A Fatty Substance) from a Diseased Artery
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Coding for Angioplasty & Stent Procedures
Coding for Angioplasty & Stent Procedures July 2020 Jennifer Bash, RHIA, CIRCC, RCCIR, CPC, RCC Director of Coding Education Agenda • Introduction • Definitions • General Coding Guidelines • Presenting Problems/Medical Necessity for Angioplasty & Stent • General Angioplasty & Stent Procedures • Cervicocerebral Procedures • Lower Extremity Procedures Disclaimer The information presented is based on the experience and interpretation of the presenters. Though all of the information has been carefully researched and checked for accuracy and completeness, ADVOCATE does not accept any responsibility or liability with regard to errors, omissions, misuse or misinterpretation. CPT codes are trademark and copyright of the American Medical Association. Resources •AMA •CMS • ACR/SIR • ZHealth Publishing Angioplasty & Stent Procedures Angioplasty Angioplasty, also known as balloon angioplasty and percutaneous transluminal angioplasty, is a minimally invasive endovascular procedure used to widen narrowed or obstructed arteries or veins, typically to treat arterial atherosclerosis. Vascular Stent A stent is a tiny tube placed into the artery or vein used to treat vessel narrowing or blockage. Most stents are made of a metal or plastic mesh-like material. General Angioplasty & Stent Coding Guidelines • Angioplasty is not separately billable when done with a stent • Pre-Dilatation • PTA converted to Stent • Prophylaxis • EXCEPTION-Complication extending to a different vessel • Coded per vessel • Codes include RS&I • Territories • Hierarchy General Angioplasty -

Coronary Angiogram, Angioplasty and Stent Placement
Page 1 of 6 Coronary Angiogram, Angioplasty and Stent Placement A Patient’s Guide Page 2 of 6 What is coronary artery disease? What is angioplasty and a stent? Coronary artery disease means that you have a If your doctor finds a blocked artery during your narrowed or blocked artery. It is caused by the angiogram, you may need an angioplasty (AN-jee- buildup of plaque (fatty material) inside the artery o-plas-tee). This is a procedure that uses a small over many years. This buildup can stop blood from inflated balloon to open a blocked artery. It can be getting to the heart, causing a heart attack (the death done during your angiogram test. of heart muscle cells). The heart can then lose some of its ability to pump blood through the body. Your doctor may also place a stent at this time. A stent is a small mesh tube that is placed into an Coronary artery disease is the most common type of artery to help keep it open. Some stents are coated heart disease. It is also the leading cause of death for with medicine, some are not. Your doctor will both men and women in the United States. For this choose the stent that is right for you. reason, it is important to treat a blocked artery. Angioplasty and stent Anatomy of the Heart 1. Stent with 2. Balloon inflated 3. Balloon balloon inserted to expand stent. removed from into narrowed or expanded stent. What is a coronary angiogram? blocked artery. A coronary angiogram (AN-jee-o-gram) is a test that uses contrast dye and X-rays to look at the blood vessels of the heart. -
Vela Proximal Endograft System Phoenix Atherectomy System
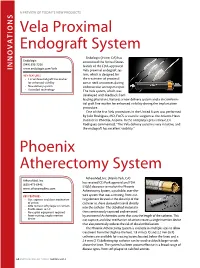
A PREVIEW OF today’s NEW PRODUCTS ONS I Vela Proximal Endograft System Endologix (Irvine, CA) has Endologix announced the United States (949) 595-7200 launch of the FDA-approved INNOVAT www.endologix.com/Vela Vela proximal endograft sys- KEY FEATURES tem, which is designed for • Circumferential graft line marker the treatment of proximal for enhanced visibility aortic neck anatomies during • New delivery system endovascular aneurysm repair. • ActiveSeal technology The Vela system, which was developed with feedback from leading physicians, features a new delivery system and a circumferen- tial graft line marker for enhanced visibility during the implantation procedure. One of the first Vela procedures in the United States was performed by Julio Rodriguez, MD, FACS, a vascular surgeon at the Arizona Heart Institute in Phoenix, Arizona. In the company’s press release, Dr. Rodriguez commented, “The Vela delivery system is very intuitive, and the endograft has excellent visibility.” Phoenix Atherectomy System AtheroMed, Inc. (Menlo Park, CA) AtheroMed, Inc. has received CE Mark approval and FDA (650) 473-6846 510(k) clearance to market the Phoenix www.atheromedinc.com Atherectomy System, a pushable, over-the- KEY FEATURES wire system that uses a rotating, front-cut- • Cut, capture, and clear mechanism ting element located at the distal tip of the of action catheter to shave diseased material directly • Able to treat soft plaque or calcium • Profile down to 5 F into the catheter. The debulked material is • No capital equipment required then continuously captured and removed • Front-cutting, single insertion by an internal Archimedes screw that runs the length of the catheter. -

Inpatient Coronary Angiography and Angioplasty (PCI)
If English is not your first language and you need help, please contact the Interpretation and Translation Service Jeśli angielski nie jest twoim pierwszym językiem i potrzebujesz pomocy, skontaktuj się z działem tłumaczeń ustnych i pisemnych ا رﮔ ا یزﯾرﮕﻧ پآ ﯽﮐ ﮩﭘ ﯽﻠ ﺑز نﺎ ںﯾﮩﻧ ﮯﮨ روا پآ وﮐ ددﻣ ﯽﮐ ترورﺿ ﮯﮨ وﺗ ، هارﺑ مرﮐ ﯽﻧﺎﻣﺟرﺗ روا ہﻣﺟرﺗ تﻣدﺧ تﻣدﺧ ہﻣﺟرﺗ روا ﯽﻧﺎﻣﺟرﺗ مرﮐ هارﺑ ، وﺗ ﮯﮨ ترورﺿ ﯽﮐ ددﻣ وﮐ پآ روا ﮯﮨ ںﯾﮩﻧ ﮯﺳ ر ا ﺑ ط ہ ﮐ ر ﯾ ںﯾرﮐ ﮯ Dacă engleza nu este prima ta limbă și ai nevoie de ajutor, te rugăm să contactezi Serviciul de interpretare și traducere Inpatient Coronary ইংরাজী যিদ আপনার .থম ভাষা না হয় এবং আপনার সাহােয9র .েয়াজন হয় তেব অনু=হ কের ?দাভাষী এবং অনুবাদ পিরেষবা@েত ?যাগােযাগ কBন Angiography and (Angioplasty (PCI إ ذ ا مﻟ نﻛﺗ ﻠﺟﻧﻹا ﺔﯾزﯾ ﻲھ كﺗﻐﻟ ﻰﻟوﻷا ﺗﺣﺗو جﺎ إ ﻰﻟ ةدﻋﺎﺳﻣ ، ﻰﺟرﯾﻓ لﺎﺻﺗﻻا ﺔﻣدﺧﺑ ا ﻟ ﺔﻣﺟرﺗ ا ﺔﯾوﻔﺷﻟ او ﻟ ﺔﯾرﯾرﺣﺗ وﺔوﺷ ﻣر ﻣﺧ ﺎﺗاﻰرﻓ،ةﻋﺳ ﻟإج ﺣوﻰواكﻐ ھﺔز ﺟﻹ ﻛ ﻟ : 0161 627 8770 An information guide : [email protected] To improve our care environment for Patients, Visitors and Staff, Northern Care Alliance NHS Group is Smoke Free including buildings, grounds & car parks. For advice on stopping smoking contact the Specialist Stop Smoking Service on 01706 517 522 For general enquiries please contact the Patient Advice and Liaison Service (PALS) on 0161 604 5897 For enquiries regarding clinic appointments, clinical care and treatment please contact 0161 624 0420 and the Switchboard Operator will put you through to the correct department / service The Northern Care Alliance NHS Group (NCA) is one of the largest NHS organisations The Northern Care Alliance NHS Group (NCA) is one of the largest NHS organisationsin the country, employingin the country 17,000 bringing staff and together providing two a NHS range Trusts, of hospital Salford and Royalcommunity NHS Foundationhealthcare services Trust and to around The Pennine 1 million Acute people Hospitals across Salford, NHS Trust. -

Preparing for Your Peripheral Artery Angioplasty and Stenting
Preparing for your Peripheral Artery Angioplasty and Stenting Michigan Medicine Frankel Cardiovascular Center Michigan Medicine Phone Numbers Billing ………………………………………………………………………… 855-855-0863 734-615-0863 Call Center ……………………………………………………………………888-287-1082 Vascular Surgery (use Call Center) ………………………………………888-287-1082 Cardiovascular Operating Room Desk …………………………………734-232-4553 Office of Clinical Safety (comments) ……………………………………877-285-7788 Emergency Department ……………………………………………………734-936-6666 Guest Assistance Program (GAP) (accommodations) …………………800-888-9825 Hospital Operator ……………………………………………………………734-936-4000 Lost & Found …………………………………………………………………734-936-7890 Mardigian Wellness Resource Center ……………………………………734-232-4120 Parking & Transportation …………………………………………………734-764-7474 Registration & Insurance4 Verification …………………………………866-452-9896 Med-Inn (hotel) ……………………………………………………………800-544-8684 734-936-0100 Tobacco Consultation Services ……………………………………………734-938-6222 Units (Patient Care): CVC-4 ICU ……………………………………………………………734-936-6514 CVC-5 Cardiac Surgery ……………………………………………734-232-4772 CVC-2A Cardiac Procedure Unit………………………………… 734-232-4200 Other: Michigan Quit Line (Smoking) ……………………………………………800-784-8669 Address (mail): Frankel CVC (room number/unit if known) or UH (room number/unit if known) Person’s Name University of Michigan Health System 1500 E. Medical Center Drive Ann Arbor, MI 48109 Building Location (visiting): Samuel and Jean Frankel Cardiovascular Center East Ann Street & Observatory Street Ann Arbor, MI 481 Table of Contents: -

Diagnosing and Treating Vascular Disease
THE CENTER FOR VASCULAR CARE AT WASHINGTON HOSPITAL CENTER Diagnosing and Treating Vascular Disease If you have symptoms of vascular disease or Peripheral Artery Disease (PAD), the best thing to do is see your physician for examination and possible testing. And, if you have the following risk factors, see your doctor to determine if you should be tested. The Center for Vascular Care at Washington Hospital Center can provide painless, risk free tests and the most complete array of treatment options for vascular disease in the region. RISK FACTORS TESTING FOR VASCULAR DISEASE FOR VASCULAR DISEASE Ankle-brachial Index: Patients with leg I Cigarette smoking artery blockage are at increased risk of I Older than age 50* heart attack and stroke. This test (ABI) is I Obesity a simple, safe, painless test for blockages. A blood pressure cuff is placed above I Diabetes the ankles and pressures are measured I Heart disease compared to arm pressures to determine I High Cholesterol the risk of cardiovascular events. It takes I High-stress lifestyle 5–10 minutes. I High blood pressure Carotid Duplex Scan: Blockage in a major I Family history of aneurysms artery increases the likelihood of a stroke. *Over age 65 if no other risk factors exist Thickening of the walls of the carotid arteries can lead to heart attack. An arterial SYMPTOMS OF VASCULAR DISEASE duplex scan is a safe, painless, highly I Leg pain that goes away with rest accu rate method of determining blockage. A sound wave device, placed lightly on the I Numbness of the legs or feet at rest skin, can tell if there is a problem. -

Endovascular Stent Grafts: Atreatment for Abdominal Aortic Aneurysms TABLE of CONTENTS
PATIENT INFORMATION BOOKLET Endovascular Stent Grafts: ATreatment for Abdominal Aortic Aneurysms TABLE OF CONTENTS Introduction 1 Glossary 2 Abdominal Aorta 4 Abdominal Aortic Aneurysm 5 Causes 6 Symptoms 6 Treatment Options 6 Open Surgery 7 Endovascular Stent Grafting 8 Abdominal Stent Graft 9 Risks 10 Benefits 11 Abdominal Stent Graft Procedure 12 What Symptoms Should Prompt You to Call Your Doctor After the Procedure? 14 Follow-Up 14 Implanted Device Identification Card 14 Magnetic Resonance Imaging 15 Lifestyle Changes 15 Questions You May Want to Discuss with Your Doctor 15 Additional Information 17 INTRODUCTION You have discussed having a stent graft procedure to treat an abdominal aortic aneurysm (AAA) with your doctor. Your doctor has given you this guide to help you further understand the device and procedure. Only a doctor can determine if you are a good candidate for an abdominal stent graft procedure. A Glossary is provided in the next section to help you understand the medical terms used in this book. Words that are bolded in the text are defined in the Glossary. S GLOSSARY Abdominal aortic aneurysm (AAA): A bulging or"ballooning"of a weakened area of the abdominal aorta. This term is often called "AAA.' Anatomy: The study of parts of the body. Aneurysm rupture/Rupture: A tear in the blood vessel wall near or at the location of the weakened area of the blood vessel. Aorta: The main artery that carries blood from the heart to the rest of the body. CT scan: A scan that creates a series of X-rays that form a picture of the aneurysm and nearby blood vessels. -

Carotid Endarterectomy Compared with Angioplasty and Stenting: the Status of the Debate
Neurosurg Focus 5 (6):Article 2, 1998 Carotid endarterectomy compared with angioplasty and stenting: the status of the debate Felipe C. Albuquerque, M.D., George P. Teitelbaum, M.D., Donald W. Larsen, M.D., and Steven L. Giannotta, M.D. Department of Neurological Surgery, Los Angeles County and University of Southern California Medical Center, Los Angeles, California Endarterectomy is the treatment of choice for patients with symptomatic stenosis of the internal carotid artery. Recently, debate has arisen over the potential benefits of endovascular techniques. Although retrospective analyses of angioplasty and stenting procedures suggest comparable clinical efficacy to endarterectomy, prospective evaluation is pending. The authors review the status of the debate and discuss those issues on both sides that are particularly contentious and clinically relevant. Key Words * carotid endarterectomy * angioplasty * stenting Atherosclerotic disease of the common carotid artery bifurcation is associated with 20 to 30% of cerebrovascular accidents.[13,15,27] Stroke is the third leading cause of death in the United States and the most common and disabling neurological disorder among the elderly worldwide.[13,15,27] In light of these public health concerns, research in the last half of this century has been focused on the optimum treatment of carotid artery stenosis. Prospective analyses such as those performed by the North American Symptomatic Carotid Endarterectomy Trial (NASCET), the Asymptomatic Carotid Atherosclerosis Study (ACAS), and the European Carotid Surgery Trial have demonstrated superior reduction in stroke incidence among symptomatic and a select group of asymptomatic patients who undergo carotid endarterectomy (CEA).[17,18,36] In fact, these studies have established CEA as the "gold standard" for the treatment of carotid artery atherosclerosis. -

After Your Peripheral Vascular Angioplasty”, with Permission from the University Health Network Patient and Caregiver Education Program
After your Peripheral Vascular Surgical Program Angioplasty For Patients Going Home After Surgery You have had a peripheral vascular angioplasty. This is a surgery to open arteries (blood vessels) in your legs that are blocked with plaque (see Figure 1). During this surgery, we insert a catheter (thin tube) with a balloon at the tip, usually through the groin, into the blocked artery. At the blockage, we inflate the balloon, pushing the plaque out against the artery wall. This widens the artery and restores the flow of blood. The surgery can help reduce the symptoms of poor blood flow, such as pain, numbness, and wounds that will not heal. The surgery may also prevent the need to amputate the leg or foot. Figure 1. The illustration shows how peripheral artery disease can affect arteries in the legs. “A” shows a normal artery with normal blood flow. “B” shows an artery with plaque buildup that’s partially blocking blood flow. By National Heart Lung and Blood Insitute (NIH) (National Heart Lung and Blood Insitute (NIH)) [Public domain]. Read this information to learn: • What activities you can do when you get home • How to care for your puncture site • What problems to look out for • When you will have a follow-up. Form # 005023 © 2017_09 (REVIEWED 2020_11) www.hrh.ca What symptoms might I have after surgery? SYMPTOM WHAT TO DO GROIN PUNCTURE SITE: You • These are normal and should resolve within 2 to 3 weeks. may notice a small lump (the size of a large marble) and/or some bruising. PAIN: You may have groin • We may give you a prescription for pain medicine at the time of discomfort. -

Lower Extremity Invasive Diagnostic and Endovascular Procedures
UnitedHealthcare® Commercial Medical Policy Lower Extremity Invasive Diagnostic and Endovascular Procedures Policy Number: 2021T0602F Effective Date: July 1, 2021 Instructions for Use Table of Contents Page Related Commercial Policies Coverage Rationale ........................................................................... 1 • Pneumatic Compression Devices Documentation Requirements......................................................... 2 • Surgical and Ablative Procedures for Venous Definitions ........................................................................................... 3 Insufficiency and Varicose Veins Applicable Codes .............................................................................. 4 Description of Services ..................................................................... 5 Community Plan Policy Clinical Evidence ............................................................................... 5 • Lower Extremity Invasive Diagnostic and U.S. Food and Drug Administration ................................................ 7 Endovascular Procedures References ......................................................................................... 8 Medicare Advantage Coverage Summary Policy History/Revision Information................................................ 9 • Instructions for Use ........................................................................... 9 Cardiovascular Diagnostic Procedures Coverage Rationale Note: This policy does not apply to upper extremities. Diagnosis Lower extremity -

Angioplasty and Stent Education Guide
Angioplasty and Stent Education Guide Table of Contents Treating coronary artery disease . 2 What is coronary artery disease . 3 Coronary artery disease treatment options . 4 What are coronary artery stents . 6 What are the different types of coronary stents . 7 How does the drug coating and polymer work on the SYNERGYTM bioabsorbable polymer drug-eluting stent? . 8 Risks of treatment options . 9 Before your coronary artery stenting procedure . 12 During a typical coronary artery stenting procedure . 13 After a typical coronary artery stenting procedure . 14 Medications . 15 Frequently asked questions . 16 Glossary . 17 1 Treating coronary artery disease Your doctor may want you to have a stent placed in your coronary artery . This is to help treat your coronary artery disease . This guide explains the procedure and what you can expect from start to finish . A glossary at the end of this guide defines common medical terms related to this procedure . You will also learn steps you can take to live a healthier life with coronary artery disease . 2 What is coronary artery disease? Coronary Artery Disease (CAD) is the narrowing of the arteries in the heart . This narrowing can also be called stenosis . It is usually Aorta Left caused by a build up of fat or calcium deposits called plaque . Over Coronary Right Artery time, this plaque can build to a total blockage of the artery . This Coronary process is called atherosclerosis . Artery Circumflex Artery When the heart doesn’t receive enough blood flow due to blockage in the artery, it may cause mild to severe chest pain or pressure . -

Endovascular Versus Open Revascularization for Peripheral Arterial Disease
COVER STORY Endovascular Versus Open Revascularization for Peripheral Arterial Disease A review of 12-year data revealing changes in amputation and limb salvage rates associated with a shift in revascularization modalities. BY NILESH N. BALAR, MD; RANJITH DODLA, MD; PARIND OZA, MD; PARTH N. PATEL; AND MAYANK PATEL, MD eripheral arterial disease (PAD) affects approxi- mately 12% to 14% of the general population, which steadily increases with age and affects up P to 20% of patients who are older than 75 years.1 The prevalence of PAD markedly increases in patients with diabetes, hypertension, hyperlipidemia, and a history of smoking.2 The most sensitive tool to detect PAD is the ankle-brachial index.2 Various treatment options include lifestyle modifications, endovascular revascularization, and open revascularization. In the past, most of these patients with significant limb ischemia have been treated Figure 1. Trends in endovascular revascularization, surgical with surgical revascularization. However, with rapid revascularization, and amputation over 12 years. advances in catheter-based technology, there has been a significant shift toward endovascular interventions.3,4 lower extremity amputations. All amputations were per- There are very few data regarding limb salvage rates formed by vascular surgeons only. Surgical revasculariza- and lower extremity amputation rates after infrainguinal tion procedures were femoropopliteal artery bypass, endovascular procedures.5 To examine the impact of femorofemoral crossover bypass, femorotibial vessel endovascular interventions on the amputation and limb bypass, and other distal vessel bypasses. Both native and salvage rates and determine its relationship to open prosthetic conduits were included in the study. Because revascularization, we set forth to retrospectively examine few axillary femoral and aortobifemoral bypass proce- a 12-year period of data from this patient population at dures were performed in any given year, these procedures our center.