Final Report Nigeria: Yellow Fever
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

YELLOW FEVER SITUATION REPORT Report of Yellow Fever Cases in 14 States Serial Number 010: Epi-Week 4 (As at 29 January 2021)
YELLOW FEVER SITUATION REPORT Report of Yellow fever Cases in 14 States Serial Number 010: Epi-Week 4 (as at 29 January 2021) HIGHLIGHTS ▪ The Nigeria Centre for Disease Control (NCDC) is currently responding to reports of yellow fever cases in 14 states - Akwa Ibom, Bauchi, Benue, Borno, Delta, Ebonyi, Enugu, Gombe, Imo, Kogi, Osun, Oyo, Plateau and Taraba States From the 14 States ▪ In the last week (weeks 4, 2021) ‒ Four new confirmed cases were reported from National Reference Laboratory (NRL) from 2 Local Government Areas (LGAs) in Benue - [Okpokwu (3), Ado (1) ‒ Thirteen presumptive positive cases were reported from NRL [Benue (6)] and Central Public Health Laboratory (CPHL) from [Enugu (6), Oyo (1)] ‒ One new LGA reported a confirmed case from Ado (1) in Benue State, ‒ No new death was recorded among confirmed cases ▪ Cumulatively from epi-week 24, 2020 – epi-week 4, 2021 ‒ A total of 1,502 suspected cases with 179 presumptive positive cases have been reported from 34 LGAs across 14 States from the Nigeria Laboratories ‒ Out of the 1,502 suspected, 161 confirmed cases [Delta-63 Ika North-East (48), Aniocha-South(6), Ika South (4), Oshimili South (2), Oshimili North(1), Ukwuani(1), Ndokwa West (1)], [Enugu-53 Enugu East (4), Enugu North (1), Igbo-Etiti (6), Igbo-Eze North(13), Isi-Uzo (15), Nkanu West (3) Nsukka(8), Udenu (3)], [Benue-17 (Ogbadibo (12), Okpokwu (4), Ado (1)], [Bauchi-9 Ganjuwa (8), Darazo (1)], [Borno-6 Gwoza(1), Hawul (1), Jere (2), Shani (1), Maiduguri (1)], [Ebonyi-3 Ohaukwu (3)], [Oyo-3), Ibarapa North East (1), Ibarapa North (2)], [Gombe-1 Akko (1)], [Imo-1 Owerri North(1)], [Kogi-1 Lokoja (1)], [Plateau- 1 Langtang North (1)], [Taraba-1 Jalingo (1)], [Akwa Ibom-1 Uyo(1)] and [Osun-1 Ilesha East (1)]. -

Nigeria's Constitution of 1999
PDF generated: 26 Aug 2021, 16:42 constituteproject.org Nigeria's Constitution of 1999 This complete constitution has been generated from excerpts of texts from the repository of the Comparative Constitutions Project, and distributed on constituteproject.org. constituteproject.org PDF generated: 26 Aug 2021, 16:42 Table of contents Preamble . 5 Chapter I: General Provisions . 5 Part I: Federal Republic of Nigeria . 5 Part II: Powers of the Federal Republic of Nigeria . 6 Chapter II: Fundamental Objectives and Directive Principles of State Policy . 13 Chapter III: Citizenship . 17 Chapter IV: Fundamental Rights . 20 Chapter V: The Legislature . 28 Part I: National Assembly . 28 A. Composition and Staff of National Assembly . 28 B. Procedure for Summoning and Dissolution of National Assembly . 29 C. Qualifications for Membership of National Assembly and Right of Attendance . 32 D. Elections to National Assembly . 35 E. Powers and Control over Public Funds . 36 Part II: House of Assembly of a State . 40 A. Composition and Staff of House of Assembly . 40 B. Procedure for Summoning and Dissolution of House of Assembly . 41 C. Qualification for Membership of House of Assembly and Right of Attendance . 43 D. Elections to a House of Assembly . 45 E. Powers and Control over Public Funds . 47 Chapter VI: The Executive . 50 Part I: Federal Executive . 50 A. The President of the Federation . 50 B. Establishment of Certain Federal Executive Bodies . 58 C. Public Revenue . 61 D. The Public Service of the Federation . 63 Part II: State Executive . 65 A. Governor of a State . 65 B. Establishment of Certain State Executive Bodies . -

Assessment of Youths Involvement in Self-Help Community Development Projects in Nsukka Local Government Area of Enugu State By
i ASSESSMENT OF YOUTHS INVOLVEMENT IN SELF-HELP COMMUNITY DEVELOPMENT PROJECTS IN NSUKKA LOCAL GOVERNMENT AREA OF ENUGU STATE BY EZEMA MARCILLINUS CHIJIOKE PG/M.ED/11/58977 DEPARTMENT OF ADULT EDUCATION AND EXTRA-MURAL STUDIES, UNIVERSITY OF NIGERIA, NSUKKA AUGUST, 2014. 2 ASSESSMENT OF YOUTHS INVOLVEMENT IN SELF-HELP COMMUNITY DEVELOPMENT PROJECTS IN NSUKKA LOCAL GOVERNMENT AREA OF ENUGU STATE BY EZEMA MARCILLINUS CHIJIOKE PG/M.ED/11/58977 DEPARTMENT OF ADULT EDUCATION AND EXTRA-MURAL STUDIES, UNIVERSITY OF NIGERIA, NSUKKA ASSOC. PROF (MRS.) F.O. MBAGWU (SUPERVISOR) AUGUST, 2014. 3 TITLE PAGE Assessment of Youths Involvement in Self-Help Community Development Projects in Nsukka Local Government Area of Enugu State 4 APPROVAL PAGE This project has been approved for the Department of Adult Education and Extra-Mural Studies University of Nigeria, Nsukka. By _________________ _________________ Assoc. Prof (Mrs) F.O. Mbagwu Prof. P.N.C. Ngwu Supervisor Head of Department _______________ ________________ Internal Examiner External Examiner ________________________ Prof. IK. Ifelunni Dean Faculty of Education 5 CERTIFICATION Ezema M.C is a postgraduate student in the Department of Adult Education and Extra-Mural Studies with Registration Number PG/M.Ed/11/58977 and has satisfactorily completed the requirements for the course and research work for the degree of Masters in Adult Education and Community Development. The work embodied in this project is original and has not been submitted in part or full for any other diploma or degree of this university or any other university. ___________________ ___________________ Ezema, Marcillinus Chijioke Assoc. Prof (Mrs) F.O. Mbagwu Student Supervisor 6 DEDICATION This research work is dedicated to God Almighty for his mercy and protection to me throughout the period of writing this project. -
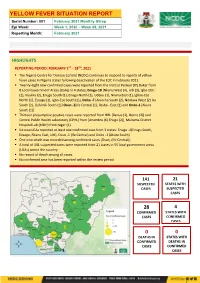
YELLOW FEVER SITUATION REPORT Serial Number: 001 February 2021 Monthly Sitrep Epi Week: Week 1, 2020 – Week 08, 2021 Reporting Month: February 2021
YELLOW FEVER SITUATION REPORT Serial Number: 001 February 2021 Monthly Sitrep Epi Week: Week 1, 2020 – Week 08, 2021 Reporting Month: February 2021 HIGHLIGHTS REPORTING PERIOD: FEBRUARY 1ST – 28TH, 2021 ▪ The Nigeria Centre for Disease Control (NCDC) continues to respond to reports of yellow fever cases in Nigeria states following deactivation of the EOC in February 2021. ▪ Twenty -eight new confirmed cases were reported from the Institut Pasteur (IP) Dakar from 8 Local Government Areas (LGAs) in 4 states; Enugu-18 [Nkanu West (4), Udi (3), Igbo-Etiti (2), Nsukka (2), Enugu South (1), Enugu North (1), Udenu (1), Nkanu East (1), Igboe-Eze North (1), Ezeagu (1), Igbo-Eze South (1)], Delta -7 [Aniocha South (2), Ndokwa West (2) Ika South (2), Oshimili South (1)] Osun -2[Ife Central (1), Ilesha - East (1) and Ondo-1 [Akure South (1)] ▪ Thirteen presumptive positive cases were reported from NRL [Benue (2), Borno (2)] and Central Public Health Laboratory (CPHL) from [Anambra (6) Enugu (2)], Maitama District Hospital Lab (MDH) from Niger (1) ▪ Six new LGAs reported at least one confirmed case from 3 states: Enugu -4(Enugu South, Ezeagu, Nkanu East, Udi), Osun -1 (Ife Central) and Ondo -1 (Akure South) ▪ One new death was recorded among confirmed cases [Osun, (Ife Central)] ▪ A total of 141 suspected cases were reported from 21 states in 55 local government areas (LGAs) across the country ▪ No record of death among all cases. ▪ No confirmed case has been reported within the review period 141 21 SUSPECTED STATES WITH CASES SUSPECTED CASES 28 4 -

Break the Silence News!
Break the Silence News! A Monthly Bulleting of Tamar Sexual Assault Referral Centre (SARC) Volume 9 January 2016 - February 2016 Edition participants to help carry out health awareness DFID trains campaign among stakeholders in the various 46 doctors, nurses, counselors and communities in Nigeria through the churches, social workers on rape in Enugu mosques and schools. Also speaking at the event in Enugu, one of the Justice For All (J4A) Programme of the Department trainers/facilitators from Manchester who for International Development (DFID), have begun incidentally is the Centre Manager of St. Mary's the training of 46 medical practitioners and social Sexual Assault Referral Centre, Manchester City, workers on how to handle rape victims. Mrs. Bernie Ryan, said that the essence of the st th The five days training which started from 1 -5 training was to impart practical knowledge and wide February 2016, was organized in Enugu for different scale experience to participants in relation to states across the federation. The objective was on the providing services to victims of sexual violence in need to set up a Sexual Assault Referral Centre and terms of physical, emotional and medical support. train participants on how to manage it as well as She extolled the participants and urged them to respond to the victims properly. The participants change their mindset and attitudes toward sexual drawn from Zamfara, Yobe, Kaduna, Enugu, Ekiti, assault victims so that more people could be helped. Cross River and Akwa Ibom states, were being A medical consultant and participant, Dr Nene trained on technical skills, forensic examination and Andem, said that the training had exposed her a lot to counseling. -

Federal Government of Nigeria 2011 Budget Federal Ministry of Land and Housing
FEDERAL GOVERNMENT OF NIGERIA 2011 BUDGET SUMMARY FEDERAL MINISTRY OF LAND AND HOUSING TOTAL PERSONNEL TOTAL OVERHEAD TOTAL TOTAL CODE MDA COST COST RECURRENT TOTAL CAPITAL ALLOCATION =N= =N= =N= =N= =N= MINISTRY OF LANDS & 0250001 HOUSING 3,137,268,528 418,458,068 3,555,726,596 33,147,994,158 36,703,720,754 TOTAL 3,137,268,528 418,458,068 3,555,726,596 33,147,994,158 36,703,720,754 27,227,159,376 15,086,283,689 NATIONAL ASSEMBLY LAND AND HOUSING: 1 2011 AMENDMENT APPROPRIATION FEDERAL GOVERNMENT OF NIGERIA 2011 AMENDMENT APPROPRIATION CODE LINE ITEM (=N=) TOTAL: MINISTRY OF LANDS & HOUSING 36,703,720,754 TOTAL ALLOCATION: 36,703,720,754 21 PERSONNEL COST 3,137,268,528 2101 SALARY 2,789,977,780 210101 SALARIES AND WAGES 2,789,977,780 21010101 CONSOLIDATED SALARY 2,789,977,780 2102 ALLOWANCES AND SOCIAL CONTRIBUTION 347,290,748 210202 SOCIAL CONTRIBUTIONS 347,290,748 21020201 NHIS 138,916,299 21020202 CONTRIBUTORY PENSION 208,374,449 22 TOTAL GOODS AND NON - PERSONAL SERVICES - GENERAL 418,458,068 2202 OVERHEAD COST 418,458,068 220201 TRAVEL& TRANSPORT - GENERAL 138,312,778 22020101 LOCAL TRAVEL & TRANSPORT: TRAINING 29,251,947 22020102 LOCAL TRAVEL & TRANSPORT: OTHERS 58,059,000 22020103 INTERNATIONAL TRAVEL & TRANSPORT: TRAINING 24,496,875 22020104 INTERNATIONAL TRAVEL & TRANSPORT: OTHERS 26,504,956 220202 UTILITIES - GENERAL 13,136,994 22020201 ELECTRICITY CHARGES 6,237,000 22020202 TELEPHONE CHARGES 3,534,300 22020203 INTERNET ACCESS CHARGES 900,000 22020205 WATER RATES 1,945,944 22020206 SEWERAGE CHARGES 519,750 220203 MATERIALS & -

Agulu Road, Adazi Ani, Anambra State. ANAMBRA 2 AB Microfinance Bank Limited National No
LICENSED MICROFINANCE BANKS (MFBs) IN NIGERIA AS AT FEBRUARY 13, 2019 S/N Name Category Address State Description 1 AACB Microfinance Bank Limited State Nnewi/ Agulu Road, Adazi Ani, Anambra State. ANAMBRA 2 AB Microfinance Bank Limited National No. 9 Oba Akran Avenue, Ikeja Lagos State. LAGOS 3 ABC Microfinance Bank Limited Unit Mission Road, Okada, Edo State EDO 4 Abestone Microfinance Bank Ltd Unit Commerce House, Beside Government House, Oke Igbein, Abeokuta, Ogun State OGUN 5 Abia State University Microfinance Bank Limited Unit Uturu, Isuikwuato LGA, Abia State ABIA 6 Abigi Microfinance Bank Limited Unit 28, Moborode Odofin Street, Ijebu Waterside, Ogun State OGUN 7 Above Only Microfinance Bank Ltd Unit Benson Idahosa University Campus, Ugbor GRA, Benin EDO Abubakar Tafawa Balewa University Microfinance Bank 8 Limited Unit Abubakar Tafawa Balewa University (ATBU), Yelwa Road, Bauchi BAUCHI 9 Abucoop Microfinance Bank Limited State Plot 251, Millenium Builder's Plaza, Hebert Macaulay Way, Central Business District, Garki, Abuja ABUJA 10 Accion Microfinance Bank Limited National 4th Floor, Elizade Plaza, 322A, Ikorodu Road, Beside LASU Mini Campus, Anthony, Lagos LAGOS 11 ACE Microfinance Bank Limited Unit 3, Daniel Aliyu Street, Kwali, Abuja ABUJA 12 Achina Microfinance Bank Limited Unit Achina Aguata LGA, Anambra State ANAMBRA 13 Active Point Microfinance Bank Limited State 18A Nkemba Street, Uyo, Akwa Ibom State AKWA IBOM 14 Ada Microfinance Bank Limited Unit Agwada Town, Kokona Local Govt. Area, Nasarawa State NASSARAWA 15 Adazi-Enu Microfinance Bank Limited Unit Nkwor Market Square, Adazi- Enu, Anaocha Local Govt, Anambra State. ANAMBRA 16 Adazi-Nnukwu Microfinance Bank Limited Unit Near Eke Market, Adazi Nnukwu, Adazi, Anambra State ANAMBRA 17 Addosser Microfinance Bank Limited State 32, Lewis Street, Lagos Island, Lagos State LAGOS 18 Adeyemi College Staff Microfinance Bank Ltd Unit Adeyemi College of Education Staff Ni 1, CMS Ltd Secretariat, Adeyemi College of Education, Ondo ONDO 19 Afekhafe Microfinance Bank Ltd Unit No. -

Niger Delta Budget Monitoring Group Mapping
CAPACITY BUILDING TRAINING ON COMMUNITY NEEDS ASSESSMENT & SHADOW BUDGETING NIGER DELTA BUDGET MONITORING GROUP MAPPING OF 2016 CAPITAL PROJECTS IN THE 2016 FGN BUDGET FOR ENUGU STATE (Kebetkache Training Group Work on Needs Assessment Working Document) DOCUMENT PREPARED BY NDEBUMOG HEADQUARTERS www.nigerdeltabudget.org ENUGU STATE FEDERAL MINISTRY OF EDUCATION UNIVERSAL BASIC EDUCATION (UBE) COMMISSION S/N PROJECT AMOUNT LGA FED. CONST. SEN. DIST. ZONE STATUS 1 Teaching and Learning 40,000,000 Enugu West South East New Materials in Selected Schools in Enugu West Senatorial District 2 Construction of a Block of 3 15,000,000 Udi Ezeagu/ Udi Enugu West South East New Classroom with VIP Office, Toilets and Furnishing at Community High School, Obioma, Udi LGA, Enugu State Total 55,000,000 FGGC ENUGU S/N PROJECT AMOUNT LGA FED. CONST. SEN. DIST. ZONE STATUS 1 Construction of Road Network 34,264,125 Enugu- North Enugu North/ Enugu East South East New Enugu South 2 Construction of Storey 145,795,243 Enugu-North Enugu North/ Enugu East South East New Building of 18 Classroom, Enugu South Examination Hall, 2 No. Semi Detached Twin Buildings 3 Purchase of 1 Coastal Bus 13,000,000 Enugu-North Enugu North/ Enugu East South East Enugu South 4 Completion of an 8-Room 66,428,132 Enugu-North Enugu North/ Enugu East South East New Storey Building Girls Hostel Enugu South and Construction of a Storey Building of Prep Room and Furnishing 5 Construction of Perimeter 15,002,484 Enugu-North Enugu North/ Enugu East South East New Fencing Enugu South 6 Purchase of one Mercedes 18,656,000 Enugu-North Enugu North/ Enugu East South East New Water Tanker of 11,000 Litres Enugu South Capacity Total 293,145,984 FGGC LEJJA S/N PROJECT AMOUNT LGA FED. -

NIGERIAN AGRICULTURAL JOURNAL ISSN: 0300-368X Volume 49 Number 2, October 2018
NIGERIAN AGRICULTURAL JOURNAL ISSN: 0300-368X Volume 49 Number 2, October 2018. Pp. 242-247 Available online at: http://www.ajol.info/index.php/naj EFFECT OF RURAL-URBAN MIGRATION ON RICE PRODUCTION IN ENUGU STATE, NIGERIA 1Apu, U., 1Okore, H.O., 2Nnamerenwa, G.C. and 1Gbede, O.A. 1Department of Rural Sociology and Extension; 2Department of Agricultural Economics, Michael Okpara University of Agriculture, Umudike, Abia State Corresponding Authors’ email: [email protected] ABSTRACT This study assessed the effect of rural-urban migration on rice production in Enugu State, Nigeria. Multi-stage and Purposive sampling procedure was used to select 60 respondents which constituted the sample size of the study. Data were obtained through the use of a structured questionnaire. Descriptive statistics such as frequency counts and percentages, and inferential statistics such as correlation and z-test procedure were employed for analyses of data. Findings indicated that majority of the respondents (81.67%) were at their youthful age of 16 to 45 years old. The highest household size obtained was between 4 and 9 persons per household. Majority of the respondents in the study area (53.33%) were small scale farmers and had below 6 hectares of rice farm land. Poor living conditions, low influx of income and lack of employment were the most important reasons for rural-urban migration as confirmed by the respondents in Enugu State (65.00%). In the study area, 62.68% migrated to the urban areas. A larger proportion of the respondents (60.00%) indicated that between 4 and 9 household members participated in the rice production activities. -

Reports on Inter-Religious Violence in Nigeria, Particularly in the South (Ibadan Etc )
Reports on Inter-religious violence in Nigeria, particularly in the South (Ibadan etc ) In a section titled Societal Abuses and Discrimination (Section III.) the US Department of State religious freedom report for Nigeria states: Tension between Christians and Muslims remained acute in some areas, and conflicts of a seemingly socioeconomic or political nature often divided people along religious lines. Events, particularly of a religious tenor, occurring in other regions of the country or parts of the world, heightened tensions between religious groups. Religious differences often exacerbated ethnic differences. Competition for scarce resources, in concert with unequal and discriminatory employment practices, provoked violence between individuals of different religious or ethnic communities. Religion was also often a catalyst for hostility, used by politicians and others to foment discord. (US Department of State (Bureau of Democracy, Human Rights, and Labor) (19 September 2008) Nigeria International Religious Freedom Report) The annual report published by the US Commission on International Religious Freedom refers to religious violence in Nigeria as follows: Since 1999, more than 10,000 Nigerians have been killed in sectarian and communal attacks and reprisals between Muslims and Christians. The most serious of these clashes occurred in Kaduna state (February and May 2000 and November 2002); Jos, Plateau state (September 2001); Kano state and Yelwa, Plateau state (February-May 2004); and in northern and southeastern Nigeria, in the wake of the controversy over depictions of the Prophet Muhammad in the Danish press in February 2006 (see below). Ethnic and religious violence continued throughout the past year, although the number of deaths resulting from the violence decreased compared to previous years. -

Landfill Site Selection for Solid Waste Management in Karu Lga, Nasarawa State, Nigeria
International Journal of Trend in Research and Development, Volume 3(6), ISSN: 2394-9333 www.ijtrd.com Landfill Site Selection for Solid Waste Management in Karu Lga, Nasarawa State, Nigeria Rakiat Ladi Haruna, Alaga T.A, Gajere E.N, Ukor Chioma and Amos S.I Cooperative Information Network (COPINE), NASRDA, National Centre For Remote Sensing (NCRA), Jos., Obafemi Awolowo University, Oau Campus, Ile- Ife, Nigeria Abstract: Solid waste disposal is a crucial problem in the urban and rural areas because most solid wastes are not dumped in the suitable areas. Karu LGA has the challenge of solid waste dumping site identification. The specific objectives of this study were to: map and identify the existing landfill site and dump sites in the study area and to identify potential suitable landfill site(s) in the study area. The main data used for this study were SRTM image with a spatial resolution of 30m spatial resolution, Landsat 8 OLI imagery, google earth imagery and ground control point (GCP) collected by ground point survey (GPS). The maps were prepared by overlay and suitability analysis of geographic information system (GIS), remote sensing techniques and multi criteria analysis methods. The potential suitability map was prepared by overlay analyses on Arc map and suitability levels as high, moderate, less suitable, and unsuitable sites of the study area were determined. The results indicate that 37.7% of the study area is unsuitable for solid waste dumping; 44.29% less suitable; 14.97% moderately suitable; and 3.0 % most suitable. The GIS and remote sensing techniques are important tools for solid waste site selection. -

Politics and Policies of Religious Broadcasting in Nigeria
Asonzeh Ukah1 Оригинални научни рад University of Bayreuth UDK: 316.77:2(669) ; 2-662:316.7(669) ; Germany 340.134:654.17/.19(669) BANISHING MIRACLES: POLITICS AND POLICIES OF RELIGIOUS BROADCASTING IN NIGERIA Abstract Nigeria is home to a vibrant media marketplace. Excluding more than a hundred ti- tles of daily tabloids and weekly newspapers, there is a densely saturated broadcast in- dustry consisting of radio, television (terrestrial, satellite, pay per view and cable chan- nels) and video-film in Nigeria. Since the deregulation of the broadcast industry in 1992 with the issuing of broadcast licences to individuals and groups, the country has witnessed a burgeoning growth such that at the beginning of 2008, there were about 284 broadcasting stations in Nigeria. Since then, more licenses have been approved and issued, indicating a further expansion in the industry. Focusing on the practices and policies of the National Broadcasting Commission (NBC) vis-à-vis religious broad- casting in a multi-religious society, this paper investigates the politics, policies and processes of regulating deregulation within the industry which have raised some con- troversies in recent times, particularly with reference to what the NBC calls “unverified miracles”. Key Words: Broadcasting, Television, Pentecostalism, Politics, Miracles, Deregula- tion. Introduction Since Nigeria received political Independence in 1960, all the Constitutions drafted and promulgated have guaranteed freedom of religious association, expression and practice.2 What the Constitutions have not granted citizens, in a straightforward, un- complicated manner, is freedom to own and operate a broadcast medium. In a multi- religious society such as Nigeria, the role of the state with respect to religious com- munication is critical.