A History of Poliomyelitis in New Zealand
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
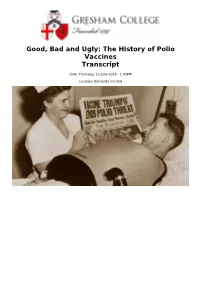
Good, Bad and Ugly: the History of Polio Vaccines Transcript
Good, Bad and Ugly: The History of Polio Vaccines Transcript Date: Thursday, 12 June 2014 - 1:00PM Location: Barnard's Inn Hall 12 June 2014 Good, Bad and Ugly: The History of Polio Vaccines Professor Gareth Williams The main villain of the piece is the poliovirus, one of the smallest and simplest viruses. It is usually spread by the faecal-oral route (dirty fingers!) and in most cases is confined to the gut. As travels down the intestine, it induces antibodies (immunity) against itself, which will protect the person against future attacks by the virus. In about 1% of cases, the virus floods into the bloodstream and infects the nerve cells in the spinal cord which drive the muscles. This causes the characteristic paralysis, which can affect one or more limbs and/or the muscles of respiration – in which case artificial ventilation (e.g. with the iron lung) may be needed to keep the patient breathing and alive. Polio originally caused sporadic clusters of paralysis, especially in children. For some reason, this pattern changed during the late 19th century into explosive epidemics which swept through many countries each summer. The first major outbreak, on the East Coast of the USA in the summer of 1916, caused 25,000 cases of paralysis and 6,000 deaths. Draconian public health measures were powerless to prevent the spread of polio, resulting in widespread panic across America. Each year, panic resurfaced as the polio season approached, with the wealthy leaving towns and cities in droves. During the early 1950s, Americans feared polio almost as much as the atom bomb. -

Jonas Salk at the National Press Club, April 12, 1965
Jonas Salk at the National Press Club, April 12, 1965 Jonas Salk, May 1962. A.F.P. – D.P.A. Photos. National Press Club Archives On the tenth anniversary of the licensing of the polio vaccine he developed, Dr. Jonas E. Salk (1914-1995) visited Washington to accept a joint congressional resolution that hailed the vaccine as “one of the most significant medical achievements of our time.” At the White House, President Johnson offered Salk his congratulations. The day also marked the twentieth anniversary of the death of former President Franklin D. Roosevelt, who, having suffered from paralytic polio since 1921, had established the foundation that funded Salk’s efforts. Following his meetings with Congress and the President, Salk gave a talk and answered reporters’ questions at a National Press Club luncheon. In the title of its lead editorial ten years earlier celebrating the successful testing of the new vaccine, the New York Times proclaimed the “Dawn of a New Medical Day.” Testing of the vaccine, like the funding for its development, had engaged the participation of millions of ordinary American citizens. Through March of Dimes campaigns, hundreds of thousands of volunteers went door-to-door raising $41 million in 1952 alone from average donations of 27 cents. The tests involved 1.8 million school children, 200,000 volunteers, 64,000 teachers, and 60,000 physicians, nurses, and health officials, making it the largest clinical trial in history. Interpreting the jubilant 1 reaction to news that the vaccine had been proven safe and effective, the Times commented, “Gone are the old helplessness, the fear of an invisible enemy, the frustration of physicians.” Poliomyelitis, also known as infantile paralysis, is an extremely contagious viral infection caused by any of three types of poliovirus. -

The March of Dimes and Polio: Lessons in Vaccine Advocacy for Health Educators
Feature Article The March of Dimes and Polio: Lessons in Vaccine Advocacy for Health Educators Dawn Larsen ABSTRACT The polio vaccine became available in 1955, due almost entirely to the efforts of the March of Dimes. In 1921, Franklin Roosevelt gave a public face to polio and mounted a campaign to prevent it, establishing the National Foundation for Infantile Paralysis in 1938. During the Depression, U.S. citizens were asked to contribute one dime. Entertainer Eddie Cantor suggested the name the March of Dimes, paraphrasing the popular newsreel “The March of Time.” Jonas Salk advocated a killed-virus vaccine while Albert Sabin proposed a live-virus vaccine. Both competed for both recognition and funding from the March of Dimes. In 1955 Salk’s vaccine was adopted, nationwide vaccination programs were implemented, and polio rates dropped by 80 percent. In 1961, Sabin’s vaccine, endorsed by the American Medical Association, became the vaccine of choice. The World Health Assembly advocated polio eradication by the year 2000. By 2004 eradication efforts were threatened by allegations linking vaccines to chronic diseases. Immunization dropped and polio resurfaced in the U.S., Australia, Africa and Russia. Research linking vaccines to chronic disease was dis- credited, but vaccine opponents remain active. Health educators are well positioned to mitigate damage caused by the anti-vaccine movement and address barriers to immunization efforts. Larsen D. The March of Dimes and polio: lessons in vaccine advocacy for health educators. Am J Health Educ. 2012;43(1):47-54. Submitted May 30, 2011. Accepted July 9, 2011. In 2008, The March of Dimes cel- prenatal health promotion programs, and of the virus that has been ranked second ebrated its 70th anniversary. -

Isolating Madness: Photographs from Seacliff Lunatic Asylum, 1887-1907
Isolating Madness: Photographs from Seacliff Lunatic Asylum, 1887-1907 Elizabeth Laing For my mum, thank you for taking me to the museum. A thesis submitted to the Victoria University of Wellington in fulfillment of the requirements for the degree of Master of Arts in Art History Victoria University of Wellington 2014 For my mum, thank you for taking me to the museum. Acknowledgements This thesis would not have been possible without the access granted by the Southern District Health Board, and the assistance of staff from the Archives New Zealand branch in Dunedin. I would particularly like to acknowledge Vivienne Cuff, who ably facilitated my research during my visits to the reading room, and patiently responded to all of my subsequent enquiries. As an agreed condition of access, I have concealed the identities of the patients discussed by using pseudonyms. I would like to sincerely thank my supervisor, Geoffrey Batchen, whose conversations and steadfast support inspired this thesis in countless ways. I hope that it meets with his approval. Abstract Frederic Truby King (1858-1938) is an eminent figure in New Zealand history. His name continues to flourish in contemporary society, due in part to its affiliation with the Royal New Zealand Plunket Society. However, the general populace is still relatively unaware of the time that King spent employed as the medical superintendent of Seacliff Lunatic Asylum, on the remote outskirts of Dunedin. The prevailing image of King during this period is of a single-minded physician, whose career was in a state of acceleration towards the establishment of Plunket. -
Plunket Annual Report 2016/17
ANNUAL REPORT The2017 Royal New Zealand Plunket Society Inc. a Our vision 3 From our New Zealand President 4 From our Chief Executive 6 Plunket by the numbers 8 Our heart 12 Our people 16 Our approach 18 Our insights 20 Our funding 22 Plunket Board and Leadership 26 Financials 28 Funding Partners 34 Principal Partner 36 ISSN 0112-7004 (Print) ISSN 2537-7671 (Online) 1 OUR VISION OUR GOALS OUR MĀORI PRINCIPLES Our vision, Healthy tamariki – We make sure every Mana Atua – Mana Atua is the most Whānau tamariki/child has the opportunity to be important foundation pillar, enabling āwhina as healthy and well as they can be. Māori to reconnect to the source of Confident whānau – We build the creation, based on their realities as goals, In the first 1000 confidence and knowledge of whānau/ tangata whenua. The disconnection families across New Zealand. of tangata whenua from their Mana days we make Atua (resulting in a state of Wairua Connected communities – We make Matangaro) is a source of ‘haumate’ the difference sure no whānau/family is left isolated, strategic (unwellness). disconnected or unable to cope. of a lifetime Mana Tūpuna – Acknowledging OUR STRATEGIC THEMES the ancestral dimension, a person’s Tamariki, their whānau/family and connection to their ancestry through themes whakapapa (genealogy). communities are at the heart of everything we do. Mana Whenua – Mana Whenua High performing Plunket people. recognises the physical, spiritual and emotional connection to the land. This & Māori Integrated, collaborative and includes forests, swamps, pa sites, connected approach. rivers and other geographical entities, Plunket is a learning organisation elements each in their own right able to principles fuelled by knowledge, data and define a person’s tūrangawaewae (place insights. -

“They'll Go Like British Shells!”: a Historical Perspective on Commercial
“They’ll Go Like British Shells!”: A Historical Perspective on Commercial “Anzackery” in New Zealand STEVEN LOVERIDGE Abstract The term “Anzackery” was regularly employed in New Zealand during the centenary of the First World War to condemn a sense of irreverent exploitation of Anzac remembrance, with commercial exploitation forming a particular concern. This article contends that such sentiments continue a much older dynamic and seeks to offer a historical perspective by surveying the relationship between marketing and war, circa 1914–1918. It examines the rise of a distinctive mode of branding goods and services in the decades leading up to and including the First World War, investigates the wartime mobilisation of this consumerism and contemplates the nature of the resulting criticism. In doing so, it provides some perspective on and insight into the contemporary concerns of the relationship between commercial activity and Anzac remembrance in New Zealand. Across the centenary of the First World War, New Zealand enterprises displayed a remarkable capacity to brand diverse products with reference to the conflict and Anzac.1 Museum gift shops stocked a wealth of merchandise—including T-shirts, mobile phone cases, fridge magnets, stickers, coffee mugs, drink coasters and postcards—stamped with First World War iconography. Specialty remembrance poppies were produced for motorists to attach to their vehicles’ bumpers and rear windows. The Wellington Chocolate Factory created “The Great War Bar,” the wrapper of which depicted entrenched soldiers taking relief in small comforts. Accompanying marketing noted that “Thousands of chocolate bars left the hands of loved ones on their voyage to those on the front line. -

Polio in Italy
Polio in Italy Bernardino Fantini (*) (*) Institute for the History of Medicine and Health, University of Geneva. [email protected] Dynamis Fecha de recepción: 23 de enero de 2012 [0211-9536] 2012; 32 (2): 329-359 Fecha de aceptación: 5 de marzo de 2012 SUMMARY: 1.—Introduction. 2.—The epidemiology of polio in Italy. 3.—The social and scientific reactions to the polio epidemics. 4.—The 1958 epidemics. 5.—The different actors. 6.—The vaccination campaign and the elimination of the disease. 7.—Changing attitudes in patients and the public. 8.—The origins of patient’s associations. 9.—The post-epidemic problems. The post-polio syndrome. 10.—Concluding remarks. ABSTRACT: The history of polio in Italy is relatively short because the particular social and demographic history of the country has actually compressed the most dramatic history of the polio epidemic into only 40 years, from the first severe epidemic just before World War II to the early 1980s, when the epidemic vanished thanks to an effective and country-wide vaccination campaign. The epidemic, however, had a formidable impact on medicine, public health, social attitudes and culture. An analysis of this case study can illustrate the impact of an epidemic of a severe disease on individual and collective life, and at the same time the efficacy of public health measures against it, and the importance of the social structure, state and private, in coping with the consequences of the epidemics. In this period, the attitude towards the handicapped changed from stigma and isolation to social integration, thanks especially to the changes in health legislation, social action and the initiatives of the patient’ associations. -

Poliomyelitis and the Neurologists: the View from England, 1896-1966
Poliomyelitis and the Neurologists: The View from England, 1896-1966 ANNE HARDY The American vs. the European Experience In 1907, following one of the earliest poliomyelitis outbreaks in New York City, the New York Neurological Society set up a poliomyelitis committee with a view to studying and illuminating the behavior of this newly epi- demic disease.' The neurologists7 interest in polio was of long standing, dating from the orthopedic surgeon Jacob von Heine's conclusion, in 1860, that the symptoms of infant paralysis pointed to "an affection of the central nervous system, namely the spinal cord."* Ten years later, Heine7s deduction had been confirmed by the researches ofJean-Martin Charcot (1825-93), who demonstrated the destruction of the grey matter of the anterior horns of the spinal cord (within which the motor impulses arise and are transmitted) in cases of infant paralysk3 This demonstration of the pathology of the disease placed it firmly within the concerns of neurol- ogy, where it remained until polio arrived as a major epidemic problem. In America, according to John R. Paul, the New York Neurological Society's committee marked "almost the last time that neurologists as a professional body were to assume a position of dominance with respect This article was written in memory of Elizabeth Mary Margaret Hardy (1922-52). I am grateful to Michael Neve, who gave me the occasion to write it; to Bill Bynum, for advice; to Irvine Loudon, for generously supplying the graph; and to Tony Gould, Andrew Wear, and the Bulletin's anonymous referees, for constructive criticism. 1.John R. -

'Hidden Under Many Bushels': Lady
New Zealand Journal of History, 39, 1 (2005) ‘Hidden under many bushels’ LADY VICTORIA PLUNKET AND THE NEW ZEALAND SOCIETY FOR THE HEALTH OF WOMEN AND CHILDREN* Mittie wrote this morning & said V[ictoria]s name & words of wisdom on infants were being quoted in many journals; I’m glad as I’ve looked on for her name in many accounts of welfare meetings & not seen it & thought as usual she was being hidden under many bushels.1 ON 14 MAY 1907 in Dunedin, Dr Truby King founded the New Zealand Society for the Health of Women and Children, now known as the Plunket Society. It was named in honour of Lady Victoria Plunket, wife of the unexceptional Sir William ‘Willie’ Plunket, Governor-General of New Zealand from 1904 to 1910.2 Within 20 years, both King, the Society and its nurses had become international icons of infant welfare and enduring symbols of the strength and might of all things British. The success of the Plunket Society is well known and the organization remains an influential and important New Zealand institution. At one time or another a large majority of New Zealand parents have accessed the Society’s child health services including the Plunket nurse. Its history has also been well served in recent times. Linda Bryder’s book A Voice for Mothers offers a comprehensive and readable history of the Plunket Society, and places it firmly within the history of the voluntary sector in the twentieth century.3 Indeed Bryder states that the Plunket Society is perhaps the ‘most successful voluntary organization’ in New Zealand.4 Phillipa Mein -

Rape Representation in New Zealand Newspapers (1975 – 2015)
It’s The Same Old Story: Rape Representation in New Zealand Newspapers (1975 – 2015) By Angela Millo Barton A thesis submitted to the Victoria University of Wellington in fulfilment of the requirements for the degree of Master of Arts in Criminology School of Social and Cultural Studies Victoria University of Wellington 2017 ii Abstract Newspaper reporting of rape, and in particular, representations of women as rape victims, have historically been presented by the media in a misinformed manner, influenced by myths and misconceptions about the dynamics of sexual violence. Previous research has shown media depictions can promote victim-blaming attitudes which affect society’s understanding toward sexual violence, promoting false narratives and rape-supportive beliefs. Victim narratives of sexual victimisation struggle within a ‘culture of silencing’ that prevents the majority of sexual offending from coming to the attention of authorities, and identifying the silencing of women’s experiences of rape has, and continues to be, a key objective for feminist scholars. Newspapers are one medium which has been exclusionary of women's experiences, therefore it is important to look at the role of newspapers on a longitudinal level to investigate whether there have been changes in reporting practices and attitudes. To address this issue, this study draws on feminist perspectives and adopts a quantitative and qualitative methodology utilising newspaper articles as a specific source of inquiry. Articles concerning male-female rape were collected from eight prominent New Zealand newspapers across a 40 year period from 1975 – 2015 with individual years for analysis being 1975, 1985, 1995, 2005 and 2015. Results from this analysis show minimal inclusion of women’s words regarding newspaper commentary in articles concerning rape. -

Hymn of Hate”
Wicked Wilhelmites and Sauer Krauts: The New Zealand Reception of Ernst Lissauer’s “Hymn of Hate” ROGER SMITH Abstract When the German poet Ernst Lissauer published his anti-English poem “Haßgesang gegen England” in the early weeks of the First World War, the effect was electric. The poem, translated into English and dubbed the “Hymn of Hate,” echoed around the globe, reaching as far as New Zealand where newspapers sedulously followed its international reception and published local responses. Given the nature of New Zealand’s relationship to Britain and the strength of the international press links, it is not surprising that news of the poem reached New Zealand in the early months of the war. However, the sheer volume of coverage given to a single German war poem in New Zealand’s press over the course of the war and after, as well as the many and varied responses to that poem by New Zealanders both at home and serving overseas, are surprising. This article examines the broad range of responses to Lissauer’s now forgotten poem by New Zealanders during the Great War and after, from newspaper reports, editorials and cartoons, to poetic parodies, parliamentary speeches, enterprising musical performances and publications, and even seasonal greeting cards. “The poem fell like a shell into a munitions depot.” With these words, the Austrian novelist Stefan Zweig recalled the impact made by Ernst Lissauer’s anglophobic poem “Haßgesang gegen England” (“A Chant of Hate Against England”) upon first publication in Germany in 1914.1 The reception of Lissauer’s poem in the German-speaking world is a remarkable story, but its reception, in translation, in the English-speaking world is no less surprising. -

Nature's Good for You Sir Truby King, Seacliff Asylum, and the Greening Of
Health & Place 22 (2013) 107–114 Contents lists available at SciVerse ScienceDirect Health & Place journal homepage: www.elsevier.com/locate/healthplace Nature's good for you: Sir Truby King, Seacliff Asylum, and the greening of health care in New Zealand, 1889–1922 Paul V. Stock a,n, Chris Brickell b,1 a University of Kansas, Sociology and the Environmental Studies Program, 1415 Jayhawk Boulevard, Room 739, Fraser Hall, Lawrence, KS 66045-7556, United States b University of Otago, Sociology, Gender and Social Work, P.O. Box 56, Dunedin 9054, New Zealand article info abstract Article history: Sir Frederic Truby King's work at Seacliff Asylum in New Zealand, between 1889 and 1922, illustrates a Received 26 October 2012 prominent role of agriculture in relationship to human health and the environment. King utilized Received in revised form farming practices, a rural setting, occupational therapy, dietary changes and moves towards self- 28 February 2013 sufficiency as examples of asylum management practices, but these also ensured patient health and Accepted 4 March 2013 well-being. In this article, we analyze King's practices at Seacliff as a genealogical precursor to today's Available online 28 March 2013 green care and care farming movements. Keywords: & 2013 Elsevier Ltd. All rights reserved. Sir Frederic Truby King New Zealand Asylums Care farming/green care Agriculture 1. Introduction fishing operation at the nearby beach settlement of Karitane. At the same time, this outdoor work provided valuable therapeutic [A] harmless old man… looked after the chickens. His phobia benefits. There is a certain historical continuity too. The care was fire, and he painted all the farm gates, posts and fences centers of today's burgeoning green care movement have both with clay and water “to prevent them burning”.