Colon Terms and Definitions Colon Terms and Definitions
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
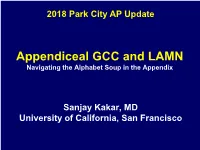
Appendiceal GCC and LAMN Navigating the Alphabet Soup in the Appendix
2018 Park City AP Update Appendiceal GCC and LAMN Navigating the Alphabet Soup in the Appendix Sanjay Kakar, MD University of California, San Francisco Appendiceal tumors Low grade appendiceal mucinous neoplasm • Peritoneal spread, chemotherapy • But not called ‘adenocarcinoma’ Goblet cell carcinoid • Not a neuroendocrine tumor • Staged and treated like adenocarcinoma • But called ‘carcinoid’ Outline • Appendiceal LAMN • Peritoneal involvement by mucinous neoplasms • Goblet cell carcinoid -Terminology -Grading and staging -Important elements for reporting LAMN WHO 2010: Low grade carcinoma • Low grade • ‘Pushing invasion’ LAMN vs. adenoma LAMN Appendiceal adenoma Low grade cytologic atypia Low grade cytologic atypia At minimum, muscularis Muscularis mucosa is mucosa is obliterated intact Can extend through the Confined to lumen wall Appendiceal adenoma: intact muscularis mucosa LAMN: Pushing invasion, obliteration of m mucosa LAMN vs adenocarcinoma LAMN Mucinous adenocarcinoma Low grade High grade Pushing invasion Destructive invasion -No desmoplasia or -Complex growth pattern destructive invasion -Angulated infiltrative glands or single cells -Desmoplasia -Tumor cells floating in mucin WHO 2010 Davison, Mod Pathol 2014 Carr, AJSP 2016 Complex growth pattern Complex growth pattern Angulated infiltrative glands, desmoplasia Tumor cells in extracellular mucin Few floating cells common in LAMN Few floating cells common in LAMN Implications of diagnosis LAMN Mucinous adenocarcinoma LN metastasis Rare Common Hematogenous Rare Can occur spread -

Crohn's Disease of the Colon
Gut, 1968, 9, 164-176 Gut: first published as 10.1136/gut.9.2.164 on 1 April 1968. Downloaded from Crohn's disease of the colon V. J. McGOVERN AND S. J. M. GOULSTON From the Royal Prince Alfred Hospital, Sydney, Australia The fact that Crohn's disease may involve the colon never affected unless there had been surgical inter- either initially or in association with small bowel ference. There was no overt manifestation of mal- disease is now firmly established due largely to the absorption in any of these patients. evidence presented by Lockhart-Mummery and In 18 cases the colon alone was involved. Five had Morson (1960, 1964) and Marshak, Lindner, and universal involvement, five total involvement with Janowitz (1966). This entity is clearly distinct from sparing of the rectum, two involvement of the ulcerative colitis and other forms of colonic disease. descending colon only, two the transverse colon only, Our own experience with this disorder reveals many and in the other four there was variable involvement similarities with that published from the U.K. and of areas of large bowel (Fig. 2). the U.S.A. Thirty patients with Crohn's disease involving the large bowel were seen at the Royal CLINICAL FEATURES Prince Alfred Hospital during the last decade, the majority during the past five years. The criteria for The age incidence varied from 6 to 69 years when the inclusion were based on histological examination of patient was first seen, the majority being between the operative specimens in 28 and on clinical and radio- ages of 11 and 50. -

Carcinomatous Cirrhosis of the Liver with Sarcomatosis of the Peritoneum 1
CARCINOMATOUS CIRRHOSIS OF THE LIVER WITH SARCOMATOSIS OF THE PERITONEUM 1 S. SANES, M.D., AND K. TERPLAN, M.D. (From tile Pathological Laboratory of the Buffalo General Hospital and School of Medicine, University of Buffalo) The following case is reported because of the occurrence of two different types of malignant neoplasm with typical portal cirrhosis of the liver. That a pathogenetic relationship exists between Laennec's cirrhosis and primary carcinoma of the liver is generally recognized. Whether the association of a peritoneal sarcoma with the cirrhosis in this case was more than a coincidence seemed an interesting point for discussion. REPORT OF CASE E. G., 11 white Italian male fifty-seven years old, was admitted to the Buffalo General Hospital on the service of Drs. N. G. Russell and A. H. Aaron, Nov. 25, 1934. He died Nov. 29, 1934. All his adult life he had partaken of large amounts of wine and whiskey daily. At the age of seventeen years he had suffered an attack of jaundice of several weeks' duration. The patient first began to lose weight and strength in 1932 and noticed that his skin was becoming dark. In March 1934 he complained of cramp-like abdominal pain, diarrhea, and bloating. The stools were watery. There was no nausea or vomiting. Upon hos pitalization, April 9, 1934, physical examination revealed that the pupils reacted to light and accommodation. The chest was emphysematous; breath sounds were diminished in both bases. The heart was regular; a systolic murmur was heard. The blood pressure was 118/70. The liver and spleen were palpable three finger breadths below the costal margin. -

7) Anatomy of OMENTUM
OMENTUM ANATOMY DEPARTMENT DR.SANAA AL-SHAARAWY Dr. Essam Eldin Salama OBJECTIVES • At the end of the lecture the students must know: • Brief knowledge about peritoneum as a thin serous membrane and its main parts; parietal and visceral. • The peritonial cavity and its parts the greater sac and the lesser sac (Omental bursa). • The peritoneal folds : omenta, mesenteries, and ligaments. • The omentum, as one of the peritonial folds • The greater omentum, its boundaries, and contents. • The lesser omentum, its boundaries, and contents. • The omental bursa, its boundaries. • The Epiploic foramen, its boundaries. • Mesentery of the small intestine, and ligaments of the liver. • Nerve supply of the peritoneum. • Clinical points. The peritoneum vIs a thin serous membrane, §Lining the wall of the abdominal and pelvic cavities, (the parietal peritoneum). §Covering the existing organs, (the visceral peritoneum). §The potential space between the two layers is the peritoneal cavity. Parietal Visceral The peritoneal Cavity vThe peritoneal cavity is the largest one in the body. vDivisions of the peritoneal cavity : §Greater sac; extends from Lesser Sac diaphragm down to the pelvis. §Lesser sac; lies behind the stomach. §Both cavities are interconnected through the epiploic foramen. §In male : the peritoneum is a closed sac . §In female : the sac is not completely closed because it Greater Sac communicates with the exterior through the uterine tubes, uterus and vagina. The peritoneum qIntraperitoneal and Intraperitoneal viscera retroperitoneal organs; describe the relationship between various organs and their peritoneal covering; §Intraperitonial structure; which is nearly totally covered by visceral peritoneum. §Retroperitonial structure; lies behind the peritoneum, and partially covered by visceral peritoneum. -

The Formation of Peritoneal Adhesions
THE FORMATION OF PERITONEAL ADHESIONS Christian DellaCorte, Ph.D., C.M.T. The increased incidence of postoperative adhesions and their complications has focused attention on trying to understand the adhesion, adhesion formation, clinical consequences, and prevention of adhesion formation. Adhesions are highly differentiated, formed through an intricate process involving a complex organ, the peritoneum, whose surface lining is the key site in adhesion formation. The peritoneum, a serous membrane, serves a protective function for the contents of the abdominal cavity. Homeostasis is maintained by allowing exchange of molecules and production of peritoneal fluid. This provides an environment for optimal function of intra-abdominal organs. Forms of trauma to the peritoneum (i.e., mechanical, thermal, chemical, infectious, surgical, and/or ischemic) can result in the formation of peritoneal adhesions. In 1919, it was shown that peritoneal healing differed from that of skin. When the peritoneal membrane is traumatized, a dynamic response results that produces a series of steps toward rapid regeneration in approximately five to seven days of the injured peritoneum via re-epithelialization, irrespective of the size of injury. Microscopic studies showed the new peritoneal cells are derived from mesodermal cells of the underlying granulation tissue, multipotent mesenchymal cells that are able to take the form of fibroblasts or mesothelial cells. When a defect is made in the parietal peritoneum the entire surface becomes simultaneously epithelialized, differing from the gradual epidermalization from the borders as is found in skin wounds. Multiplication and migration of mesothelial cells from the margins of the wound may play a small part in the regenerative process, but it does not play a major role. -

Nomina Histologica Veterinaria, First Edition
NOMINA HISTOLOGICA VETERINARIA Submitted by the International Committee on Veterinary Histological Nomenclature (ICVHN) to the World Association of Veterinary Anatomists Published on the website of the World Association of Veterinary Anatomists www.wava-amav.org 2017 CONTENTS Introduction i Principles of term construction in N.H.V. iii Cytologia – Cytology 1 Textus epithelialis – Epithelial tissue 10 Textus connectivus – Connective tissue 13 Sanguis et Lympha – Blood and Lymph 17 Textus muscularis – Muscle tissue 19 Textus nervosus – Nerve tissue 20 Splanchnologia – Viscera 23 Systema digestorium – Digestive system 24 Systema respiratorium – Respiratory system 32 Systema urinarium – Urinary system 35 Organa genitalia masculina – Male genital system 38 Organa genitalia feminina – Female genital system 42 Systema endocrinum – Endocrine system 45 Systema cardiovasculare et lymphaticum [Angiologia] – Cardiovascular and lymphatic system 47 Systema nervosum – Nervous system 52 Receptores sensorii et Organa sensuum – Sensory receptors and Sense organs 58 Integumentum – Integument 64 INTRODUCTION The preparations leading to the publication of the present first edition of the Nomina Histologica Veterinaria has a long history spanning more than 50 years. Under the auspices of the World Association of Veterinary Anatomists (W.A.V.A.), the International Committee on Veterinary Anatomical Nomenclature (I.C.V.A.N.) appointed in Giessen, 1965, a Subcommittee on Histology and Embryology which started a working relation with the Subcommittee on Histology of the former International Anatomical Nomenclature Committee. In Mexico City, 1971, this Subcommittee presented a document entitled Nomina Histologica Veterinaria: A Working Draft as a basis for the continued work of the newly-appointed Subcommittee on Histological Nomenclature. This resulted in the editing of the Nomina Histologica Veterinaria: A Working Draft II (Toulouse, 1974), followed by preparations for publication of a Nomina Histologica Veterinaria. -

ABDOMINOPELVIC CAVITY and PERITONEUM Dr
ABDOMINOPELVIC CAVITY AND PERITONEUM Dr. Milton M. Sholley SUGGESTED READING: Essential Clinical Anatomy 3 rd ed. (ECA): pp. 118 and 135141 Grant's Atlas Figures listed at the end of this syllabus. OBJECTIVES:Today's lectures are designed to explain the orientation of the abdominopelvic viscera, the peritoneal cavity, and the mesenteries. LECTURE OUTLINE PART 1 I. The abdominopelvic cavity contains the organs of the digestive system, except for the oral cavity, salivary glands, pharynx, and thoracic portion of the esophagus. It also contains major systemic blood vessels (aorta and inferior vena cava), parts of the urinary system, and parts of the reproductive system. A. The space within the abdominopelvic cavity is divided into two contiguous portions: 1. Abdominal portion that portion between the thoracic diaphragm and the pelvic brim a. The lower part of the abdominal portion is also known as the false pelvis, which is the part of the pelvis between the two iliac wings and above the pelvic brim. Sagittal section drawing Frontal section drawing 2. Pelvic portion that portion between the pelvic brim and the pelvic diaphragm a. The pelvic portion of the abdominopelvic cavity is also known as the true pelvis. B. Walls of the abdominopelvic cavity include: 1. The thoracic diaphragm (or just “diaphragm”) located superiorly and posterosuperiorly (recall the domeshape of the diaphragm) 2. The lower ribs located anterolaterally and posterolaterally 3. The posterior abdominal wall located posteriorly below the ribs and above the false pelvis and formed by the lumbar vertebrae along the posterior midline and by the quadratus lumborum and psoas major muscles on either side 4. -
Small Intestine Cancer Early Detection, Diagnosis, and Staging Detection and Diagnosis
cancer.org | 1.800.227.2345 Small Intestine Cancer Early Detection, Diagnosis, and Staging Detection and Diagnosis Catching cancer early often allows for more treatment options. Some early cancers may have signs and symptoms that can be noticed, but that is not always the case. ● Can Small Intestine Cancer (Adenocarcinoma) Be Found Early? ● Signs and Symptoms of Small Intestine Cancer (Adenocarcinoma) ● Tests for Small Intestine Cancer (Adenocarcinoma) Stages and Outlook (Prognosis) After a cancer diagnosis, staging provides important information about the extent of cancer in the body and anticipated response to treatment. ● Small Intestine Cancer (Adenocarcinoma) Stages ● Survival Rates for Small Intestine Cancer (Adenocarcinoma) Questions to Ask About Small Intestine Cancer Get some questions you can ask your cancer care team to help you better understand your cancer diagnosis and treatment options. ● Questions to Ask Your Doctor About Small Intestine Cancer 1 ____________________________________________________________________________________American Cancer Society cancer.org | 1.800.227.2345 Can Small Intestine Cancer (Adenocarcinoma) Be Found Early? (Note: This information is about small intestine cancers called adenocarcinomas. To learn about other types of cancer that can start in the small intestine, see Gastrointestinal Carcinoid Tumors1, Gastrointestinal Stromal Tumors2, or Non-Hodgkin Lymphoma3.) Screening is testing for diseases like cancer in people who do not have any symptoms. Screening tests can find some types of cancer early, when treatment is most likely to be effective. But small intestine adenocarcinomas are rare, and no effective screening tests have been found for these cancers, so routine testing for people without any symptoms is not recommended. For people at high risk For people with certain inherited genetic syndromes4 who are at increased risk of small intestine cancer, doctors might recommend regular tests to look for cancer early, especially in the duodenum (the first part of the small intestine). -

Surgicaltechniques
OBGM_0806_Hatch.final 7/21/06 11:06 AM Page 17 SURGICALTECHNIQUES THE RETROPERITONEAL SPACE Keeping vital structures out of harm’s way Knowledge of the retroperitoneal space is critical, to avoid unnecessary blood loss and injury of the ureter, bladder, bowel, and nerves he accomplished gynecologic sur- Kenneth D. Hatch, MD The “landmark” Professor, Department geon must know the anatomy of of Obstetrics and Gynecology, T the retroperitoneal space in order umbilical ligament Arizona Health Sciences Center Tucson, Ariz to avoid damage to normal structures, as® Dowden Health Media well as remove pathology. Many disease The umbilical ligament was the umbilical processes involve the pelvic peritoneum, artery in fetal life and courses along the uterosacral ligaments, rectosigmoidCopyrightFor or edgepersonal of the bladder use to theonly anterior abdom- ovarian pedicles, and require the surgeon inal wall up to the umbilicus. It is a useful to enter the retroperitoneal space to iden- guide into the perivesicle space. Lateral to it tify the ureters and blood vessels and are the iliac vessels, and medial is the blad- keep them out of harm’s way. The chal- der. It is also a good marker for finding the IN THIS ARTICLE lenges are complex: right spot to open the round ligament. • Badly distorted anatomy and the ante- ❙ Endometriosis may rior and posterior cul-de-sac necessi- imperil the ureter tate mobilization of the rectosigmoid Page 20 and bladder. • Intraligamentous fibroids require ❙ Preventing ureteral knowledge of the blood supply in the retroperitoneal space. Malignant disor- injury ders mandate that the lymph nodes be Page 23 dissected to determine extent of disease and as part of treatment. -
Digestive System
Digestive system Dr. Anna L. Kiss Department of Anatomy, Histology and Embryology Semmelweis University Budapest 2019 The gastrointestinal tract (GI tract): digestion and excretion Upper gastrointestinal tract The upper GI tract consists of the mouth, pharynx, esophagus, and stomach. The lower GI tract. small intestine, which has three parts: -duodenum -jejunum -ileum large intestine, which has three parts: -cecum (the vermiform appendix is attached to the cecum). -colon (ascending colon, transverse colon, descending colon and sigmoid flexure) -rectum Primitive Gut Tube Coeliac trunk Superior mesenteric artery Inferior mesenteric artery Vitelline duct Umbilical loop Umbilical artery Final Position of Parts of Gut Tube Abdominal esophagus Thoracic esophagus Liver Stomach Gall bladder & bile duct Duodenum Pancreas 2.) Transverse colon Jejunum & ileum 1.) Ascending colon 3.) Descending colon Cecum Appendix 4.) Sigmoid colon Final Position of Parts of Gut Tube Stomach: left hypochondric region (intraperitoneal) Duodenum: right side (partly retroperitoneal) Jejunum, ileum: umbilical + iliac region (intraperitoneal) Appendix: right side (Mc Burney point) (intraperitoneal) Ascending colon: right iliac region Transverse colon: middle position (intraperitoneal) Descending colon: left iliac region Sigmoid colon: sacral and pelvic region (intraperitoneal) highly acidic environment due to gastric acid production The stomach lies between the esophagus and the duodenum It is on the left side of the abdominal cavity. Stomach fundus cardia rugae!! lesser curvature body pylorus greater curvature Diaphragm Fundus pyloric antrum Corpus superior part body (duodenum) Greater curvature descending part (duodenum) ascending part Jejunum horizontal part Histology of the gut Mucosa: • epithelium: simple columnar (goblet cells) • propria (lymphoreticular connective tissue): glands (Lieberkhün crypts) • muscularis mucosae (2 layered smooth muscle) Submucosa: loose connective tissue (submucosus plexus; glands, lymphatic follicles) External muscle layer (t. -

Comparison of Survival and Prognostic Factors in Patients with Gastric Adenocarcinoma in T2 and T3 Original Article377
Jucá Comparison of survival and prognostic factors in patients with gastric adenocarcinoma in T2 and T3 Original Article377 Comparison of survival and prognostic factors in patients with gastric adenocarcinoma in T2 and T3 Comparação da sobrevivência e dos fatores prognósticos em pacientes com adenocarcinoma gástrico T2 e T3 PATRÍCIA CAMPOS JUCÁ – ACBC-RJ1; LAERCIO LOURENÇO – TCBC-SP2; RUBENS KESLEY – TCBC-RJ1; EDUARDO LINHARES RIELLO DE MELLO – TCBC-RJ1; IVANIR MARTINS DE OLIVEIRA 3; JOSÉ HUMBERTO SIMÕES CORREA – TCBC-RJ1 ABSTRACT Objective: To compare the survival and prognosis after surgical treatment of patients with gastric adenocarcinoma which extends to the muscular layer (T2), and patients whose tumor invades the subserosa (T3). Methods: This was a retrospective study of 122 patients with gastric cancer invading the muscularis propria and subserosa, undergoing surgical treatment from January 1997 to December 2008 and followed-up until December 2010. We analyzed demographic, surgical and pathological variables. Results: Of the 122 patients, 22 (18%) were excluded from the final analysis because they showed: positive margin or less than 15 lymph nodes in the surgical specimen, early postoperative mortality and second primary tumors. Among the 100 patients included, 75 had tumors inveding the muscularis propria (T2) and 25 with extension to the subserosa (T3). Overall survival was 83.8%, and 90.6% for T2 and 52.1% or T3. Univariate analysis showed statistical significance in: lymph node metastasis (p = 0.02), tumor size (p = 0.000), tumor pathological stage (p = 0.000), lymph node pathologic stage (p = 0.000) and staging by classification of groups TNM-UICC/AJCC, 2010 (p = 0.000). -

SPLANCHNOLOGY Part I. Digestive System (Пищеварительная Система)
КАЗАНСКИЙ ФЕДЕРАЛЬНЫЙ УНИВЕРСИТЕТ ИНСТИТУТ ФУНДАМЕНТАЛЬНОЙ МЕДИЦИНЫ И БИОЛОГИИ Кафедра морфологии и общей патологии А.А. Гумерова, С.Р. Абдулхаков, А.П. Киясов, Д.И. Андреева SPLANCHNOLOGY Part I. Digestive system (Пищеварительная система) Учебно-методическое пособие на английском языке Казань – 2015 УДК 611.71 ББК 28.706 Принято на заседании кафедры морфологии и общей патологии Протокол № 9 от 18 апреля 2015 года Рецензенты: кандидат медицинских наук, доцент каф. топографической анатомии и оперативной хирургии КГМУ С.А. Обыдённов; кандидат медицинских наук, доцент каф. топографической анатомии и оперативной хирургии КГМУ Ф.Г. Биккинеев Гумерова А.А., Абдулхаков С.Р., Киясов А.П., Андреева Д.И. SPLANCHNOLOGY. Part I. Digestive system / А.А. Гумерова, С.Р. Абдулхаков, А.П. Киясов, Д.И. Андреева. – Казань: Казан. ун-т, 2015. – 53 с. Учебно-методическое пособие адресовано студентам первого курса медицинских специальностей, проходящим обучение на английском языке, для самостоятельного изучения нормальной анатомии человека. Пособие посвящено Спланхнологии (науке о внутренних органах). В данной первой части пособия рассматривается анатомическое строение и функции системы в целом и отдельных органов, таких как полость рта, пищевод, желудок, тонкий и толстый кишечник, железы пищеварительной системы, а также расположение органов в брюшной полости и их взаимоотношения с брюшиной. Учебно-методическое пособие содержит в себе необходимые термины и объём информации, достаточный для сдачи модуля по данному разделу. © Гумерова А.А., Абдулхаков С.Р., Киясов А.П., Андреева Д.И., 2015 © Казанский университет, 2015 2 THE ALIMENTARY SYSTEM (systema alimentarium/digestorium) The alimentary system is a complex of organs with the function of mechanical and chemical treatment of food, absorption of the treated nutrients, and excretion of undigested remnants.