Antibiotic Prophylaxis Clinical Practice Guideline: Supporting Documentation
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

WHO Technical Consultation to Review the Role of Drugs in Malaria Prevention for People Living in Endemic Settings
Malaria Policy Advisory Committee Meeting 13—14 May 2020, Geneva, Switzerland Background document for Session 5 WHO technical consultation to review the role of drugs in malaria prevention for people living in endemic settings Meeting report, 16–17 October 2019, Geneva, Switzerland Summary On 16–17 October 2019, the World Health Organization (WHO) convened a Technical Consultation to review the use of medicines for malaria prevention in endemic countries and to identify opportunities to increase their impact through review of the flexibility of the recommendations for their deployment. Experts reviewed the policies and use of chemoprevention as currently endorsed by WHO, including intermittent preventive treatment in pregnancy (IPTp), intermittent preventive treatment in infants (IPTi), seasonal malaria chemoprevention (SMC) and mass drug administration (MDA) for the reduction of disease burden in emergency situations. By reviewing these strategies side-by-side for the first time, the meeting was able to consider opportunities for optimization. Additional potential applications of chemoprevention were also reviewed, and key considerations identified to develop a broader role for malaria chemoprevention in malaria-endemic populations. Key conclusions of the meeting included: • There is a need for general guidance on the broader use of chemoprevention. Chemoprevention is an important approach in the package of strategies that countries may use to decrease their malaria burden and/or move towards malaria elimination. Development of broader, more flexible guidance that builds on existing chemoprevention recommendations in specific populations is expected to support the greater, more rational use of chemoprevention and enhance its impact. • Chemoprevention strategies may be tailored to country-specific needs. Guidance should be flexible enough to enable adaptation of strategies according to the needs of different countries and settings. -

Diagnostic Direct Laryngoscopy, Bronchoscopy & Esophagoscopy
Post-Operative Instruction Sheet Diagnostic Direct Laryngoscopy, Bronchoscopy & Esophagoscopy Direct Laryngoscopy: Examination of the voice box or larynx (pronounced “lair-inks”) under general anesthesia. An instrument called a laryngoscope is carefully placed into the mouth and used to visualize the larynx and surrounding structures. Bronchoscopy: Examination of the windpipe below the voice box in the neck and chest under general anesthesia. A long narrow telescope is passed through the larynx and used to carefully inspect the structures of the trachea and bronchi. Esophagoscopy: Examination of the swallowing pipe in the neck and chest under general anesthesia. An instrument called an esophagoscope is passed into the esophagus (just behind the larynx and trachea) and used to visualize the mucus membranes and surrounding structures of the esophagus. Frequently a small biopsy is taken to evaluate for signs of esophageal inflammation (esophagitis). What to Expect: Diagnostic airway endoscopy procedures generally take about 45 minutes to complete. Usually the procedure is well-tolerated and the child is back-to-normal the next day. Mild throat or tongue discomfort may persist for a few days after the procedure and is usually well-controlled with over-the-counter acetaminophen (Tylenol) or ibuprofen (Motrin). Warning Signs: Contact the office immediately at (603) 650-4399 if any of the following develop: • Worsening harsh, high-pitched noisy-breathing (stridor) • Labored breathing with chest retractions or flaring of the nostrils • Bluish discoloration of the lips or fingernails (cyanosis) • Persistent fever above 102°F that does not respond to Tylenol or Motrin • Excessive coughing or respiratory distress during feeding • Coughing or throwing up bright red blood • Excessive drowsiness or unresponsiveness Diet: Resume baseline diet (no special postoperative diet restrictions). -
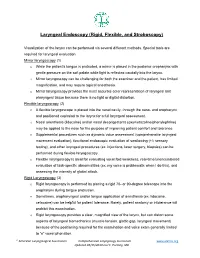
Laryngeal Endoscopy (Rigid, Flexible, and Stroboscopy)
Laryngeal Endoscopy (Rigid, Flexible, and Stroboscopy) Visualization of the larynx can be performed via several different methods. Special tools are required for laryngeal evaluation. Mirror laryngoscopy (1) o While the patient’s tongue is protruded, a mirror is placed in the posterior oropharynx with gentle pressure on the soft palate while light is reflected caudally into the larynx. o Mirror laryngoscopy can be challenging for both the examiner and the patient, has limited magnification, and may require topical anesthesia. o Mirror laryngoscopy provides the most accurate color representation of laryngeal and pharyngeal tissue because there is no light or digital distortion. Flexible laryngoscopy (2) o A flexible laryngoscope is placed into the nasal cavity, through the naso- and oropharynx and positioned cephalad to the larynx for a full laryngeal assessment. o Nasal anesthesia (lidocaine) and/or nasal decongestants (oxymetazoline/phenylephrine) may be applied to the nose for the purpose of improving patient comfort and tolerance o Supplemental procedures such as dynamic voice assessment (comprehensive laryngeal movement evaluation), functional endoscopic evaluation of swallowing (+/- sensory testing), and other laryngeal procedures (ex. injections, laser surgery, biopsies) can be performed during flexible laryngoscopy. o Flexible laryngoscopy is ideal for evaluating vocal fold weakness, real-time/unencumbered evaluation of task-specific abnormalities (ex. my voice is problematic when I do this), and assessing the intensity of glottal attack. Rigid Laryngoscopy (3) o Rigid laryngoscopy is performed by placing a rigid 70- or 90-degree telescope into the oropharynx during tongue protrusion. o Sometimes, oropharyngeal and/or tongue application of anesthesia (ex. lidocaine, cetacaine) can be helpful for patient tolerance. -
Which Antibiotic Prophylaxis Guidelines for Infective Endocarditis Should Canadian Dentists Follow?
Debate & O P I N I O N Which Antibiotic Prophylaxis Guidelines for Infective Endocarditis Should Canadian Dentists Follow? Contact Author Herve Y. Sroussi, DMD, PhD; Ashwin R. Prabhu, BDS; Dr. Epstein Joel B. Epstein, DMD, MSD, FRCD(C) Email: [email protected] For citation purposes, the electronic version is the definitive version of this article: www.cda-adc.ca/jcda/vol-73/issue-5/401.html ental providers must keep up to date 2 weeks following a procedure, dental proced- with antibiotic prophylaxis guidelines ures conducted even months earlier may be Dfor infectious endocarditis (IE) as these questioned as causative of IE.4 Furthermore, guidelines represent standards of care and periodontal and dental disease increase the determine medicolegal standards. A survey risk of bacteremia with activities of daily of Canadian dentists revealed that practi- living and may more commonly cause bac- tioners tend to employ antibiotic prophylaxis teremia; therefore, good oral care is of para- according to the guidelines in place at the mount importance in patients with conditions time of their graduation from dental school that place them at risk for IE. — guidelines that often do not meet the cur- To reduce the risk of IE following dental rent standards,1 as both the American Heart procedures, prophylactic measures have Association (AHA)2 and the British Society been developed by experts in the fields of for Antimicrobial Chemotherapy (BSAC)3 have microbiology, epidemiology, cardiology and currently updated their recommendations. dentistry. The principle preventive measure Host factors that increase the risk of IE recommended is the use of prophylactic anti- include specific cardiac abnormalities, a biotics before certain dental procedures in pa- previous episode of IE and the extent of the tients identified as at risk. -
Antibiotic Prophylaxis for Surgical Procedures
Summary and Conclusions Antibiotic Prophylaxis for Surgical Procedures A Systematic Review Swedish Council on Health Technology Assessment SBU Board of Directors and Scientific Advisory Committee Secretariat MÅNS ROSÉN Executive Director, SBU Board of Directors NINA REHNQVIST BJÖRN KLINGE MARGARETA TROEIN Karolinska Institute, Solna Karolinska Institute, TÖLLBORN (Chair) Solna The Swedish Society of Medicine EVA NILSSON BÅGENHOLM MÅNS ROSÉN The Swedish Medical SBU MATS ULFENDAHL Association The Swedish Research KARIN STRANDBERG NÖJD Council HÅKAN CEDER The Swedish Association The National Board of Local Authorities and SABINA WIKGREN ORSTAM of Health and Welfare Regions The Swedish Association ANNA-KARIN EKLUND HÅKAN SÖRMAN of Local Authorities and Swedish Association The Swedish Association Regions of Health Professionals of Local Authorities and Regions Scientific Advisory Committee DAVID BERGQVIST MATS G HANSSON ULF NÄSLUND Uppsala University Uppsala University Norrland University Hospital (Chair) Hospital, Umeå MIKAEL HELLSTRÖM BJÖRN BEERMANN Sahlgrenska Hospital, JOAKIM RAMSBERG Medical Products Agency, Gothenburg i3 Innovus, Stockholm Uppsala MARGARETA MÖLLER BO RUNESON CHRISTINA BERGH University Hospital, Karolinska Institute, Sahlgrenska Hospital, Örebro Solna Gothenburg JÖRGEN NORDENSTRÖM GUNNEL SVENSÄTER CECILIA BJÖRKELUND Karolinska University Malmö University Gothenburg University Hospital, Solna ANIA WILLMAN 2 SBU'S SUMMARY AND CONCLUSIONS SÖLVE ELMSTÅHL OLOF NYRÉN Blekinge Institute of University Hospital, Karolinska Institute, -

Analysis of the Effects of Malaria Chemoprophylaxis in Children on Haematological Responses, Morbidity and Mortality Paul D
Analysis of the effects of malaria chemoprophylaxis in children on haematological responses, morbidity and mortality Paul D. Prinsen Geerligs,1 Bernard J. Brabin,1,2 & Teunis A. Eggelte3 Abstract This paper reviews the evidence for beneficial effects of malaria chemoprophylaxis on haematological responses, morbidity, mortality, health service utilization and rebound immunity in children. As anaemia may play an important role in childhood mortality, it is important to assess evidence from controlled trials of the potential of chemoprophylaxis to reduce childhood anaemia. An analysis of trials found good evidence that malaria chemoprophylaxis improves mean haemoglobin levels and reduces severe anaemia, clinical malaria attacks, parasite and spleen rates. Significant reductions in outpatient attendance and hospital admissions have been achieved, and substantial evidence from Gambian studies shows reductions in mortality. Chemoprophylaxis in children does not seem to produce any sustained impairment of immunity to malaria, although rebound effects may be greater in children who receive prophylaxis during infancy. Short periods of targeted prophylaxis are likely to be preferable to continuous drug administration. Evidence of the protective efficacy of malaria chemoprophylaxis in children shows that this strategy could be considered within integrated health programmes for specific time periods. Intermittent routine combination therapy early in childhood may be appropriate for those living under holoendemic conditions. Large-scale studies over a number of years are needed to address this issue and the impact of this approach on health service utilization, mortality, and the emergence of drug-resistant parasites. Keywords Malaria/drug therapy/epidemiology; Malaria, Falciparum/drug therapy/epidemiology; Antimalarials/blood/therapeutic use; Anemia/drug therapy; Treatment outcome; Child; Infant mortality; Controlled clinical trials; Meta-analysis (source: MeSH, NLM). -
Flexible Sigmoidoscopy – Outpatients
Flexible sigmoidoscopy – Outpatients You have been referred by your doctor to have a flexible sigmoidoscopy. his information booklet has been written to explain the procedure. This will help you to make an informed decision before consenting to the procedure. If you are unable to attend your appointment please inform us as soon as possible. Please ensure you read this booklet and the enclosed consent form thoroughly. Please also complete the enclosed health questionnaire. You may be contacted by an endoscopy trained nurse before your procedure to go through the admission process and answer any queries you may have. If you are not contacted please come to your appointment at the time stated in your letter. Please note your appointment time is your arrival time on the unit and not the time of your procedure. If you have any mobility issues or if there is a possibility you could be pregnant, please contact the appointment staff on 01284 713551 Please remember there will be other patients in the unit who may arrive after you but are taken in for their procedure before you, this is for medical reasons or they are seeing a different doctor. Due to limited space available and to maintain other patients’ privacy and dignity, we only allow patients (and carers) through to the ward area. Relatives/ escorts will be contacted once you are ready for collection. The Endoscopy Unit endeavours to offer single sex facilities, and we aim to make you stay as comfortable and stress free as possible. Source: Endoscopy Reference No: 5035-14 Issue date: 8/1/21 Review date: 8/1/24 Page 1 of 11 Medication If you are taking WARFARIN, CLOPIDOGREL, RIVAROXABAN or any other anticoagulant (blood thinning medication), please contact the appointment staff on 01284 713551, your GP or anticoagulation nurse, as special arrangements may be necessary. -

SPECIALTY CARE Digestive Health
SPECIALTY CARE Digestive Health Through our Day Kimball Medical Group A lot of people care about your health. Including us. So if you’re 45 or practices and other associated specialty over and due for a colon screening, you should know that Day Kimball physicians, Day Kimball Healthcare has one of the most comprehensive digestive health programs around. provides you access to expert specialized care for virtually every body system Gastroenterology deals with the function, diseases and disorders of and condition, within an integrated and the digestive system, including the esophagus, stomach, pancreas, gall coordinated approach. bladder, bile ducts, liver, small intestine, colon (or large intestine), and rectum. Most everyone will need specialized care at some point in life. It’s good to know Physician Consultations that when that time comes you’ll have Consults for advanced treatment of digestive and liver disorders are access to physicians and facilities focused available through our associated board-certified gastroenterologists solely on providing you with top-notch from Connecticut GI. A referral from your primary care practitioner specialized care, close to home. (PCP) is required. Day Kimball Healthcare offers integrated, comprehensive care Endoscopy Services With our state-of-the-art Doris E. Madeira Endoscopy Suite at Day close to home. To learn more Kimball Hospital and the services of our associated gastroenterologists about all of our specialty from Connecticut GI, we are able to offer comprehensive screening, medical services -

Infectious Disease Society of America Influenza Clinical Practice Guidelines
Clinical Infectious Diseases IDSA GUIDELINE Downloaded from https://academic.oup.com/cid/advance-article-abstract/doi/10.1093/cid/ciy866/5251935 by Massachusetts Public Health Department user on 21 December 2018 Clinical Practice Guidelines by the Infectious Diseases Society of America: 2018 Update on Diagnosis, Treatment, Chemoprophylaxis, and Institutional Outbreak Management of Seasonal Influenzaa Timothy M. Uyeki,1 Henry H. Bernstein,2 John S. Bradley,3,4 Janet A. Englund,5 Thomas M. File Jr,6 Alicia M. Fry,1 Stefan Gravenstein,7 Frederick G. Hayden,8 Scott A. Harper,9 Jon Mark Hirshon,10 Michael G. Ison,11 B. Lynn Johnston,12 Shandra L. Knight,13 Allison McGeer,14 Laura E. Riley,15 Cameron R. Wolfe,16 Paul E. Alexander,17,18 and Andrew T. Pavia19 1Influenza Division, National Center for Immunization and Respiratory Diseases, Centers for Disease Control and Prevention, Atlanta, Georgia; 2Division of General Pediatrics, Cohen Children’s Medical Center, New Hyde Park, New York; 3Division of Infectious Diseases, Rady Children’s Hospital, and 4University of California, San Diego; 5Department of Pediatrics, University of Washington, Seattle Children’s Hospital; 6Division of Infectious Diseases Summa Health, Northeast Ohio Medical University, Rootstown; 7Providence Veterans Affairs Medical Center and Center for Gerontology and Healthcare Research, Brown University, Providence, Rhode Island; 8Division of Infectious Diseases and International Health, University of Virginia Health System, Charlottesville; 9Office of Public Health Preparedness -

Guideline on Antibiotic Prophylaxis for Dental Patients at Risk for Infection
american academy of pediatric dentistry Guideline on Antibiotic Prophylaxis for Dental Patients at Risk for Infection Originating Committee clinical affairs committee Review Council council on clinical affairs Adopted 1990 Revised 1991, 1997, 1999, 2002, 2005, 2007, 2008 Purpose may be at increased risk. If a patient reports a syndrome or The American Academy of Pediatric Dentistry (AAPD) recog- medical condition with which the practitioner is not familiar, nizes that numerous medical conditions predispose patients it is appropriate to contact the child’s physician to determine to bacteremia-induced infections. Because it is not possible to susceptibility to bacteremia-induced infections. predict when a susceptible patient will develop an infection, In 2007, the American Heart Association (AHA) released its prophylactic antibiotics are recommended when these patients newly revised guidelines for the prevention of IE and reducing undergo procedures most likely to produce bacteremia. This the risk for producing resistant strains of bacteria.3 The 2007 guideline is intended to help practitioners make appropriate revision was based on relevant literature and studies, in con- decisions regarding antibiotic prophylaxis for dental patients sultation with national and international experts. The AAPD, at risk. acknowledging the AHA’s expertise and efforts to produce evidenced-based recommendations, continues to endorse the Methods AHA guideline for antibiotic prophylaxis, now entitled “Pre- This guideline is based on a review of current dental and medical vention of Infective Endocarditis”. literature pertaining to postprocedural bacteremia-induced The primary reasons for the revision include: infections. A MEDLINE search was performed using the key- • “IE is much more likely to result from frequent exposure words “infective endocarditis” (IE), “bacteremia”, “antibiotic to random bacteremias associated with daily activities than prophylaxis”, and “dental infection”. -

Antibiotic Prophylaxis for GI Endoscopy
GUIDELINE Antibiotic prophylaxis for GI endoscopy This is one of a series of statements discussing the use of procedure. Endoscopy-related bacteremia carries a small GI endoscopy in common clinical situations. The Stan- risk of localization of infection in remote tissues (ie, infec- dards of Practice Committee of the American Society for tive endocarditis [IE]). Endoscopy also may result in local Gastrointestinal Endoscopy (ASGE) prepared this docu- infections in which a typically sterile space or tissue is ment, and it updates a previously issued document on breached and contaminated by an endoscopic accessory this topic.1 In preparing this guideline, MEDLINE and or by contrast material injection. This document is an up- PubMed databases were used to search for publications date of the prior ASGE document on antibiotic prophylaxis between January 1975 and December 2013 pertaining for GI endoscopy,1 discusses infectious adverse events to this topic. The search was supplemented by accessing related to endoscopy, and provides recommendations for the “related articles” feature of PubMed, with articles periprocedural antibiotic therapy. identified on MEDLINE and PubMed as the references. Additional references were obtained from the bibliogra- phies of the identified articles and from recommenda- BACTEREMIA ASSOCIATED WITH tions of expert consultants. When few or no data were ENDOSCOPIC PROCEDURES available from well-designed prospective trials, emphasis was given to results from large series and reports from Bacteremia can occur after endoscopic procedures and has been advocated as a surrogate marker for IE risk. How- recognized experts. Weaker recommendations are indi- fi cated by phrases such as “We suggest.” whereas stronger ever, clinically signi cant infections are extremely rare. -

Antibiotic Prophylaxis for Surgical Procedures: a Scoping Review
01 Pan American Journal Review of Public Health 02 03 04 05 06 Antibiotic prophylaxis for surgical procedures: 07 08 a scoping review 09 10 11 1,2 2 1 2 2 Eva Brocard, Ludovic Reveiz, Jean-Philippe Régnaux, Veronica Abdala, Pilar Ramón-Pardo, 12 and Ana del Rio Bueno2 13 14 15 16 Suggested citation Brocard E, Reveiz L, Régnaux J-P, Abdala V, Ramón-Pardo P, del Rio Bueno A. Antibiotic prophylaxis for surgical procedures: 17 a scoping review. Rev Panam Salud Publica. 2021;45:e62. https://doi.org/10.26633/RPSP.2021.62 18 19 20 21 ABSTRACT Objectives. To map the current evidence on surgical antibiotic prophylaxis (SAP) administration and identify 22 knowledge gaps in the literature available in this field. 23 Methods. The PubMed, Cochrane Library, Epistemonikos, and Health Systems Evidence databases were 24 searched from January 2015 to March 2020 for systematic reviews published in English, French, Portuguese, 25 and Spanish. 26 Results. Eighty-three systematic reviews were included, the quality of the reviews was assessed using 27 AMSTAR 2, and data were extracted for all primary outcomes. Perioperative antibiotic administration, the use 28 of first generation cephalosporins, and surgical site infection (SSI) were the most commonly reported for timing 29 of antibiotic administration, drug class, and primary outcome, respectively. Findings showed that, overall, SAP 30 may reduce SSIs compared with a placebo or with no SAP. Results suggested that intraoperative SAP may 31 lower SSI, while postoperative SAP did not show a statistically significant difference. 32 Conclusions. Findings have confirmed the role of SAP in reducing postoperative SSI across various surgeries 33 and do not support the use of antibiotics after surgery to prevent infections.