named as Himalayan marmot BOV, HMBOV1 and HMBOV2) were identified in the livers and feces of wild Himalayan marmots in China, by viral metagenomic analysis. Five of 300 liver samples from Himalayan marmots were positive for HMBOV1 and five of 99 fecal samples from these animals for HMBOV2. Their nearly complete genome sequences are 4,672 and 4,887 nucleotides long, respectively, with a standard genomic organization and containing protein-coding motifs typical for BOVs. Based on their NS1, NP1, and VP1, HMBOV1 and HMBOV2 are most closely related to porcine BOV SX/1-2 (approximately 77.0%/50.0%, 50.0%/53.0%, and 79.0%/54.0% amino acid identity, respectively). -
This Poster I It's Designed Large the Placeho Formatted Fo Placeholder
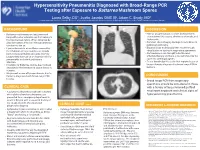
Hypersensitivity Pneumonitis Diagnosed with Broad-Range PCR Testing after Exposure to Battarrea Mushroom Spores • Laura Selby, DO1, Justin Jacobs OMS III2, Adam C. Brady, MD1 Printing: 1. Samaritan Health Services, Corvallis, Oregon 2. Western University of Health Sciences College of Osteopathic Medicine of the Pacific Northwest , Lebanon, Oregon This poster is 48” wide by 36” high. It’s designed to be printed on a BACKGROUND DISCUSSION large • Battarrea mushrooms are long-stemmed • Human lycoperdonosis is a rare disease that is fungi with a characteristic cap that belong to characterized by nausea, shortness of breath, and the Agaricaceae family. When disturbed by tachycardia. physical contact, they can release numerous • Common chest imaging findings include bilateral Customizing the Content: conidia into the air. pulmonary infiltrates. • Lycoperdonosis is a rare illness caused by • Diagnosis has traditionally been made through The placeholders in this the inhalation of large numbers of conidia visualization of spores in respiratory specimens. from certain puffball mushrooms (namely • Corticosteroids are thought to be the most formatted for you. Lycoperdon) that can cause hypersensitivity effective therapy and there is no definitive role for placeholders to add text, or click pneumonitis and mimic pulmonary systemic antifungal agents. infection. • To our knowledge this is the first reported case of an icon to add a table, chart, • Inhalation of Battarrea conidia has not been lycoperdonosis diagnosed by broad range PCR in described in the literature to cause illness in humans. SmartArt graphic, picture or humans. multimedia file. • We present a case of lycoperdonosis due to Battarea, diagnosed with broad-range PCR CONCLUSION T testing. -

Date: 1/9/2017 Question: Botulism Is an Uncommon Disorder Caused By
Date: 1/9/2017 Question: Botulism is an uncommon disorder caused by toxins produced by Clostridium botulinum. Seven subtypes of botulinum toxin exist (subtypes A, B, C, D, E, F and G). Which subtypes have been noted to cause human disease and which ones have been reported to cause infant botulism specifically in the United States? Answer: According to the cited reference “Only subtypes A, B, E and F cause disease in humans, and almost all cases of infant botulism in the United States are caused by subtypes A and B. Botulinum-like toxins E and F are produced by Clostridium baratii and Clostridium butyricum and are only rarely implicated in infant botulism” (Rosow RK and Strober JB. Infant botulism: Review and clinical update. 2015 Pediatr Neurol 52: 487-492) Date: 1/10/2017 Question: A variety of clinical forms of botulism have been recognized. These include wound botulism, food borne botulism, and infant botulism. What is the most common form of botulism reported in the United States? Answer: According to the cited reference, “In the United States, infant botulism is by far the most common form [of botulism], constituting approximately 65% of reported botulism cases per year. Outside the United States, infant botulism is less common.” (Rosow RK and Strober JB. Infant botulism: Review and clinical update. 2015 Pediatr Neurol 52: 487-492) Last updated November 1, 2017 Date: 1/11/2017 Question: Which foodborne pathogen accounts for approximately 20 percent of bacterial meningitis in individuals older than 60 years of age and has been associated with unpasteurized milk and soft cheese ingestion? Answer: According to the cited reference, “Listeria monocytogenes, a gram-positive rod, is a foodborne pathogen with a tropism for the central nervous system. -

Human Bocavirus in Nasopharyngeal Secretion of Hospitalized Children
Redni broj članka: 830 ISSN 1331-2820 (Tisak) ISSN 1848-7769 (Online) Human Bocavirus in Nasopharyngeal Secretion of Hospitalized Children with Acute Respiratory Tract Infection – First Year Results of a Four-Year Prospective Study Humani bokavirus u nazofaringealnom sekretu hospitalizirane djece s akutnom infekcijom dišnog sustava - Rezultati prve godine četverogodišnjeg prospektivnog istraživanja Maja Mijač1 Abstract 1,2 Sunčanica Ljubin-Sternak Background. Human bocavirus (HBoV) is a recently discovered parvovirus that Irena Ivković-Jureković3,4 may cause respiratory disease. The aim of this study was to determine HBoV Tatjana Tot5 prevalence among hospitalized children with acute respiratory tract infection Amarela Lukić-Grlić2,6 (ARI) in two Croatian hospitals, Children’s Hospital Zagreb and General Hos- Ivana Kale2 pital Karlovac, and to compare it with prevalence of other respiratory viruses. 2 Domagoj Slaćanac Methods. From May 2017 to April 2018 nasopharyngeal and pharyngeal swabs 1,2 Jasmina Vraneš from a total of 275 children with ARI of suspected viral etiology were obtained 1 Dr Andrija Štampar Teaching Institute of and tested by multiplex- PCR for the presence of 15 respiratory viruses, includ- Public Health, Croatia ing HBoV. 2 School of Medicine, University of Zagreb, Results. Viral etiology was proved in 221/275 (80.4%) of the patients. HBoV Croatia was detected in 17 (6.2 %) samples. Two thirds of HBoV positive patients were 3 Children’s Hospital Zagreb, Croatia between one and three years of age. HBoV was detected in older children when 4 School of Medicine, University of Osijek, compared to the children infected with respiratory syncytial virus (P < 0.001), Croatia but younger when compared to those infected with influenza (P = 0.009). -

Snapshot of Enteric Virome and RV Phylogenetics CONCLUSIONS An
The study of rotavirus phylogenetic diversity, re- assortment and interspecies transmission and associated virome in Northern Irish livestock exotic animals and wildlife Paula Lagan Tregaskis1,2, Mark Mooney2 and Ken Lemon1 1Virology Branch, Agri-food and Biosciences Institute Northern Ireland, Stoney Road, Stormont, Belfast BT4 3SD, UK 2Institute for Global Food Security, Biological Sciences, Queens University Belfast 3) VISUALISATION INTRODUCTION 1) DATA COLLECTION & QUALITY PROCESSING RESULTS 3b Korna chart Rotavirus (RV) is a highly infectious pathogen responsible for • Expected overall depth of reads expected at 25 2) WORKFLOW DATA ANALYSIS Porcine Microbiome WTA 79 acute diarrhoea in infants and animals worldwide. Enteritis is million the most common cause of mortality in neonatal calves in • Libraries yields per pair-end read; 500,000 to Northern Ireland. 3.4 million per sample. ANALYSIS A: ANALYSIS B: EDGE Platform AFBI Veterinary Science Division identified rotavirus as the Empowering the Development of Genomics Expertise • 97% Q30 (1 in 1000 base called incorrectly Trimmomatic MRC CLIMB project (Cloud Infrastructure for Microbial Bioinformatics) causative agent of enteritis in 28% of young calves and 48% 99.9%) of piglets faecal samples. • Remove low complexity reads, short reads and Meta-SPADES-Assembly uses k-mers for • RV is classified into groups from Group A to I and has a reads containing N building the initial de Bruijn graph EDGE pre-processing trimming 18Kb double stranded RNA genome. Group A is the most • Remove adaptors trim poor quality reads prevalent and virulent rotavirus. • Match pair-ends reads BLAST n and BLAST X alignment SPADES-Assembly uses k-mers for • Rotavirus has a dsRNA segmented genome with 11 for taxonomic classification building the initial de Bruijn graph segments. -

Evaluation of a Commercial Exogenous Internal Process Control for Diagnostic RNA Virus Metagenomics from Different Animal Clinical Samples T
Journal of Virological Methods 283 (2020) 113916 Contents lists available at ScienceDirect Journal of Virological Methods journal homepage: www.elsevier.com/locate/jviromet Evaluation of a commercial exogenous internal process control for diagnostic RNA virus metagenomics from different animal clinical samples T Steven Van Borma,*, Qiang Fub, Raf Winandb, Kevin Vannesteb, Mikhayil Hakhverdyanc, Dirk Höperd, Frank Vandenbusschea a Department of Animal Infectious Diseases, Sciensano, Groeselenbergstraat 99, 1180, Brussels, Belgium b Transversal Activities in Applied Genomics, Sciensano, Rue Juliette Wytsmanstraat 14, 1050, Brussels, Belgium c SVA, National Veterinary Institute, Ulls väg 2B, 751 89, Uppsala, Sweden d FLI, Friedrich Löffler Institut, Südufer 10, 17493 Greifswald, Germany ARTICLE INFO ABSTRACT Keywords: Metagenomic next generation sequencing (mNGS) is increasingly recognized as an important complementary Diagnostic metagenomics tool to targeted human and animal infectious disease diagnostics. It is, however, sensitive to biases and errors Virology that are currently not systematically evaluated by the implementation of quality controls (QC) for the diagnostic Next-generation sequencing use of mNGS. We evaluated a commercial reagent (Mengovirus extraction control kit, CeraamTools, bioMérieux) Quality control as an exogenous internal control for mNGS. It validates the integrity of reagents and workflow, the efficient Mengovirus isolation of viral nucleic acids and the absence of inhibitors in individual samples (verified using a specific -

Tropical Lung Disease Second Edition DK3042 Half-Series-Title.Qxd 8/23/05 2:25 PM Page B
DK3042_half-series-title.qxd 8/23/05 2:25 PM Page A Tropical Lung Disease Second Edition DK3042_half-series-title.qxd 8/23/05 2:25 PM Page B LUNG BIOLOGY IN HEALTH AND DISEASE Executive Editor Claude Lenfant Former Director, National Heart, Lung, and Blood Institute National Institutes of Health Bethesda, Maryland 1. Immunologic and Infectious Reactions in the Lung, edited by C. H. Kirkpatrick and H. Y. Reynolds 2. The Biochemical Basis of Pulmonary Function, edited by R. G. Crystal 3. Bioengineering Aspects of the Lung, edited by J. B. West 4. Metabolic Functions of the Lung, edited by Y. S. Bakhle and J. R. Vane 5. Respiratory Defense Mechanisms (in two parts), edited by J. D. Brain, D. F. Proctor, and L. M. Reid 6. Development of the Lung, edited by W. A. Hodson 7. Lung Water and Solute Exchange, edited by N. C. Staub 8. Extrapulmonary Manifestations of Respiratory Disease, edited by E. D. Robin 9. Chronic Obstructive Pulmonary Disease, edited by T. L. Petty 10. Pathogenesis and Therapy of Lung Cancer, edited by C. C. Harris 11. Genetic Determinants of Pulmonary Disease, edited by S. D. Litwin 12. The Lung in the Transition Between Health and Disease, edited by P. T. Macklem and S. Permutt 13. Evolution of Respiratory Processes: A Comparative Approach, edited by S. C. Wood and C. Lenfant 14. Pulmonary Vascular Diseases, edited by K. M. Moser 15. Physiology and Pharmacology of the Airways, edited by J. A. Nadel 16. Diagnostic Techniques in Pulmonary Disease (in two parts), edited by M. A.