Joint Strategic Needs Assessment for Tameside
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Manchester Metrolink Tram System
Feature New Promise of LRT Systems Manchester Metrolink Tram System William Tyson Introduction to Greater city that could be used by local rail into the city centre either in tunnel or on Manchester services—taking them into the central the street. area—to complete closure and I carried out an appraisal of these options The City of Manchester (pop. 500,000) is replacement of the services by buses. Two and showed that closure of the lines had at the heart of the Greater Manchester options were to convert some heavy rail a negative benefit-to-cost ratio, and that— conurbation comprised of 10 lines to light rail (tram) and extend them at the very least—they should be kept municipalities that is home to 2.5 million people. The municipalities appoint a Passenger Transport Authority (PTA) for the Figure 1 Metrolink Future Network whole area to set policies and the Greater 1 Victoria Manchester Passenger Transport Executive 2 Shudehill 3 Market Street Rochdale Town Centre 4 Mosley Street (GMPTE) to implement them. Buses Newbold Manchester 5 Piccadilly Gardens Drake Street Piccadilly Kingsway Business Park 6 Rochdale provide most public transport. They are 7 St Peter's Square Railway Milnrow Station deregulated and can compete with each 8 G-Max (for Castlefield) Newhey London 9 Cornbrook other and with other modes. There is a 0 Pomona Bury - Exchange Quay local rail network serving Manchester, and = Salford Quays Buckley Wells ~ Anchorage ! Harbour City linking it with the surrounding areas and @ Broadway Shaw and Crompton # Langworthy also other regions of the country. Street $ Tradfford Bar trams vanished from Greater Manchester % Old Trafford Radcliffe ^ Wharfside* & Manchester United* in 1951, but returned in a very different * Imperial War Museum for the North* ( Lowry Centre form in 1992. -
Prospectus 2021/22
Lewis Kelsall 2020 Destination:e Cambridg 100 with bestLeve l University, ever A . Engineering high grades Adam Kelsall Destination: Loughborough University Aeronautical, Engineering Clarendon Sixth Form College Camp Street Ashton-under-Lyne OL6 6DF Prospectus 2021/22 03 Message from the Principal 04 Choose a ‘Good’ College 05 Results day success 06 What courses are on offer? 07 Choosing your level and entry requirements 08 How to apply 09 Study programme 12 Study skills and independent learning programme 13 Extended Project Qualification (EPQ) and Futures Programme 14 Student Hub 16 Dates for your diary 17 Travel and transport 18 University courses at Tameside College 19 A year in the life of... Course Areas 22 Creative Industries 32 Business 36 Computing 40 English and Languages 44 Humanities 50 Science, Mathematics and Engineering 58 Social Sciences 64 Performing Arts 71 Sports Studies and Public Services 02 Clarendon Sixth Form College Prospectus 2021/22 Welcome from the Principal Welcome to Clarendon Sixth Form College. As a top performing college in The academic and support Greater Manchester for school leavers, package to help students achieve while we aim very high for our students. Our studying is exceptional. It is personalised students have outstanding success to your needs and you will have access to a rates in Greater Manchester, with a range of first class support services at each 100% pass rate. stage of your learning journey. As a student, your career aspirations and This support package enables our students your college experience are very important to operate successfully in the future stages of to us. -

Greater Manchester, New Hampshire
Greater Manchester, New Hampshire Health Improvement Plan 2016 with support from the City of Manchester Health Department and the Greater Manchester Public Health Network WORKING TO IMPROVE THE HEALTH AND WELL-BEING OF THE GREATER MANCHESTER REGION EXECUTIVE SUMMARY The City of Manchester Health Department and the Greater Manchester Public Health Network are pleased to present the first Health Improvement Plan for the Greater Manchester Public Health Region. Our collective vision is to transform public health in our region to an integrated system capable of seamless collaborations among all healthcare providers and public safety personnel with constructive engagement of patients, families, and communities. Through this integrated system, all people will have equitable access to timely, comprehensive, cost-effective, high-quality, and compassionate care. Public health is the practice of preventing disease and promoting good health within groups of people-- from small communities to entire countries. Public Health is YOUR health. It embodies everything from clean air to safe food and water, access to healthcare and safer communities. Through public health planning and prevention initiatives, the public gets sick less frequently, children grow to become healthy adults through adequate resources including health care, and our community reduces the impact of disasters by preparing people for the effects of catastrophes such as hurricanes, floods and terrorism. In preparing this Plan, the Public Health Network and its workgroups have reviewed needs assessments, utilizing data from many different sources such as community focus groups, key stakeholder interviews, and surveys. Building on this information, needs have been prioritized and work plans have been developed. This Health Improvement Plan identifies needs, goals, measurable objectives, and strategies to help us as we work together on solutions to important issues facing our community. -
Nomination Paper Pack for By-Election of Hyde Newton on 5Th
Nomination Paper Office Use Only No of Nomination Paper Time delivered Date delivered Initials Tameside Metropolitan Borough in order of delivery ELECTION OF A BOROUGH COUNCILLOR for Hyde Newton Date of Election: Thursday 5 February 2009 We the undersigned, being local government electors for the said Ward , do hereby nominate the under-mentioned person as a candidate at the said election. PLEASE COMPLETE IN CAPITALS (except where a signature is required) Candidate’s Other forename(s) Commonly used Commonly used Home Address surname forenames Description (if any) use no more than 6 words surname in full (if any) (if any) in full Title Email Address Telephone Electoral Number Signature Print Name as Signed Polling District Number Letters Proposer Seconder We the undersigned, being local government electors for the said Ward, do hereby assent to the foregoing nomination 1 2 3 4 5 6 7 8 Notes 1. The attention of candidates and electors is drawn to the rules for filling up nomination papers and provisions relating to nomination papers contained the election rules in Schedule 2 to the Local Election (Principle Areas) Rules 2006. 2. Where a candidate is commonly known by some title they may be described by their title as if it were their surname. 3. Where a candidate commonly uses a name which is different from any other name they have, the commonly used name may also appear on the nomination paper, but if it does so, the commonly used name (instead of any other name) will appear on the ballot paper. 4. But the ballot paper will show the other name if the Returning Officer thinks that the use of the commonly used name may (a) be likely to mislead or confuse electors, or (b) that the commonly used name is obscene or offensive. -

Minor Eye Conditions Service (MECS) Tameside and Glossop Pharmacies That Are Currently Providing Mecs
Minor Eye Conditions Service (MECS) Tameside and Glossop Pharmacies that are currently providing MECs Name Address Telephone 169 Mossley Road, Ashton-under-Lyne, Lancashire, OL6 Adams Pharmacy 6NE 0161 339 8889 Stalybridge Resource Centre, 2 Waterloo Road, Stalybridge. Adams Pharmacy SK15 2AU 0161 303 8599 Alipharma Ltd Thornley House Med Ctr) 11 Thornley Street, Hyde SK14 1JY 0161 351 1386 Asda Cavendish Street, Ashton Under Lyne, OL6 7DP 0161 342 6610 Asda Water Street, Hyde, Cheshire, SK14 1BD 0161 882 5700 22 Stockport Road, Ashton-Under-Lyne, Lancashire, OL7 Ashton Pharmacy 0LB 0161 330 4389 Ashton Primary Care Centre Pharmacy 193 Old Street, Ashton-Under-Lyne, Lancashire, OL6 7SR 0161 820 8281 Audenshaw Pharmacy 3 Chapel Street, Audenshaw, Manchester, M34 5DE 0161 320 9123 Boots 116-118 Station Road, Hadfield, Glossop SK13 1AJ 01457 853635 Hattersley Health Centre, Hattersley Road East, Hattersley, Boots Hyde SK14 3EH 0161 368 8498 Boots 72 Market Street, Droylsden, Manchester M43 6DE 0161 370 1626 Boots 30 Concorde Way, Dukinfield, Cheshire SK16 4DB 0161 330 3586 Boots 173 Mossley Road, Ashton-Under-Lyne OL6 6NE 0161 330 1303 Boots 1-3 Bow Street, Ashton-Under-Lyne OL6 6BU 0161 330 1746 Boots UK Ltd 15-17 Staveleigh Way, Ashton-Under-Lyne OL6 7JL 0161 308 2326 Boots UK Ltd 19 High Street West, Glossop, Derbyshire SK13 8AL 01457 852011 Boots UK Ltd 1A Market Place, Hyde, Cheshire SK14 2LX 0161 368 2249 Boots UK Ltd 33 Queens Walk, Droylsden, Manchester M43 7AD 0161 370 1402 Crown Point North, Retail Park, Ashton Road, Denton M34 -
Framework Users (Clients)
TC622 – NORTH WEST CONSTRUCTION HUB MEDIUM VALUE FRAMEWORK (2019 to 2023) Framework Users (Clients) Prospective Framework users are as follows: Local Authorities - Cheshire - Cheshire East Council - Cheshire West and Chester Council - Halton Borough Council - Warrington Borough Council; Cumbria - Allerdale Borough Council - Copeland Borough Council - Barrow in Furness Borough Council - Carlisle City Council - Cumbria County Council - Eden District Council - South Lakeland District Council; Greater Manchester - Bolton Metropolitan Borough Council - Bury Metropolitan Borough Council - Manchester City Council – Oldham Metropolitan Borough Council - Rochdale Metropolitan Borough Council - Salford City Council – Stockport Metropolitan Borough Council - Tameside Metropolitan Borough Council - Trafford Metropolitan Borough - Wigan Metropolitan Borough Council; Lancashire - Blackburn with Darwen Borough Council – Blackpool Borough Council - Burnley Borough Council - Chorley Borough Council - Fylde Borough Council – Hyndburn Borough Council - Lancashire County Council - Lancaster City Council - Pendle Borough Council – Preston City Council - Ribble Valley Borough Council - Rossendale Borough Council - South Ribble Borough Council - West Lancashire Borough Council - Wyre Borough Council; Merseyside - Knowsley Metropolitan Borough Council - Liverpool City Council - Sefton Council - St Helens Metropolitan Borough Council - Wirral Metropolitan Borough Council; Police Authorities - Cumbria Police Authority - Lancashire Police Authority - Merseyside -

Proposed Free School – Opening September 2018 Report on Section 10 Public Consultation 9Th June 2017-8Th September 2017
Laurus Ryecroft Proposed free school – opening September 2018 Report on Section 10 public consultation th th 9 June 2017-8 September 2017 laurustrust.co.uk 4 October 17 Page 1 of 21 Contents Executive summary ............................................................................................................... 3 The proposer group ............................................................................................................... 4 Initial phase ........................................................................................................................... 4 Statutory consultation ............................................................................................................ 6 Stakeholders ......................................................................................................................... 7 Statutory consultation results and responses ........................................................................ 9 Other responses to the consultation .................................................................................... 18 Conclusion and next steps .................................................................................................. 21 Appendices: Appendix 1 – Section 10 consultation information booklet Appendix 2 – Consultation questionnaire Appendix 3 – Promotional material Appendix 4 – Stakeholders laurustrust.co.uk 4 October 17 Page 2 of 21 Executive summary Laurus Ryecroft is a non-selective, non-denominational 11-18 secondary school in the pre-opening -
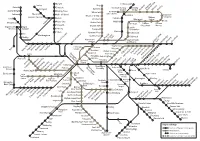
Wayfarer Rail Diagram 2020 (TPL Spring 2020)
Darwen Littleborough Chorley Bury Parbold Entwistle Rochdale Railway Smithy Adlington Radcliffe Kingsway Station Bridge Newbold Milnrow Newhey Appley Bridge Bromley Cross Business Park Whitefield Rochdale Blackrod Town Centre Gathurst Hall i' th' Wood Rochdale Shaw and Besses o' th' Barn Crompton Horwich Parkway Bolton Castleton Oldham Orrell Prestwich Westwood Central Moses Gate Mills Hill Derker Pemberton Heaton Park Lostock Freehold Oldham Oldham Farnworth Bowker Vale King Street Mumps Wigan North Wigan South Western Wallgate Kearsley Crumpsall Chadderton Moston Clifton Abraham Moss Hollinwood Ince Westhoughton Queens Road Hindley Failsworth MonsallCentral Manchester Park Newton Heath Salford Crescent Salford Central Victoria and Moston Ashton-underStalybridgeMossley Greenfield -Lyne Clayton Hall Exchange Victoria Square Velopark Bryn Swinton Daisy HillHag FoldAthertonWalkdenMoorside Shudehill Etihad Campus Deansgate- Market St Holt Town Edge Lane Droylsden Eccles Castlefield AudenshawAshtonAshton Moss West Piccadilly New Islington Cemetery Road Patricroft Gardens Ashton-under-Lyne Piccadilly St Peter’s Guide Weaste Square ArdwickAshburys GortonFairfield Bridge FloweryNewton FieldGodley for HydeHattersleyBroadbottomDinting Hadfield Eccles Langworthy Cornbrook Deansgate Manchester Manchester Newton-le- Ladywell Broadway Pomona Oxford Road Belle Vue Willows HarbourAnchorage City Salford QuaysExchange Quay Piccadilly Hyde North MediaCityUK Ryder Denton Glossop Brow Earlestown Trafford Hyde Central intu Wharfside Bar Reddish Trafford North -

794 Rot-Row :Manchester Suburban [Slater's
794 ROT-ROW :MANCHESTER SUBURBAN [SLATER'S Rothwell Williarn, policeman, Police station, Ellesmere Ro"e Charles H. coach builder, 32 Stovell road, M strePt, Pendlebury Rowe Clan~ (1hs.), householder, 12 Lime street, L RothwPll William Hy. confectioner, 267 Stockpmt rd. L Rowe Herbert H. telegraphisb, 40 Silton st. Ashley la. M Rottenbury Robert, ti.t:J:er, 219 Walkden road, 'Yorsley Rowe John, householder, 32 Birch avePue, Heaton Moor Roughley James, cashier, 429 Worsley road, Wmton Rowe Joseph, carter, 30 Denm<~rk street, A Rrmahley John Hy. corn. traveller, 15 IIaddon gro. Sale Rowe Robert, engineer, 38 Carlton road, A on ~~ Roughly Eliza (Mrs.), shopl_•eeper, II Albion st.P~~dle~ry Rowe Rosalinc (Sirs.), householder, 220 .Moseley rd. F Rough sedge Harry, compositor, g Hard man la.F ails~ rth Rowe William warper, 294 Walkden road, Worsley Roughton Horace, coach proprietor, 12 Manchester rd. ; Howerth John: brass finisher, 214 Worsley road, Win ton res. 6 ~lshfield road, Cheadle RowLmd B. R. & Co. Limited, engineers, Climax works, Roughton Wm. electrical engineer, 26 1Vilson st.Strctfrd Sandfold lane, :Sorth Reddish. T N 47 Heaton .\[oor Rou'n.<t .Annie E. (Mrs.), dress maker, 39 Gild a Brk. rd. E Rowland Benjamin, miller, 39 Brcntwood road, 'I' R und Bcnjamin Charles, householder, 9 Booth street, Howland David, joiner, 45 Didsbury road, Heaton Norris Rovle street, Denton Row land Eleanor (.\>Irs. ), hsehldr. 896 Chester rd. Stretfi d Ronr"ke Ann (~Irs.), househldr. 15 Cobden st.Water la.D Rowland George Herbcrt, houschldr. 8 Charlton road, L Rou rke Ann (Mrs.), househldr. 7 Sa lis bmy st. -

Ryecroft Hall Audenshaw
DENTON & AUDENSHAW DISTRICT ASSEMBLY RYECROFT HALL AUDENSHAW MANAGEMENT PLAN 2007/2011 1 CCOONNTTEENNTTSS PPaaggee 1. Tameside’s vision for Ryecroft 3 2. Site Details 4 3. Strategic Context 11 4. A Welcoming Place 17 5. Healthy, Safe and Secure 18 6. Clean and Well Maintained 21 7. Sustainability 23 8. Conservation and Heritage 26 9. Community Involvement 28 10. Marketing 31 11. Management 33 2 1. Tameside’s vision for Ryecroft “We want Tameside to be an attractive and environmentally friendly place to live, work and visit. We are committed to working with local communities to protect and improve our surroundings to make Tameside a cleaner and more accessible place for current and future generations”. This statement is the District Assembly’s vision for the future of Ryecroft Hall. The statement is taken from Tameside’s Community Strategy 2003/ 2013 where one of the key themes is ‘An Attractive Borough’ and was identified via extensive consultation with both local residents and businesses. The basis for managing and improving Ryecroft Hall are the eight standards set out in the Green Flag criteria, which are: • A Welcoming Place • Conservation and Heritage • Healthy, Safe and Secure • Community Involvement • Clean and Well Maintained • Marketing • Sustainability • Management As part of this vision we are committed to year on year improvements to our Parks and open spaces. 3 2. Site Details Name: Ryecroft Hall Contact: Nick Sayers, Assistant Town Manager Denton and Audenshaw District Assembly Market Street Denton M34 2AP Location: Grid Reference: 391453: 397817 Map Reference: SJ9197NW Ryecroft Hall is situated in Audenshaw between Droylsden and AshtonUnderLyne Area: 2.549 Hectares Tenure: The land is owned by Tameside Metropolitan Borough Council. -

20/00559/FUL Proposal
Application Number: 20/00559/FUL Proposal: Conversion of existing two storey workshop building to form two dwelling houses, demolition of existing single storey workshop building and erection of two single storey bungalows with associated works including car parking. Site: 218 Audenshaw Road, Audenshaw, M34 5QR Applicant: Mr D Ross Recommendation: Grant planning permission subject to conditions. Reason for report: A Speakers Panel decision is required because one of the objectors to the application has requested to address the Panel meeting and, in accordance with the Panel’s Terms of Reference, to authorise the utilisation of the Private Street Work Code for the making up of Eastwood Street, a private street, to enable development to take place. 1. APPLICATION DESCRIPTION 1.1 The applicant seeks full planning permission for the conversion of the existing two storey workshop building to form two dwelling houses and the erection of two single storey bungalows following the demolition of existing single storey workshop building. The proposals also include associated works including the provision of car parking. 1.2 The scheme has been amended to reduce the number of dwellings by two, with the original scheme proposing to replace the existing single storey workshop with four bungalows. The proposals include the erection of a relatively narrow 1.5 storey lean-to extension on the southern elevation of the mill as part of the conversion of that building. 1.3 The mix of the dwellings in the proposed scheme would be as follows:- 2 x 2 bed single storey bungalows 2 x 3 bed 2 storey houses 1.4 The following documents have been submitted in support of the planning application:- - Planning Statement - Development Financial Appraisal - Contaminated land screening report (including reference to coal mining legacy) - Preliminary Bat Report - Bat Presence Survey - Noise Impact Assessment 2. -

The Extent of Longdendale 1360 with Introduction and Notes by P.H.W
The Record Society of Lancashire and Cheshire Volume 140: start THE RECORD SOCIETY OF LANCASHIRE AND CHESHIRE FOUNDED TO TRANSCRIBE AND PUBLISH ORIGINAL DOCUMENTS RELATING TO THE TWO COUNTIES VOLUME CXL The Society wishes to acknowledge with gratitude the support given towards publication by The Marc Fitch Fund The Aurelius Foundation Cheshire County Council Lancashire County Council © The Record Society of Lancashire and Cheshire J.H. Harrop P.H.W. Booth S.A. Harrop ISBN 0 902593 63 3 Printed in Great Britain by J. W. Arrowsmith Ltd. Extenta dominii de Longdendale anno xxxiiif Edwardi tercij EXTENT OF THE LORDSHIP OF LONGDENDALE 1360 Edited by John Harrop with Paul Booth and Sylvia Harrop PRINTED FOR THE SOCIETY 2005 FOR THE SUBSCRIPTION YEAR 2002 COUNCIL AND OFFICERS FOE THE YEAR 2002 President Jenny Kermode, B.A., Ph.D. Hon. Council Secretary Dorothy J. Clayton, M.A., Ph.D., A.L.A., F.R.Hist.S., c/o John Rylands University Library of Manchester, Oxford Road, Manchester M l3 9PP Hon. Membership Secretary Maureen Barber, B.A., D.L.A., 7 Rosebank, Lostock, Bolton BL6 4PE Hon. Treasurer and Publications Secretary Fiona Pogson, B.A., Ph.D., c/o Department of History, Liverpool Hope University College, Hope Park, Liverpool L16 9JD Hon. General Editor Philip Morgan, B.A., Ph.D., F.R.Hist.S. (from March 2002 Peter McNiven, M.A., Ph.D., F.R.Hist.S., The Vicarage, 1 Heol Mansant, Pontyates, Llanelli, Carmarthenshire SA15 5SB) Other Members of the Council Diana E.S. Dunn, B.A., D.Ar. Studies B.W.