Abdominal X Rays Made Easy: Abnormal Extraluminal Gas
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Risk Factors of Biliary Peritonitis Following T-Tube Removal- the Unsolved Problem
Jemds.com Original Research Article Risk Factors of Biliary Peritonitis following T-Tube Removal- The Unsolved Problem Partha Pratim Barua1, Devid Hazarika2, Khorshid Alom Hussain3 1Associate Professor, Department of Surgery, Fakhruddin Ali Ahmed Medical College, Barpeta, Assam, India. 2Assistant Professor, Department of Surgery, Assam Medical College, Dibrugarh, Assam, India. 3Registrar, Department of Surgery, Fakhruddin Ali Ahmed Medical College, Barpeta, Assam, India. ABSTRACT BACKGROUND Gall stone disease remains one of the most common problems leading to surgical Corresponding Author: intervention. About 15% of all gall stone disease patients have stones in the common Devid Hazarika, Gunjan’s Aparna Enclave, bile duct (choledocholithiasis). Open choledocholithotomy is still widely performed, Hatigarh Chariali, Geetanagar, particularly in centres without ERCP facilities. Though primary repair of the common Guwahati-781021, Assam, India. bile duct is possible, most surgeons prefer to drain the common bile duct with T-tube. E-mail: [email protected] This avoids pressure build up in the CBD in case of oedema around the ampulla of Vater in the immediate post-operative period. Normally, the T-tube is left for 14–20 DOI: 10.14260/jemds/2019/546 days in order to allow a fibrous tract to form around it. In absences of any distal obstruction, the T-tube is removed by gentle traction in the horizontal limb. In Financial or Other Competing Interests: None. majority of the cases no complications occur after tube removal. However, in some patients, biliary peritonitis occurs with varying severity. The aim of this study is to How to Cite This Article: find out if there are yet unrecognized factors that increases the risk of biliary Barua PP, Hazarika D, Hussain KA. -

Incidental Cholecystojejunal Fistula: a Rare Complication of Gall Stone Disease
MedCrave Online Journal of Surgery Case Report Open Access Incidental cholecystojejunal fistula: a rare complication of gall stone disease Abstract Volume 8 Issue 4 - 2020 Cholecystoenteric fistula is a rare complication of gallstone disease and difficult to diagnose Vipul K Srivastava,1 Shilpi Roy,1 Ramniwas preoperatively. Among Cholecystoenteric fistula, cholecystojejunal fistulae are even rarer Meena,2 Rahul Khanna2 and only a few case reports have been published on it. Here we report a case of a 60-year 1Resident, Department of General Surgery, Institute of Medical male patient with cholecystojejunal fistula diagnosed intraoperatively while performing Sciences, India laparoscopic cholecystectomy. Fundus of the gall bladder was found to be communicating 2Professor, Department of General Surgery, Institute of Medical with proximal jejunum. We conclude that in elderly patients if the ultrasonography shows Sciences, India features of contracted gall bladder in presence of large gall stones one should consider an option of getting a computed tomography scan done preoperatively. Correspondence: Dr. Ramniwas Meena, Professor Department of General Surgery, Institute of Medical Sciences Banaras Hindu University, Varanasi–221005, UP, India, Keywords: cholecystoenteric, cholecystojejunal, fistula, gall-stones, cholecystitis Tel +919935141697, Email Received: October 25, 2020 | Published: December 17, 2020 Introduction Cholecystoenteric fistula (CEF) was first described by Courvoisier in 1890. They are a rare complication of gallstone disease and are formed due to ongoing inflammation.1 They are bilioenteric type of Internal Biliary fistula which is rare to find. Preoperative diagnosis of CEF is difficult to make with pneumobilia being the most common radiological finding.2 So here we report a rare case of cholecystojejunal fistula. -

Spontaneous External Biliary Fistula Uncomplicated by Gallstones B.R.P
Postgrad Med J: first published as 10.1136/pgmj.67.786.391 on 1 April 1991. Downloaded from Postgrad Med J (1991) 67, 391 - 392 i) The Fellowship of Postgraduate Medicine, 1991 Spontaneous external biliary fistula uncomplicated by gallstones B.R.P. Birch and S.J. Cox Department ofSurgery, Watford General Hospital, Vicarage Road, Watford, Hertfordshire, UK Summary: External biliary fistulae are rare. Only 65 cases have been reported in the literature and in each instance gallstones were a complicating factor. We report in this paper the first case of spontaneous external (cholecystocutaneous) biliary fistula uncomplicated by gallstones. Introduction External biliary fistulae, first described by Thilesus The necrotic area of the abdominal wall was in 1670 and common in the last century, have initially debrided under local anaesthesia with become rare since the advent of modern biliary antibiotic cover. The patient subsequently became surgery. There have been just 65 cases recorded apyrexial and was transfused to correct her since 19001,'2 and all of these were complicated by anaemia. gallstones. We report here the first case of spon- Four days after debridement the patient was taneous external biliary fistula in which gallstones returned to theatre for examination under anaes- were not a complicating factor. thetic. This showed there was a very narrow fistula communicating intra-abdominally. A decision was copyright. made to proceed to laparotomy. An incision was Case report made encompassing all necrotic tissues on the abdominal wall and the fistula was seen to be A 79 year old woman was admitted with a painful communicating with the fundus of the gallbladder, mass in the right upper quadrant ofher abdominal which was adherent to the anterior abdominal wall. -

The British Society of Gastroenterology
Gut: first published as 10.1136/gut.19.5.A432 on 1 May 1978. Downloaded from Gut, 1978, 19, A432-A458 The British Society of Gastroenterology The Spring Meeting of the BSG, together with the BSDE, took place at Warwick University, Coventry, from 31 March to 1 April. The meeting was largely given up to parallel sessions of scientific communications, abstracts of which appear below. During the proceedings, the President of the BSG, Dr. W. Sircus, presented Dr. D. B. Silk with the Research Medal for 1977-8: Dr. Silk later addressed the Society on 'Peptide transport in the human small intestine'. A varied social programme included a medieval banquet in Warwick Castle. R. FERGUSON AND MICHAEL ATKINSON recently managed three patients who bled ENDOSCOPY (General Hospital, Nottingham) In 43 from an angiomatous lesion of the patients (mean age 67 years) with benign gastric antrum. Each patient presented Disinfection of upper gastrointestinal fibre- oesophageal stricture caused by gastro- with a profound iron deficiency anaemia optic equipment oesophageal reflux, after initial dilatation due to persistent gastrointestinal blood by the Eder Puestow method, active loss. Barium studies of the upper and D. L. CARR-LOCKE AND P. CLAYTON medical measures were instituted. lower gastrointestinal tract failed to (Area Endoscopy Unit and Department of Ten subjects have not required further demonstrate the cause for the bleeding. Microbiology, Leicester General Hospital, dilatation after periods ranging from Gastroscopy in each patient demonstrated Leicester) As there is little information three months to three years, and 27 a striking antral abnormality consisting of available on the bacteriological con- have needed further dilatation. -

Management of Postoperative Biliary Fistula After Hydatid Liver Surgery
arch and se D e e v R f e l o o l p a m n r e Gokhan et al., J Res Development 2016, 4:1 n u t o Journal of Research and Development J DOI: 10.4172/2311-3278.1000140 ISSN: 2311-3278 Research Article Open Access Management of Postoperative Biliary Fistula After Hydatid Liver Surgery: Are There Any Differences between Localizations? Gokhan A1, Ali K1, Bora K2, Soykan A3, Mustafa K1, Emin G2, Halil A1, Servet K2, Sebahattin C4* and Özgür K4 1Department of Surgery, Bakırkoy Dr. Sadi Konuk Training and Research Hospital, Istanbul 2Department of Surgery, Okmeydani Training and Research Hospital, Istanbul 3Department of Surgery, Istanbul Training and Research Hospital, Istanbul 4Department of Surgery, Yüzüncü Yıl University Medical Faculty, Turkey *Corresponding author: Sebahattin Celik, Department of General Surgery, Yüzüncü Yıl University Faculty of Medicine Van, Turkey; Tel: +90 505 705 79 57; E-mail: [email protected] Rec date: Jan 24, 2016; Acc date: Mar 04, 2016; Pub date: Mar 15, 2016 Copyright: © 2016 Gokhan et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited. Abstract Objectives The most common complication of hepatic hydatid cysts is the intra-biliary rupture seen approximately in 10-30% of patients. This complication mainly seen in the centrally localized, large hydatid cyst operations. The aim of this study is to compare managements of postoperative biliary fistula after hydatid liver surgery, according to localization of hepatic cyst. -

Stone Ileus: an Unusual Presentation of Crohn's Disease
Ma, et al. Int J Surg Res Pract 2016, 3:046 International Journal of Volume 3 | Issue 2 ISSN: 2378-3397 Surgery Research and Practice Case Report: Open Access Stone Ileus: An Unusual Presentation of Crohn’s Disease Charles Ma and H Tracy Davido Department of Critical Care and Acute Care Surgery, University of Minnesota Health, USA *Corresponding author: H Tracy Davido MD, Assistant Professor of Surgery, Department of Critical Care and Acute Care Surgery, University of Minnesota Health, 11-115A Phillips Wangensteen Building, 420 Delaware St. SE, MMC 195, Minneapolis, MN 55455, USA, Tel: 612-626-6441, E-mail: [email protected] Introduction Case Report Stone ileus, also known as enterolith ileus enterolithiaisis, is a rare A 67-year-old morbidly obese woman came to the emergency complication of cholelithiasis and an even rarer symptom of Crohn’s department at our institution with an upper respiratory infection, disease. Gallstone ileus is secondary to fistula formation between decreased appetite, and malaise. Her past medical history was the gallbladder and the gastrointestinal (GI) system. Enterolithiasis significant for an open cholecystectomy more than 30 years earlier. of Crohn’s disease is thought to arise from the stasis of succus She had no additional past surgical history or diagnoses. The initial within the small bowel eventually leading to stone formation and workup revealed acute renal failure, with significant electrolyte growth. Both gallstone ileus and enterolithiasis of Crohn’s disease abnormalities and dehydration. She underwent intravenous fluid can result in subsequent mechanical bowel obstruction. Gallstone resuscitation and electrolyte replacement in the Medical Intensive ileus accounts for 1% to 4% of mechanical bowel obstructions, with Care Unit; however, while hospitalized, she developed new-onset higher a incidence in women over age 60 [1]. -

Type IV Mirizzi Syndrome Treated with Hepaticoduodenostomy and Minilaparoscopy
CASE REPORT Type IV Mirizzi Syndrome Treated with Hepaticoduodenostomy and Minilaparoscopy Gustavo Lopes de Carvalho, MD, PhD, Gilberto Fernandes Silva de Abreu, MD, MSc, Diego Laurentino Lima, MD, Gustavo Henrique Belarmino de Go´es, Medical Student Faculty of Medical Sciences (all authors) and University of Pernambuco (UPE), Recife, Brazil (Dr. Carvalho). ABSTRACT Introduction: Mirizzi syndrome (MS) is an uncommon complication of long-term chronic cholecystitis, characterized by extrinsic compression of the common hepatic duct or the presence of cholecystobiliary fistula. A case of type IV MS, with extensively damaged common hepatic duct (CHD) due to gallstone impaction and fistula, was effectively treated by minilaparoscopic hepaticoduodenostomy (HD). Case Description: The patient was a woman, 36 years old, weighing 66 kg, and standing 1.55 m. For 3 weeks, she had been experiencing episodes of strong right-upper-quadrant pain, radiating to the back. She also presented with choluria, fecal acholia, and severe jaundice. Preoperative magnetic resonance cholangiopancreatography (MRCP) suggested the diagnosis of Mirizzi syndrome (MS). Surgery started with “dome-down” dissection of the gallbladder. The cystic duct and the CHD were found to be highly compromised close to the gallstone impacted in the infundibulum. After resection of the affected bile ducts, the biliary tract reconstruction was performed by minilaparoscopy (MINI). The patient was discharged uneventfully 6 days after surgery, without complication. Discussion: Because of the severely compromised CHD, HD was the technique used for reconstruction, for its simple execution, and several proven advantages over hepaticojejunostomy. It was performed by MINI, a new, effective, and refined minimally invasive technique in which the surgeon uses low-friction trocars to improve visualization and dexterity in delicate surgical tasks. -

Early Biliary Complications Following Pancreaticoduodenectomy: Prevalence and Risk Factors
http://dx.doi.org/10.1016/j.hpb.2015.10.012 HPB ORIGINAL ARTICLE Early biliary complications following pancreaticoduodenectomy: prevalence and risk factors Brice Malgras1, Sandrine Duron2, Sébastien Gaujoux1,Safi Dokmak1, Béatrice Aussilhou1, Vinciane Rebours3, Maxime Palazzo3, Jacques Belghiti1 & Alain Sauvanet1 1Department of Hepato-Pancreato-Biliary Surgery, Pôle des Maladies de l’Appareil Digestif (PMAD), AP-HP, Hôpital Beaujon, Université Paris Diderot, Paris, France Clichy, 92110, 2French Armed Forces Center for Epidemiology and Public Health, Marseille, and 3Departement of Pancreatology, Pôle des Maladies de l’Appareil Digestif (PMAD), AP-HP, Hôpital Beaujon, Université Paris Diderot, Paris, France Clichy, 92110, France Abstract Background: Early biliary complications (EBC) following pancreaticoduodenectomy (PD) are poorly known. This study aimed to assess incidence, predictive factors, and treatment of EBC including bilio- enteric stricture, transient jaundice, biliary leak, and cholangitis. Method: From 2007 to 2011, 352 patients underwent PD. Statistical analysis including logistic regression was performed to determine EBC predictive factors. Results: 49 patients (14%) developed 51 EBC, including 7(2%) bilio-enteric strictures, 15(4%) transient jaundices, 9(3%) biliary leaks, and 20(6%) cholangitis with no mortality and a 18% reoperation rate. In multivariate analysis, male gender, benign disease, malignancy with preoperative chemoradiation, and common bile duct (CBD) diameter 5 mm were predictive of EBC. Of the 7 strictures, all were associated with CBD 5 mm and 5(71%) required reoperation. Transient jaundice resolved spontaneously in all 15 cases. Among 8 patients with serum bilirubin level >50 mmol/L (3 mg/dL) at POD3, 7(88%) developed bilio-enteric stricture. Biliary leak resolved spontaneously in 5(56%); otherwise, it required reoperation. -

Colo-Cystic Duct Fistula: an Unknown Complication of Colonic Diverticular Disease
Elmer ress Case Report J Med Cases. 2015;6(5):214-215 Colo-Cystic Duct Fistula: An Unknown Complication of Colonic Diverticular Disease Lakshmi Kant Pathaka, c, Vimala Vijayaraghavanb Abstract Case Report Enterobiliary fistula is a complication of gall stones and gall bladder History of present illness disease. Diverticular diseases are known for fistulous complication but enterobiliary fistula as a complication is unknown. This case pre- sents a patient with diverticular disease with lower gastro-intestinal The patient is an 82-year-old male who presented with four bleed who was found to have a colo-cystic duct fistula at surgery. episodes of hematochezia described as dark red blood in the stool. He did not have any nausea, vomiting or abdominal pain. Keywords: Colo-cystic fistula; Diverticulosis; Entero-biliary fistula The patient had two similar episodes in the past, one 3 years and another 5 years before the current episode. Introduction Past medical history Spontaneous enterobiliary fistulas (EBFs) are a complication The past medical history included peripheral neuropathy, hy- of biliary disease or a disease of adjacent structures. They are pertension, coronary artery disease, bladder cancer, abdominal usually associated with gallstones, but have also been reported aortic aneurysm repair and hypothyroidism. with peptic ulcer disease, abdominal trauma, Crohn’s disease, and malignancies of the biliary tract, bowel, and head of the pancreas [1]. Communication can occur between the gallblad- Hospital course der or biliary system and the stomach, small intestine, or colon. Although the incidence of such fistulas is unknown, autopsy On admission, his vitals were stable and a physical examina- studies estimate it as less than 1%. -

Spontaneous Internal Biliary Fistulae
Gut: first published as 10.1136/gut.5.5.429 on 1 October 1964. Downloaded from Gut, 1964, 5, 429 Spontaneous internal biliary fistulae J. L. A. DOWSE From Llandough Hospital, near Cardiff EDITORIAL SYNOPSIS This paper provides a comprehensive account of the various types of spon- taneous internal biliary fistulae and emphasizes the importance of chronic gall bladder disease in the aetiology. Air in the biliary tree is an important radiological sign. Early diagnosis and treatment of chronic cholelithiasis may prevent this complication. The gall bladder lies on the under surface of the through the cavity of the gall bladder. The cases liver, and is held in position by areolar tissue and the recorded by Faber are extremely unusual; of 13 peritoneum covering the under surface of the liver. gall stones, 'nine small and four large' voided in the It lies obliquely, its long axis being directed back- urine 'without any symptoms of a remarkable wards and upwards and slightly medially from the nature except pains in the bladder'; of a fistula lower anterior edge of the liver, to the right end of between the gall bladder and pregnant uterus, with the porta hepatis. The fundus of the gall bladder is the passage of gall stones during labour; of fistulous in close relation to the anterior abdominal wall. connexions between the gall bladder and portal vein, The transverse colon is closely related to the inferior 'so that the vein has been filled entirely with stones' surface of the fundus and body of the gall bladder, (Frerichs, 1861). Infections and injury of the biliary and the pylorus and first part of the duodenum lie tract have caused extravasation of bile into the below the neck of the gall bladder and cystic duct. -

Cholecystocolonic Fistula: Facts and Myths. a Review of the 231
J Hepatobiliary Pancreat Surg (2009) 16:8–18 DOI 10.1007/s00534-008-0014-1 REVIEW ARTICLE Cholecystocolonic fistula: facts and myths. A review of the 231 published cases Renato Costi Æ Bruto Randone Æ Vincenzo Violi Æ Olivier Scatton Æ Leopoldo Sarli Æ Olivier Soubrane Æ Bertrand Dousset Æ Thierry Montariol Received: 19 March 2008 / Accepted: 28 April 2008 / Published online: 17 December 2008 Ó Springer 2008 Abstract Resolution of colonic biliary ileus by interventional Background Cholecystocolonic fistula (CCF) is the sec- endoscopy is reported. ond most common cholecystoenteric fistula and is often Conclusion CCF should be considered in differential discovered intraoperatively, resulting in a challenging sit- diagnosis of diarrhea, especially in old, female patients. A uation for the surgeon, who is forced to switch to a possible second hepatobiliary abnormality should be complex procedure, often in old, unfit patients. Manage- always investigated. Extemporaneous frozen section ment of this uncommon but possible finding is still ill should be performed if gallbladder cancer is suspected. defined. Depending on clinical presentation, different treatments for Methods An extensive review of 160 articles published CCF are indicated, ranging from minimally invasive pro- from 1950 to 2006 concerning 231 cases of CCF was cedures to extensive resection. performed. Results CCF is mostly an affliction of women in their Keywords Cholecystocolonic fistula Á Biliary ileus Á sixth to seventh decades and is rarely diagnosed preoper- Diagnosis Á Treatment Á Laparoscopy atively. Chronic diarrhea is the key symptom in nonemergency patients, but, in one-fourth of cases, CCF presents with an acute onset, mostly biliary ileus. -
Gallbladder-Appendicular Fistula
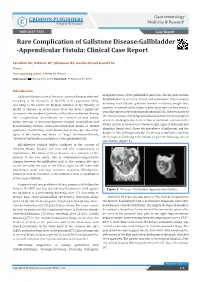
Gastro Med Res Gastroenterology Copyright © Mikheev IO CRIMSON PUBLISHERS C Wings to the Research Medicine & Research ISSN 2637-7632 Case Report Rare Complication of Gallstone Disease:Gallbladder -Appendicular Fistula: Clinical Case Report Yareshko NO, Mikheev IO*, Shabanov NA, Barska KS and Kanaki AV Ukraine *Corresponding author: Mikheev IO, Ukraine Submission: February 02, 2019; Published: February 07, 2019 Introduction malignant tumor of the gallbladder, pancreas, chronic pancreatitis. Gallstone disease is one of the most common diseases detected, Established more accurate clinical and anamnestic characteristics according to the literature, in 10-15% of the population [1-5]. According to the Center for Medical Statistics of the Ministry of of biliary tract fistulas: gallstone disease in history, weight loss, increase in the number of patients with Gallstone disease. Among jaundice, recurrent chills, bouts of pain up to three to four times a Health of Ukraine, in recent years there has been a significant rare complications cholelithiasis are isolated external biliary year, discomfort in the right hypochondrium [3,4]. The peculiarity of the clinical course of biliodigestive fistulas is intermittent symptom biliary system, as well as loss of body weight, signs of dyspepsy, and of severe cholangitis due to the reflux of intestinal contents in the fistula, internal or cholecystodigestive fistulas, torakobiliary and syndrome, cholelithiasis small bowel obstruction, but also other bronchobiliary fistulas, cholecystocholedoheal fistula or Mirizzi abundant liquid stool. Given the prevalence of gallstones and the danger of this, although rare, but it’s serious complication, such as types of bile fistula and micro or “large” choledocholithiasis, the formation of biliodigestive fistula, we give the following clinical “wrinkled” gallbladder, calcification of the gallbladder [6].