Current Status of Skeletal Anchorage Dental Applications in Orthodontics, Part II
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Treatment Options for Jaw Growth Variations
TREATMENT OPTIONS FOR JAW GROWTH VARIATIONS An Editorial by Robert M. Mason, DMD, PhD PROBLEMS OF OVERGROWTH OF A JAW: It is well known among orthodontists that where there is a growth process involving overgrowth of a jaw, the rule is that growth should be allowed to proceed and then treat the situation after growth has ceased. The reason for this is that growth cannot be effectively stopped or otherwise modified to the extent that jaw growth can be overpowered; that is, “Mother Nature” is smarter than any of us in dentistry. What can be accomplished with an overgrowth of a jaw, however, is orthodontic “remodeling” of some of the parts which are expressing overgrowth. An example is a Class III “growing” mandible. Functional appliances, such as the Frankel or Bionator, can influence the shape of the growing mandible by remodeling, which may give the appearance of manipulating growth, while instead, long-term studies show that such jaw shape changes are only temporary. Over time, the overgrowth pattern returns. Hence, the orthodontic caveat: it is best to let a mandible grow to its full extent and then treat it either by a combination of jaw surgery and orthodontics, or orthodontics alone which may amount to “camouflaging” the problem. What happens dentally in the example of overgrowth of the mandible is that in an attempt for the body to try to maintain dental contacts, the lower incisors tip lingually and the upper incisors tip labially (facially) in an attempt to maintain anterior dental contact relationships as lower jaw growth continues. If the treatment decision is to try to correct the problem with orthodontics alone, Class III elastics would be used along with orthodontic fixed appliances to maintain the lingual tipping and maxillary flaring of incisors. -
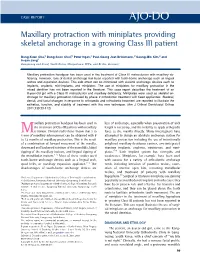
Maxillary Protraction with Miniplates Providing Skeletal Anchorage in a Growing Class III Patient
CASE REPORT Maxillary protraction with miniplates providing skeletal anchorage in a growing Class III patient Bong-Kuen Cha,a Dong-Soon Choi,b Peter Ngan,c Paul-Georg Jost-Brinkmann,d Soung-Min Kim,e and In-san Jangf Gangneung and Seoul, South Korea, Morgantown, WVa, and Berlin, Germany Maxillary protraction headgear has been used in the treatment of Class III malocclusion with maxillary de- ficiency. However, loss of dental anchorage has been reported with tooth-borne anchorage such as lingual arches and expansion devices. This side effect can be minimized with skeletal anchorage devices such as implants, onplants, mini-implants, and miniplates. The use of miniplates for maxillary protraction in the mixed dentition has not been reported in the literature. This case report describes the treatment of an 8-year-old girl with a Class III malocclusion and maxillary deficiency. Miniplates were used as skeletal an- chorage for maxillary protraction followed by phase 2 orthodontic treatment with fixed appliances. Skeletal, dental, and facial changes in response to orthopedic and orthodontic treatment are reported to illustrate the esthetics, function, and stability of treatment with this new technique. (Am J Orthod Dentofacial Orthop 2011;139:99-112) axillary protraction headgear has been used in loss of anchorage, especially when preservation of arch Mthe treatment of Class III patients with maxillary length is necessary, and the inability to apply orthopedic retrusion. Clinical studies have shown that 2 to force to the maxilla directly. Many investigators have 4 mm of maxillary advancement can be obtained with 8 attempted to design an absolute anchorage system for to 12 months of maxillary protraction. -

Non-Surgical Treatment of an Adult Class III Malocclusion Patient with Facial Asymmetry by Unilateral Mandibular Arch Distalization
Volume 29 Issue 2 Article 4 2017 Non-surgical Treatment of an Adult Class III Malocclusion Patient with Facial Asymmetry by Unilateral Mandibular Arch Distalization Chi-Yu Tsai Department of Orthodontics, Kaohsiung Chang Gung Memorial Hospital, Chang Gung University College of Medicine, Kaohsiung, Taiwan Shiu-Shiung Lin Department of Orthodontics, Kaohsiung Chang Gung Memorial Hospital, Chang Gung University College of Medicine, Kaohsiung, Taiwan Yi-Hao Lee Department of Orthodontics, Kaohsiung Chang Gung Memorial Hospital, Chang Gung University College of Medicine, Kaohsiung, Taiwan Li-Tyng Sun Department of Orthodontics, Kaohsiung Chang Gung Memorial Hospital, Chang Gung University College of Medicine, Kaohsiung, Taiwan Yu-Jen Chang Department of Orthodontics, Kaohsiung Chang Gung Memorial Hospital, Chang Gung University College Fofollow Medicine, this and Kaohsiung, additional T aiwanworks at: https://www.tjo.org.tw/tjo Part of the Orthodontics and Orthodontology Commons See next page for additional authors Recommended Citation Tsai, Chi-Yu; Lin, Shiu-Shiung; Lee, Yi-Hao; Sun, Li-Tyng; Chang, Yu-Jen; and Wu, Te-Ju (2017) "Non-surgical Treatment of an Adult Class III Malocclusion Patient with Facial Asymmetry by Unilateral Mandibular Arch Distalization," Taiwanese Journal of Orthodontics: Vol. 29 : Iss. 2 , Article 4. DOI: 10.30036/TJO.201706_29(2).0004 Available at: https://www.tjo.org.tw/tjo/vol29/iss2/4 This Case Report is brought to you for free and open access by Taiwanese Journal of Orthodontics. It has been accepted for inclusion -

Relationship Between Skeletal Class II and Class III Malocclusions with Vertical Skeletal Pattern
original article Relationship between skeletal Class II and Class III malocclusions with vertical skeletal pattern Sonia Patricia Plaza1, Andreina Reimpell1, Jaime Silva1, Diana Montoya1 DOI: https://doi.org/10.1590/2177-6709.24.4.063-072.oar Objective: The purpose of this study was to establish the association between sagittal and vertical skeletal patterns and assess which cephalometric variables contribute to the possibility of developing skeletal Class II or Class III malocclusion. Methods: Cross-sec- tional study. The sample included pre-treatment lateral cephalogram radiographs from 548 subjects (325 female, 223 male) aged 18 to 66 years. Sagittal skeletal pattern was established by three different classification parameters (ANB angle, Wits and App-Bpp) and vertical skeletal pattern by SN-Mandibular plane angle. Cephalometric variables were measured using Dolphin software (Imaging and Management Solutions, Chatsworth, Calif, USA) by a previously calibrated operator. The statistical analysis was carried out with Chi-square test, ANOVA/Kruskal-Wallis test, and an ordinal multinomial regression model. Results: Evidence of associa- tion (p < 0.05) between sagittal and vertical skeletal patterns was found with a greater proportion of hyperdivergent skeletal pattern in Class II malocclusion using three parameters to assess the vertical pattern, and there was more prevalent hypodivergence in Class III malocclusion, considering ANB and App-Bpp measurements. Subjects with hyperdivergent skeletal pattern (odds ratio [OR]=1.85- 3.65), maxillary prognathism (OR=2.67-24.88) and mandibular retrognathism (OR=2.57-22.65) had a significantly (p < 0.05) greater chance of developing skeletal Class II malocclusion. Meanwhile, subjects with maxillary retrognathism (OR=2.76-100.59) and man- dibular prognathism (OR=5.92-21.50) had a significantly (p < 0.05) greater chance of developing skeletal Class III malocclusion. -

Understanding Anchorage in Orthodontics-Review Article
Open Access Journal of Dentistry & Oral Disorders Review Article Understanding Anchorage in Orthodontics-Review Article Nahidh M1*, Al Azzawi AM2 and Al-Badri SC3 1Department of Orthodontics, College of Dentistry, Abstract University of Baghdad, Iraq Before starting active treatment of any orthodontic case, anchorage must 2Department of POP, College of Dentistry, University of be planned well to get rid of the problems that might accompanied the treatment Babylon, Iraq procedures. This article reviewed the anchorage from all aspects starting from 3Specialist Orthodontist, Ministry of Health, Baghdad, the definition, sources, types, planning, anchorage loss and how to avoid it. Iraq *Corresponding author: Mohammed Nahidh, Department of Orthodontics, College of Dentistry, University of Baghdad, Iraq Received: September 10, 2019; Accepted: October 23, 2019; Published: October 30, 2019 Definition • Mandibular symphysis According to the third law of Newton, for every action there • Back of the neck (cervical bone) is a reaction equals in amount and opposite in direction. This can A. Intra-oral sources of anchorage be applied in orthodontics simply when retracting canine against posterior teeth. The expected thing is distalization of the canine in the Teeth: In orthodontics, teeth themselves are the most frequently first premolar extraction site against mesial (forward) movement of used anchorage unit to resist unwanted movement. Forces can be the posterior teeth which called anchorage unit. exerted from one set of teeth to move certain other teeth. Many factors related to the teeth can influence the anchorage like: the root According to Graber [1], the term anchorage is referred as “the form, the size (length) of the roots, the number of the roots, the nature and degree of resistance to displacement offered by an anatomic anatomic position of the teeth, presence of ankylosed tooth, the axial unit when used for the purpose of affecting tooth movement”, while inclination of the teeth, root formation, contact points of teeth and Gardiner et al. -
I Skeletal Class I Malocclusion
Orthopedic appliance Dr. K. Ravi, MDS, Prof , HOD &Dean , Department of Orthodontics, SRM Dental College. Contents of the lecture • Definition of Orthopaedic appliance • Difference between orthopaedic & orthodontic appliance • Types of orthopaedic appliance • Indications an overview • Head gears • Reverse pull Head gear • Chin cup Orthopaedic appliance • Orthopaedic appliances are appliances that exert orthopaedic force and bring about bony changes . • They are growth modification appliances given in the growing stage of the individuals with skeletal malocclusion. • There are three type of orthopaedic appliances – Head gear – Reverse pull head gear ( Face mask ) – Chin cup Difference between Orthopaedic appliance & Orthodontic appliance Orthopaedic appliance Orthodontic appliance Exert orthopaedic force Exert orthodontic force Heavy intermittent force Low continuous force Greater than 400gms Lesser than 400gms Skeletal changes Dental changes Head gear Hawley's appliance Face mask or Reverse pull HG Begg appliance Chin Cup Straight wire appliance Malocclusion Skeletal Dental Growth Surgical Camouflage Hawley's appliance ,Begg modification in intervention in Appliance & Straight wire growing patients Less severe adults appliance Skeletal Class II Head gear – Maxillary prognathism Functional appliance – Mandibular retrognathism Skelatal Class III Reverse pull HG or face mask for maxillary retrognathism chin cup for mandibular prognathism Constricted maxilla Rapid maxillary expansion appliance Head gear – Maxillary prognathism (Skeletal class II Malocclusion) . Head gears are used in skeletal class II Cases with maxillary prognathism Indications . Restriction of maxillary growth . With a maxillary acrylic splint . With functional appliances . Treating gummy smile . Fixed appliance for preserving anchorage in the upper arch Mechanism of action . Head gears restrict the growth of maxilla by restricting the suture at circummaxillary sutures. -

Effects of Maxillary Protraction with Skeletal Anchorage and Petit-Type Facemask in High-Angle Class III Patients
Original Article DOI: 10.7860/JCDR/2020/43419.13587 Effects of Maxillary Protraction with Skeletal Dentistry Section Anchorage and Petit-Type Facemask in High-Angle Class III Patients: A Retrospective Study BURAK KALE1, MUHAMMED HILMI BUYUKCAVUS2 ABSTRACT for 12 hours a day. Cephalometric measurements were made Introduction: Skeletal anchorage-supported applications are to evaluate the effects of the maxillary protraction. The paired performed to increase the skeletal effect of maxillary protraction t-test was applied to evaluate differences between pre- and used in the treatment of Class III malocclusions related to posttreatment variables. maxillary retrognathia. Results: In our study, the skeletal Class III relationships were Aim: To assess the craniofacial and soft tissue effects of the improved; maxillary measurements significantly increased maxillary protraction with skeletal anchorage and Petit-type (SNA° 3.48±0.42°; A–VRL 3.94±0.81 mm), SNB° decreased facemask in high-angle growth Class III young adolescent (-0.50±0.30°), ANB° increased (3.85±0.46°) (p<0.001) and SN- patients due to maxillary retrognathia. GoGn° slightly increased (0.25±0.21°) (p>0.05). The maxillary and mandibular incisors showed retroclination (-3.12±0.42° Materials and Methods: The archives for this retrospective p<0.01;-0.46±0.24°; respectively). The changes in skeletal study were scanned according to inclusion criteria as follows: and dental parameters caused a significant increase in overjet skeletal Class III malocclusion due to maxillary retrognathia, (3.56±1.01 mm; p<0.001). high-angle growth pattern, treated using face mask with miniplate anchorage. This study consisted of 15 patients Conclusion: Using skeletal anchorage with Petit-type (7 females and 8 males; mean age,11.96±1.03 years) treated facemask has been successfully treated in patients with using Petit-type face mask with miniplate anchorage inserted high-angle Class III young adolescent patients that provided in maxillae. -
CASE REPORT “Surgery-First” Approach with Invisalign Therapy to Correct a Class II Malocclusion and Severe Mandibular Retrognathism
@2019 JCO, Inc. May not be distributed without permission. www.jco-online.com CASE REPORT “Surgery-First” Approach with Invisalign Therapy to Correct a Class II Malocclusion and Severe Mandibular Retrognathism JOY CHANG, BS, DDS, MDS DEREK STEINBACHER, DMD, MD RAVINDRA NANDA, BDS, MS, PhD FLAVIO URIBE, DDS, MDS or patients with severe skeletal jaw discrepancies, the combination of orthodontics with orthognathic surgery is often the only approach that Fcan both harmonize facial esthetics and restore functional occlusion.1 Unfortunately, conventional presurgical orthodontics involves a lengthy de- compensation period that worsens the patient’s facial appearance and ex- acerbates the malocclusion.2,3 Many patients pursuing surgical-orthodontic treatment are adults who wish to avoid a deterioration in their profile and facial appearance during presurgical orthodontics.4 Dr. Chang Dr. Steinbacher Dr. Nanda Dr. Uribe Dr. Chang is a former Resident; Dr. Nanda is Professor Emeritus; and Dr. Uribe is an Associate Professor, Postgraduate Program Director, and Charles J. Burstone Endowed Professor, Division of Orthodontics, Department of Craniofacial Sciences, University of Connecticut School of Dental Medicine, Farmington, CT. Dr. Steinbacher is an Associate Professor of Plastic Surgery, Assistant Professor of Pediatrics, and Director of Dental Services, Oral Maxillofacial and Craniofacial Surgery, Yale School of Medicine, New Haven, CT. Dr. Chang is in the private practice of ortho- dontics in San Jose, CA. Dr. Nanda is also an Associate Editor and Dr. Uribe is a Contributing Editor of the Journal of Clinical Orthodontics. E-mail Dr. Uribe at [email protected]. VOLUME LIII NUMBER 7 © 2019 JCO, Inc. 397 SURGERY-FIRST WITH INVISALIGN TO CORRECT CLASS II MALOCCLUSION Fig. -

Invisalign Treatment Planning Guide 1 Align Technology, Inc
Table of Contents INTRODUCTION . 2 Getting Quality Clinical Outcomes with Invisalign. 2 Invisalign Applicability . 3 DIAGNOSIS AND TREATMENT OPTIONS 1. Crowding . 4 2. Spacing. 10 3. Narrow Arches . 16 4. Crossbite. 20 5. Deep Bite . 24 6. Open Bite . 28 7. Class II . 32 Invisalign 8. Class III . 38 CLINICAL NOTES Treatment IPR . 5 Tooth Size Discrepancy . 11 Planning Staging . 12 Auxiliary Treatment. 12 Guide Expansion . 17 Attachments. 25 Anchorage . 42 APPENDIX Prescription Form Tips. 44 Glossary . 46 Index. 48 Credits . 54 Invisalign Treatment Planning Guide 1 Align Technology, Inc. Introduction HOW TO USE THIS GUIDE Getting Quality Clinical The guide is organized by patient diagnosis. ABOUT THIS GUIDE Match your patient’s diagnosis to the appropriate Outcomes with Invisalign The goal of this guide is to provide you with a diagnosis decision tree to see some possible treat- decision making tool you can use while selecting ment options. Read the accompanying treatment Successful clinical outcomes with Invisalign and treatment planning your Invisalign cases. notes and evaluate your options given your start with attention to detail during case By outlining typically used Invisalign approaches Invisalign experience level. See Figure A, below. selection and treatment planning. Here are and discussing their complexity and predict- five guidelines for setting up your cases that ABOUT THIS SERIES ability, we hope to make the treatment planning pay great dividends later: This guide is the first in a three-part series options and implications more clear for you of Invisalign patient care references, comple- to evaluate. 1. Submit high quality records. Accurate menting the ClinCheck® Evaluation Guide PVS impressions and clear patient photos and (D4458) and the Invisalign Clinical Monitoring Align Technology is not a provider of medical, radiographs are critical for the creation of your Guide (D4219). -

Comprehensive Orthodontic Cases (Children and Adults Treated with Braces)
Comprehensive Orthodontic Cases (Children and Adults Treated with Braces) Cases Treated by: Bella Shen Garnett, DMD, MMSc Initial Final Age: 16 – Male Severe protrusion 12mm overjet treated non-extraction and non- surgical Appliance: Braces with Herbst Treatment Length: 23 months Treated by Dr. Bella Shen Garnett Initial Final Age 11 years old - Female Spacing / Impacted Canine and Second molars in buccal crossbite Treatment Length: 19 months Treated by Dr. Bella Shen Garnett Initial Final Age: 26 Spacing and occlusal cant Treatment Length: 15 months Treated by Dr. Bella Shen Garnett Initial Final Age: 33 Relapse from previous orthodontic treatment Open bite with tongue thrust Braces with tongue spurs to train tongue thrust to prevent bite opening Treatment Length: 14 months Treated by Dr. Bella Shen Garnett Initial Final Patient missing lateral incisors #7, 10 Spaces were opened for implants and the smile was made broader Treatment Time: 18 months Treated by Dr. Bella Shen Garnett Initial Final Adult male presents with severe crowding Extracted all first bicuspids Treatment Length: 21 months Treated by Dr. Bella Shen Garnett Initial Final Adult male presents with a deep bite Class II malocclusion Treated non-extraction with braces and bite turbos Treatment length: 16 months Treated by Dr. Bella Shen Garnett Intial Final 14 Year old female Class II on the left and 5mm overjet Treated with Braces and a Pendex (Expand and distalized upper posterior teeth) Treatment Length: 14 Months Treated by Dr. Bella Shen Garnett Initial Final 55 Year old female presents with an underbite and severe bone loss around lower right canine due to fremitus Treated with braces and elastics and veneers by dentist post ortho Treatment length: 15 Months Treated by Dr. -

Anchorage in Orthodontics: a Literature Review
Review article Annals and Essences of Dentistry 5368/aedj.2016.8.2.3.2 ANCHORAGE IN ORTHODONTICS: A LITERATURE REVIEW 1 Siva Krishna P 1 Post graduate 2 Prasad Mandava 2 Professor and Head 3 Gowri sankar Singaraju 3 Professor 4 Vivek Reddy Ganugapanta 4 Reader 1-4 Department of Orthodontics, Narayana Dental College, Nellore, Andhra Pradesh, India. ABSTRACT Abstract : During orthodontic treatment the teeth are exposed to forces and moments, and these acting forces always generate reciprocal forces of the same magnitude but opposite in direction which follows Newton’s third law. To avoid unwanted tooth movements and maintain treatment success, these reciprocal forces must be diverted effectively. In orthodontic treatment, anchorage loss is a potential side effect of orthodontic mechanotherapy and one of the major causes of unsuccessful results. Its cause has been described as a multifactorial response in relation to the extraction site, appliance type, age, crowding, and overjet.Therefore, clinicians throughout the years have made an effort to find biomechanical solutions to control anchorage. The purpose of this article is to review the basics of anchorage and the anchorage planning in different appliance systems. KEYWORDS: Anchorage, Anchor loss, Anchorage planning in different appliance systems. INTRODUCTION Anchorage is the word used in orthodontics to mean and comfortable could make appliance design simplified resistance to displacement. Every orthodontic appliance and more efficient. consists of two elements an active element and a resistance element. The active parts of the orthodontic The present article will focus on anchor saving appliance are concerned with tooth movements. The measures and anchorage concepts in different appliance resistance units provide resistance (anchorage) that systems in orthodontics. -

Effectiveness and Stability of Anterior Open Bite Correction Using Temporary Skeletal Anchorage: Comparison to Surgical Outcomes
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by Carolina Digital Repository EFFECTIVENESS AND STABILITY OF ANTERIOR OPEN BITE CORRECTION USING TEMPORARY SKELETAL ANCHORAGE: COMPARISON TO SURGICAL OUTCOMES by J. Turner Hull A thesis submitted to the faculty of the University of North Carolina at Chapel Hill in partial fulfillment of the requirements for the degree of Master of Science in the Department of Orthodontics. Chapel Hill 2009 Approved by: Advisor: J.F. Camilla Tulloch Reader: Ceib Phillips Reader: Timothy Turvey Reader: Nicole Scheffler © 2008 J. Turner Hull, DDS ALL RIGHTS RESERVED ii ABSTRACT J. TURNER HULL: Effectiveness and Stability of Anterior Open Bite Correction Using Temporary Skeletal Anchorage: Comparison to Surgical Outcomes (Under the direction of Dr. Camilla Tulloch) The skeletal and dental changes that occur following the intrusion of maxillary posterior teeth with temporary skeletal anchorage (TSA) and the stability of these changes over time were assessed in twelve patients (1 male, 11 females) with anterior open bite. A comparative sample of patients treated with maxillary osteotomy was frequency matched based on age and gender. Lateral cephalograms were obtained before treatment/surgery, at the end of treatment/post-surgery, and at least 6 months following the completion of treatment. All pretreatment measurements except overbite were similar, on average, between the two treatment groups. Positive overbite was achieved for all patients treated with TSA’s (Pre-tx OB x = -1.0mm, Post-tx OB x = 2.7mm). Both groups showed a similarly small average change during the follow-up time period.